
Translate this page into:
Lipomatous meningioma: A rare subtype of benign metaplastic meningiomas
Address for correspondence: Dr. Mehmet Sabri Gürbüz, Yıldıztepe Mahallesi Bağcılar Cadesi No: 108, Bağcılar 34203, Istanbul, Turkey. E-mail: mehmetsabrigurbuz@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Lipomatous meningiomas are extremely rare subtypes of benign meningiomas and are classified as metaplastic meningioma in the World Health Organization classification. We present a 77-year-old man presented with the history of a gradually intensifying headache for the last 3 months. A right frontoparietal mass was detected on his cranial magnetic resonance imaging. The patient was operated on via a right frontoparietal craniotomy, and histopathological diagnosis was lipomatous meningioma. Distinctive characteristics of lipomatous meningiomas were discussed with special emphasis to importance of immunohistochemical examinations, particularly for its differentiation from the tumors showing similar histology though having more aggressive character.
Keywords
Differential diagnosis
histopathological diagnosis
lipoblastic meningioma

Introduction
Meningiomas make up about 15% of intracranial mass lesions. Meningiomas derive from arachnoid cap cells and most frequently occur in association with cerebral meninges. They account for approximately 20% of primary brain and spinal cord tumors.[12]
Metaplastic meningioma is a rare subtype of benign meningiomas, characterized by the presence of mesenchymal components.[3] Lipomatous meningioma is even a rarer variant with the presence of fat within meningioma cells, leading to a particular challenge in histopathological diagnosis.[45] It should be identified whether this is a result of a fat storage or component of a metaplastic process. A thorough immunohistochemical workup should be completed to differentiate it from other fat-containing tumors, such as liposarcomas, lipomas, epidermoid and dermoid tumors, chordomas, and metastatic mucinous carcinomas, since each has a different treatment strategy and prognosis.[35]
In this report, we present a 77-year-old man operated on for a right frontoparietal mass and diagnosed with lipomatous meningioma. Distinctive characteristics of this rare type of benign meningioma were discussed under the light of the current literature, with special emphasis to importance of further immunohistochemical examinations for its differentiation from more aggressive tumors that may show similar histology.
Case Report
A 77-year-old man was admitted to our clinic with the complaint of gradually increasing headache for the last 3 months. Physical and neurological examinations were unremarkable. Contrast-enhanced magnetic resonance imaging scan showed a well-enhanced extra-axial mass lesion in the right frontoparietal region with surrounding edema [Figure 1a–c]. The patient was operated on via a right frontoparietal craniotomy, and total tumoral excision was achieved. Postoperative cranial computed tomography scan revealed tumor removal with normal postoperative changes and persisting preexisting perilesional edema [Figure 2].
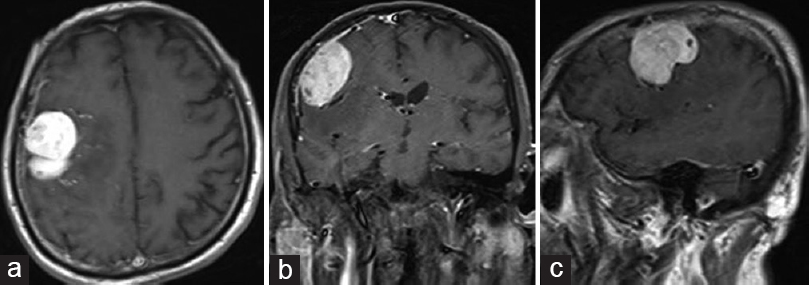
- (a) Preoperative T1-weighted contrast-enhanced axial cranial magnetic resonance imaging showing a right frontoparietal mass lesion and perilesional edema. (b) Preoperative T1-weighted contrast-enhanced coronal cranial magnetic resonance imaging showing a right frontoparietal mass lesion and perilesional edema. (c) Preoperative T1-weighted contrast-enhanced sagittal cranial magnetic resonance imaging showing a right frontoparietal mass lesion and perilesional edema
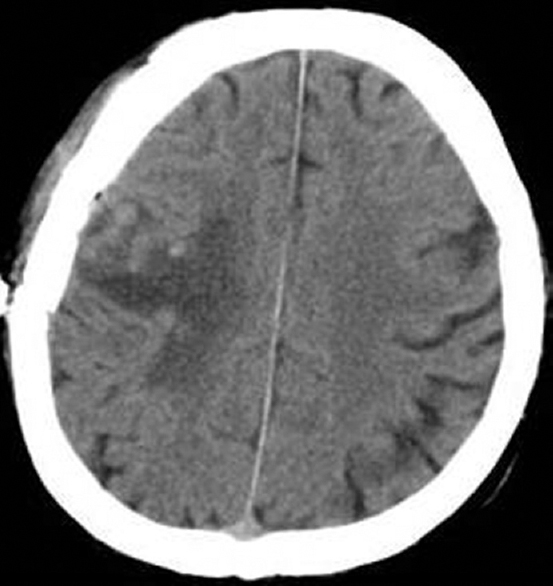
- Postoperative axial cranial computed tomography image showing tumor removal with normal postoperative changes and persisting preexisting perilesional edema
Pathological examination revealed a highly vascularized tumor consisting of typical meningotheliomatous meningioma cells mixed with mature adipose tissue. Tumor tissue contained large cells seeming as fat-like proliferation with classic meningothelial neoplastic cells. Tumoral cells had round nuclei and fat vacuoles in their cytoplasms. Immunohistochemical coexpression of epithelial membrane antigen (EMA), vimentin, and progesterone supported the meningothelial origin of tumor cells. On the other hand, tumor was negative for glial fibrillary acidic protein (GFAP) and S-100. Tumor cells had low proliferation capacity with 1–2% of Ki-67 positivity. Histopathological diagnosis was lipomatous meningioma [Figure 3a–d].
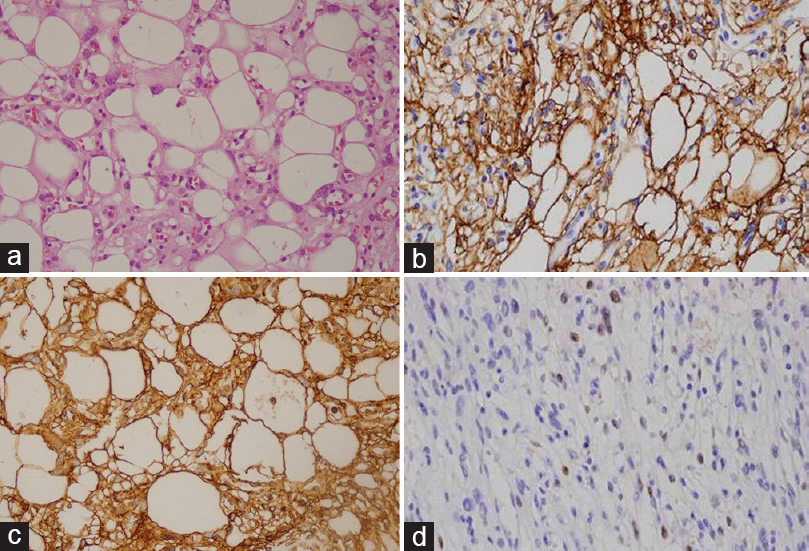
- (a) Tumor tissue containing large cells seeming as fat-like proliferation with classic meningothelial neoplastic cells. Tumor cells have round nuclei and fat vacuoles in their cytoplasms (H and E, ×40). (b) Tumor tissue showing the expression of epithelial membrane antigen (EMA, ×40). (c) Tumor tissue showing positive staining with vimentin (Vimentin, ×40). (d) Tumor tissue showing the expression of progesterone receptor (PR, ×200)
Postoperative period was uneventful and the patient was discharged from the hospital on the 5th day of operation, with no neurological deficit.
Discussion
Meningiomas are the most common extra-axial central nervous system tumors and constitute 15–30% of all intracranial tumors. They are benign, slow-growing lesions and usually appear in the middle to late adulthood and more frequently in women.[12] Meningiomas are classified into three groups according to the World Health Organization (WHO) grading system: benign meningiomas (WHO Grade I), atypical meningiomas (WHO Grade II), and malignant meningiomas (WHO Grade III).[67]
Metaplastic meningioma is a rare subtype of WHO Grade I meningiomas, histologically characterized by the presence of so-called “metaplastic changes” involving mesenchymal components, such as osseous, cartilaginous, lipomatous, and myxoid tissue.[5] The pluripotent mesenchymal cells that give rise to the development of meningiomas may transform into other cell types. An example of this process is metaplastic differentiation of meningothelial cells into mature adipocytes.[3] Metaplastic differentiation usually occurs in meningothelial, transitional, and fibrous subtypes of meningiomas. Metaplasia may involve almost all mesenchymal components, including osseous, cartilaginous, lipomatous, and myxoid tissue. This is a consequent of mesenchymal and neuroectodermal differentiation of pluripotent arachnoid cap cells.[89]
Lipomatous meningiomas are rare subtypes of meningiomas first described by Bailey and Bucy in 1931.[10] The terms “lipomatous” or “lipoblastic” represent the cells found in meningiomas resembling adipocytes. If the mature adipocytes are widely available in the tumor, this is considered a metaplastic change and called lipomatous or lipoblastic.[411] If it is a simple fat storage phenomenon as in the xanthomatous variant, the term “lipidized” is considered more suitable for it.[3] Our case revealed meningotheliomatous cells with widely available adipocytes prompting the histological diagnosis of lipomatous meningioma.
Lipomatous meningioma shows positive reactivity for vimentin and EMA and negative reactivity for GFAP in immunohistochemical staining. Their positive reactivity for vimentin and EMA represents their dual mesenchymal and epithelial characteristics.[356] In our case, expressions of EMA, vimentin, and progesterone and negative GFAP reactivity were suggesting meningioma. Negative reactivity of adipocytes to S-100 suggests that the adipocytes observed in our case were the products of a metaplastic process rather than true adipocytes.[612] In parallel with recent literature, these immunohistochemical characteristics suggest that the presence of lipid accumulation in meningioma might be considered a transformation of meningothelial cells rather than a true metaplasia.[4512]
Differentiation of lipomatous meningioma from lipidized meningiomas has been considered of no prognostic value.[11] Similarly, Lattes and Bigotti reported no recurrence in their series including seven cases and pointed out that lipomatous meningioma behaves analogous to the biologic course of ordinary meningiomas.[9] However, it is crucial to differentiate lipomatous meningioma from the tumors that show similar histology but differ in treatment and prognosis. Consequently, lipomatous meningioma should be differentiated from fat-containing tumors such as liposarcoma, lipoma, epidermoid and dermoid tumors, chordomas, and metastatic mucinous carcinomas through further immunohistochemical investigation.
In conclusion, lipomatous meningioma is a very rare subtype of metaplastic meningioma and requires differentiation from the tumors associated with lipid accumulation. Further immunohistochemical examinations are of great importance for accurate histopathological diagnosis of lipomatous meningiomas since other fat-containing tumors may show similar histology though having more aggressive character.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Clinicopathological analysis of metaplastic meningioma: report of 15 cases in Huashan Hospital. Chin J Cancer Res. 2013;25:112-8.
- [Google Scholar]
- Lipomatous meningioma: a clinicopathologic study of 18 cases with special reference to the issue of metaplasia. Am J Surg Pathol. 2001;25:769-75.
- [Google Scholar]
- Meningiomas. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, eds. WHO Classification of Tumours of the Central Nervous System. Lyon: IARC Press; 2007. p. :164-72.
- [Google Scholar]
- Lipomatous meningioma: Report of a case and a diagnostic pitfall. Turk Neurosurg. 2006;16:40-3.
- [Google Scholar]
- Lipomatous meningioma: report of 2 cases and review of the literature. Surg Neurol. 2008;69:398-402.
- [Google Scholar]




