
Translate this page into:
An Analytical Study to Correlate Serum Levels of Levetiracetam with Clinical Course in Patients with Epilepsy
Address for correspondence: Dr. Varun Gupta, 6, Sood Enclave, Dugri Dhandra Road, Ludhiana - 141 013, Punjab, India. E-mail: varun8085@yahoo.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
With the advancement of therapeutics, newer antiepileptic drugs (AEDs) like Levetiracetam (LEV), with good therapeutic efficacy and tolerability are available. But unfortunately, therapeutic drug monitoring is not routinely done in India for these drugs.
Objectives:
The objective of this study is to determine the range of serum levels of LEV in patients at stabilized doses and correlate them with their clinical course.
Materials and Methods:
Patients with epilepsy and started on LEV were enrolled from the Neurology Department after the Ethics Committee approval. Serum levels of LEV were estimated using high-performance liquid chromatography and correlated with patient demographics, dosage, dosage forms, concomitant AEDs, compliance of the patient, therapeutic effect, adverse drug reactions (ADRs), and suspected toxicity.
Results:
Serum levels of LEV ranged from 0.4 to 102.2 μg/ml at different time points and demonstrated a negligible positive correlation with age of the patients (r = 0.12) but negligible negative correlation with bodyweight (r = −0.19). No conclusive relationship could be established for dose, gender, dosage forms, clinical efficacy (seizure frequency), ADRs, and toxicity. Compliance was verified in all the patients. Levels were found to reduce with the use of concomitant enzyme inducer drugs (56.78%) whereas increase with valproic acid (7.8%).
Conclusion:
These findings emphasize the need for monitoring the serum levels of newer AEDs like LEV considering the various parameters studied here, so as to maintain the therapeutic efficacy by preventing under or over dosage and to generate a broader database of serum levels of LEV in the Indian population to help appropriate prescribing with more confidence.
Keywords
Drug monitoring
epilepsy
high-performance liquid chromatography
seizures

INTRODUCTION
Therapeutic drug monitoring (TDM) of antiepileptic drugs (AEDs) is a common practice and is usually done to optimize their dosing regimens, efficacy and in investigating therapeutic failure or patient compliance and avoid toxicity. TDM of these drugs is considered necessary because of many reasons. As seizures occur irregularly, sometimes with long gaps in between the episodes, long-term administration and therefore observation of AED therapy becomes necessary to assess the patient compliance and its clinical benefit. Some AEDs produce adverse effects which are difficult to distinguish from underlying neurologic disease and finally, there are no laboratory tests or diagnostic procedures available that can easily assess the clinical efficacy of the AEDs. Patient demographics such as age, gender, and bodyweight play a key role in the pharmacokinetic variability of these drugs. Measuring serum levels is also indicated in patients with conditions such as hepatic or renal impairment and pregnancy which alter their pharmacokinetic characteristics so as to maintain there effective drug levels.[12345]
On the other hand, it is also a fact that if pharmacokinetic parameters of a drug are consistent and predictable, then dosing of that drug can often be done without the need for TDM which is usually seen with newer AEDs. Levetiracetam (LEV) is one of the newer AED which became available in the year 2000. Although there exists a linear relationship between the dose and the serum levels of LEV, some studies have suggested that serum levels of LEV can get affected by a number of parameters.[6] Therefore, effective serum levels for LEV are not well known. Reference ranges (levels) for the newer AEDs like LEV have been difficult to establish. Ideally, TDM guides physicians toward that serum concentration of the drug which would optimize the seizure control, while avoiding or at least minimizing their toxic effects. However, it has been seen that a particular individual may show a good clinical response at AED concentrations even outside the reference range for that drug.
Based on this understanding, serum levels of LEV were measured and correlated with the patient's demographics and clinical response, based on the assumption that the clinical effects for certain diseases correlate better with drug concentrations than with the dose given. While TDM is an established method to individualize the dosage of AEDs since many years, its impact on clinical course in patients with epilepsy has rarely been assessed especially with new AEDs in a systematic manner.[2]
MATERIALS AND METHODS
The study is reported according to STROBE guidelines for observational studies. Patients suffering from epilepsy (any seizure semiology) and started on LEV were enrolled for the study, after obtaining their written informed consent, from the outpatient Department of Neurology of a tertiary care Medical College and Hospital of North India from July 1, 2014 to August 31, 2015, after approval from Institutional Ethics Committee. As this was a pilot study, 31 patients above 18 years of age and started on LEV were selected but only 29 completed the study [Figure 1]. Patients who were pregnant, having a history of renal insufficiency, liver disease, or any other comorbid condition were excluded. No efforts were made to alter the treatment course as part of the study.

- Flow chart of patient recruitment
Patient demographics such as age, gender, height, and bodyweight along with clinical characteristics such as seizure frequency, detailed history of AEDs intake both past and present and other concomitant treatment received were recorded. The blood samples of these patients were collected for estimation of serum levels of LEV (after dose stabilization), creatinine, alanine transaminase (ALT), aspartate transaminase (AST), and albumin. The timing of sample collection and last dose taken were also recorded. Serum levels of LEV in these patients were measured using Shimadzu's high-performance liquid chromatography (HPLC) system (LC-2010 AHT/CHT). C18 column was used as stationary phase and triethylamine buffer (10 ml triethylamine in 1000 ml water) adjusted to pH 6.5 ± 0.2 by phosphoric acid and acetonitrile in the ratio of 85:15 respectively was used as mobile phase. All chemicals were HPLC grade and procured from Sigma-Aldrich. Flow rate of the mobile phase was 0.8 ml/min with a run time of 8 min. Oven temperature was 25°C Celsius. Chromatograph was read at 205-nanometer wavelength using ultraviolet detector. Unknown patient serum samples were run against the standard calibration curve of LEV prepared which was linear with a correlation coefficient (r) of 0.999. The limit of detection and quantification of this assay method were 0.01 and 0.03 µg/ml, respectively.
Descriptive statistics were used in making an analysis on Microsoft Excel. The determined serum levels of LEV were correlated with age, gender, bodyweight, dose used, formulation, compliance, therapeutic effect, suspected toxicity, suspected drug interactions, and adverse drug reactions (ADRs) in the patients.
RESULTS
Figure 1 shows the recruitment of patients in a flow chart. Among the 29 patients who were included in the study, 15 were males and 14 were females. Most of the patients belong to the age group of 18–35 years. Table 1 shows the demographic characteristics of these patients. Serum levels of creatinine, ALT, AST, and albumin were within normal ranges for these patients. Other than LEV, patients were also on clobazam, valproic acid (VA), oxcarbazepine, carbamazepine, phenytoin, phenobarbitone, lamotrigine, and topiramate in various combinations.

The mean dose given to the patients in the study was 26.45 ± 10.76 mg/kg/day with a range of 7.57–50.00 mg/kg/day whereas the median total daily dose of LEV given was 1500 mg (range 500–4000 mg). The median serum level of LEV obtained at different time intervals from the drug intake and blood sampling was 17.8 µg/ml with a range of 0.4–102.2 µg/ml as shown in Table 2. Figure 2 illustrates the range of serum LEV concentration at total dose given per day in milligrams. It shows that there is no increase in the serum LEV levels with an increase in doses. Figure 3 shows the distribution of serum LEV levels of patients versus time gap since blood sample collection after the last dose in semi-logarithmic scale. The levels show no relationship with the time of sample collection. Table 3 shows the serum LEV levels with respect to age, gender, bodyweight and formulation. For making comparisons, patients with similar doses and blood sampling time since the last dose were taken. For comparing the effects of age and bodyweight, patients were divided into below and above 40 years of age and 60 kg bodyweight, respectively. Correlation (r) between serum LEV concentration with dose administered (mg/kg/day), age and bodyweight were found out to be −0.04, 0.12, and −0.19. All patients were on LEV tablets except one each (elderly at 73 and 65 years age) on syrup and intravenous injection.

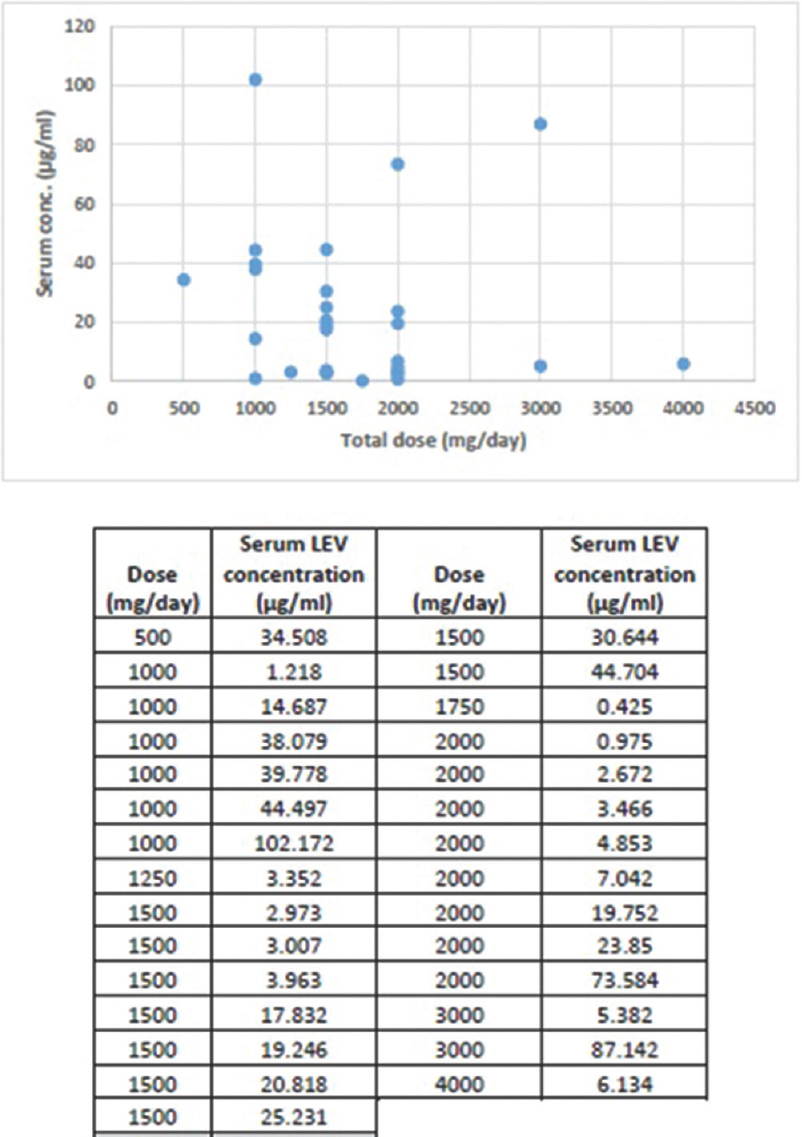
- Total levetiracetam dose versus serum concentration
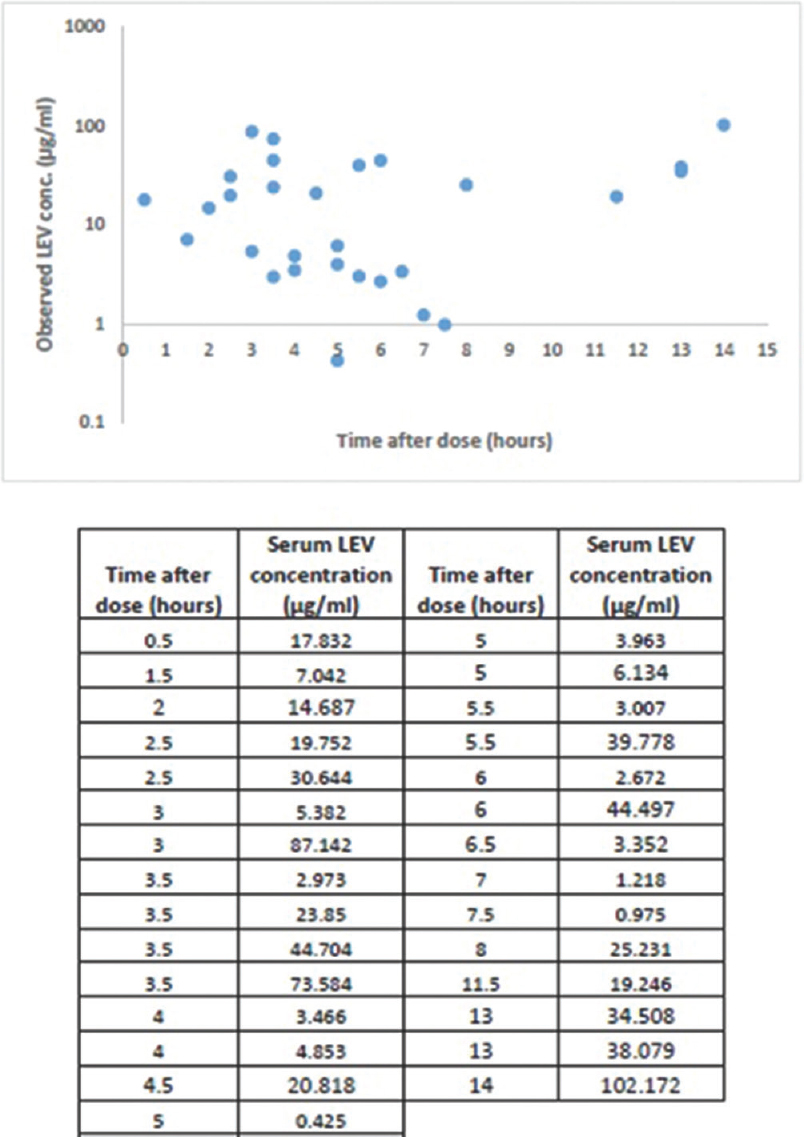
- Levetiracetam concentration versus time

All patients were compliant as they had detectable levels of LEV in their serum but whether they were strictly adherent to drug therapy cannot be commented upon as the levels show wide variations. 22 out of 29 (75.86%) patients showed >50% reduction in seizure frequency/week out of which 18 were completely seizure free. Two showed 50% reduction, three showed no change, and one showed 50% increase in seizure frequency/week as shown in Figure 4. The patient with increased frequency of seizure episodes was suffering from absence seizures and was diagnosed with bilateral temporal lobe due to epilepsy. One patient suffered from frequent oral twitching due to post hypoxic brain injury, but there was no record of the frequency of these twitchings. Table 4 shows serum LEV concentrations with and without AED comedication whereas Table 5 shows a comparison of serum levels of two patients each, on similar doses of LEV while on concomitant use of other AEDs. Although taken at different time intervals since drug intake, the serum levels of LEV were 7.8% higher in patients on concomitant drug VA and 56.8% lower in patients on concomitant inducer drugs (carbamazepine, phenobarbitone, phenytoin) as compared to those in patients on concomitant neutral drugs (clobazam, lamotrigine, oxcarbazepine, topiramate) or LEV monotherapy. Most common ADRs reported were somnolence and aggressiveness. Serum LEV levels of these patients were within or below the normal trough levels of serum LEV and had no correlation with these ADRs. No patients showed signs of any toxicity.
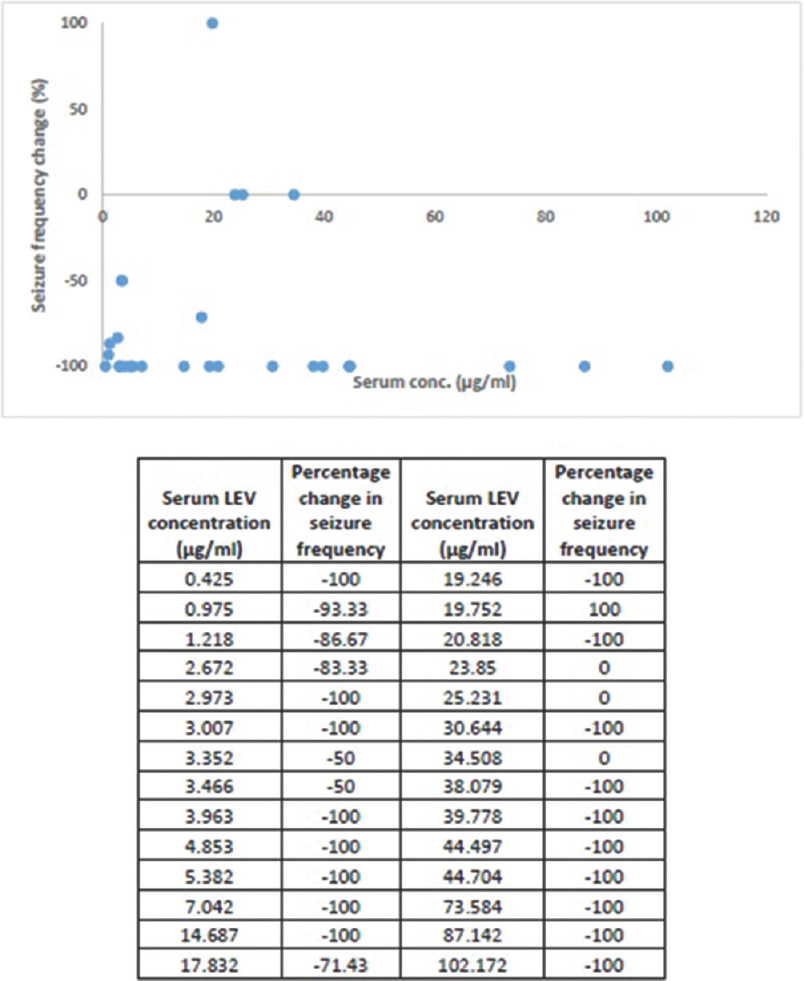
- Change in seizure frequency versus serum levetiracetam concentrations


DISCUSSION
In this study, the serum LEV levels (nontrough) showed a negligible negative correlation with the dose of LEV given per kilogram (kg) bodyweight. Mathew et al. (n = 69) obtained a negligible positive correlation (r = 0.29) while May et al. (n = 297) obtained a moderately positive correlation (r = 0.67) between trough serum LEV concentration and dose per kg bodyweight.[789] Although there exists a linear relationship between the dose and the trough serum levels of LEV over a dose range of 500–5000 mg, some studies have however suggested that serum levels of LEV can get affected by a number of parameters such as age, bodyweight, comedication, hepatic, or renal insufficiency.[6] Furthermore, the LEV concentrations depend on the time interval from the last dose taken, and because of short half-life (6–8 h), large fluctuations are expected during the day; as a result, nontrough levels of LEV could not be well correlated with the dose.[9]
Serum levels of LEV showed negligible positive correlation with the age of the patients as also seen by Mathew et al. (r = 0.19) in their study.[78] Elderly patients showed higher serum LEV levels as compared to younger patients. This is in conjunction with a study conducted by May et al. according to which older patients need a lower LEV dose per bodyweight than young adults to achieve comparable LEV levels.[9] It has been concluded that the older adults have lower clearance (CL) than younger adults and therefore require a mean 40% lower dose of LEV to achieve the same serum level.[10] Age affect the apparent clearance of LEV to the largest extent as shown by a 40% reduction in the elderly compared with the adults. This difference in the serum concentration of LEV can be due to the difference in the clearance rate of the drug from the kidney with age.[11]
Three studies done on the correlation of serum LEV levels with gender came out with a conclusion that gender had no significant effect on the serum levels, and/or clearance of LEV but another study found that females had 12% higher LEV exposure than males.[9121314] In the present study, only two patients (one male and one female) could be compared as blood samples for them were collected at the same time gap (3.5 h), where the female patient showed a higher concentration of LEV as compared to the male patient. This could be due to the differences in the bodyweight between the two genders (males are heavier), but due to limited number of comparable subjects, no significant conclusions could be drawn as in regard to the effect of gender on serum LEV levels. Radtke in his study (n = 391) showed that any differences in the pharmacokinetic parameters (if present) are likely related to the differences in bodyweight of both the genders and show no differences when normalized for bodyweight.[6]
According to Pigeolet et al. (n = 524) bodyweight has a statistically significant effect on apparent plasma clearance of LEV and its volume of distribution. Decreasing bodyweight from 70 kg to 40 kg increased LEV exposure by 16%. In this study also, the serum levels were found to be higher in ≤60 kg patients as compared to >60 kg patients, and the correlation between serum LEV levels and bodyweight was negligibly negative against that seen by Mathew et al. (r = 0.12)[7814]
In a study (n = 24), it was found that all pharmacokinetic parameters of both oral and liquid formulations of LEV were bioequivalent and therefore no adjustment in dosage is necessary if a patient is switched from one formulation to another. In this study, all patients except two were on oral tablets. The only patient on syrup was elderly (73 years) and showed a higher concentration of LEV which could be due to the age. On the other hand, other patient (age 65 years) on intravenous injection had a high concentration which could also be due to the age or a higher dose [Table 3]. Therefore, no clear conclusion could be drawn of the effect of formulations on the serum concentration of LEV.[15]
All patients showed compliance to drug therapy as they had detectable levels of LEV in their serum, but they may or may not be strictly adherent to the dosage schedule as these levels were measured at different time gaps from the drug intake and blood sample collection and vary widely with a range of 0.4–102.2 µg/ml. The values on the lower side of this range are well below the established lower trough range of LEV (before the scheduled next dose) in the western studies (12 µg/ml) while patients still showing improvement in their seizure frequency.[2]
There was no observed relationship of the clinical response seen in our patients with the serum concentration of LEV. This was similar to what was seen in the study conducted by Sheinberg et al., (n = 50) where 95% of the patients had more than a 50% reduction of seizure frequency; only one patient had increased seizure frequency, and two had no change in seizure frequency after start of LEV.[13]
Coadministration of enzyme inducer AEDs reduced the serum concentration of LEV as compared to the coadministration of neutral AEDs whereas coadministration of VA increased the LEV concentration [Table 4]. Decrease in serum levels of LEV occurs due to the increase in its clearance (CL/F) by concomitant use of enzyme inducer AEDs which have an inducible effect on the enzymes (plasma esterases, hydrolases) involved in the LEV metabolism. On the other hand, fat gain related to increased food consumption is a known ADR caused by VA. Increase in serum levels of LEV with VA occurs due to change in body water composition as LEV dissolves in water. The volume of distribution (V/F) of LEV is decreased by VA.[1012141617]
Hirsch et al. (n = 629) showed that drowsiness and psychiatric/behavioral effects were the most common adverse effects associated with LEV use.[10] Sheinberg et al. found that there was no relationship between serum concentrations of LEV and adverse events.[13] In this study also, we found that the most common ADRs were somnolence and aggressiveness and that they could not be correlated with the serum concentrations of LEV.
No patients showed signs of any toxicity like psychosis or suicidal tendencies. There is no cut off limit of serum levels of LEV in the literature above which toxicity appears. Only three patients showed serum levels of LEV above upper limit of trough therapeutic range (46 µg/ml). As these levels have been obtained at 3 h (87.1 µg/ml), 3.5 h (73.6 µg/ml), and 14 h (102.2 µg/ml) gap of drug intake and blood sample collection, they may not suggest toxic levels even otherwise.[18]
Limitations
Despite being a pilot study with a small sample size, the present study has shown that the serum LEV levels are affected by the age, bodyweight and use of comedications and can also predict patient compliance. A study with a larger sample size in the future can be done which could provide robust conclusions about each parameters studied. Although the purpose of the present project was to study the ranges of serum LEV concentrations irrespective of the time gap between the last dose taken and the blood sample collection, a future study with blood samples collected at the same time after the drug intake, preferably the trough samples just before the next morning dose of LEV, should be preferably done as LEV shows variations in its serum levels throughout the day. Better comparisons can also be made if patients are enrolled with same total doses instead of different doses.
CONCLUSION
AED therapy is prescribed quite commonly at all levels of patient care, i.e., both rural and urban clinical practice. Using newer AEDs is quite costly but nevertheless necessary as regard to their advantages over the older well-established counterparts. However, guided administration of these drugs is quite imperative for the purpose of rational prescribing and long-term patient care. This study was done to find the LEV concentrations irrespective of the timing of last doses for the purpose of population pharmacokinetic studies. The study emphasizes that the TDM of newer AEDs like LEV should be done in routine clinical practice so as to adjust the dose according to age, bodyweight, and comedication and prevent its adverse effects. More studies on TDM of newer AEDs is required on a large number of Indian patients to develop a pooled database for generating the pharmacokinetic data ranges for our population. Newer AEDs should be prescribed based on the TDM data available so as to prevent the irrational practice of medicine, complications of ADRs, toxicity, and various drug-drug interactions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Therapeutic drug monitoring of old and newer anti-epileptic drugs. Clin Chem Lab Med. 2004;42:1228-55.
- [Google Scholar]
- Antiepileptic drugs – Best practice guidelines for therapeutic drug monitoring: A position paper by the subcommission on therapeutic drug monitoring, ILAE Commission on Therapeutic Strategies. Epilepsia. 2008;49:1239-76.
- [Google Scholar]
- 2011. Measurement of Levetiracetam in Serum or Plasma by Homogeneous Immunoassay. Cleveland Ohio. Available from: http://www.clevelandcliniclabs.com/portals/66/PDF/TechBriefs/LevetiracetamTech Brief.pdf
- Usefulness of monitoring free (unbound) concentrations of therapeutic drugs in patient management. Clin Chim Acta. 2007;377:1-13.
- [Google Scholar]
- Therapeutic drug monitoring of the newer anti-epilepsy medications. Pharmaceuticals (Basel). 2010;3:1909-35.
- [Google Scholar]
- An initial experience with therapeutic drug monitoring of levetiracetam as reported from a pediatric clinical setting in India. Neurol India. 2012;60:146-9.
- [Google Scholar]
- Applied Statistics for the Behavioral Sciences (5th ed). Boston: Wadsworth Publishers; 2003.
- Serum concentrations of levetiracetam in epileptic patients: The influence of dose and co-medication. Ther Drug Monit. 2003;25:690-9.
- [Google Scholar]
- Effect of age and comedication on levetiracetam pharmacokinetics and tolerability. Epilepsia. 2007;48:1351-9.
- [Google Scholar]
- Pharmacokinetic variability of four newer antiepileptic drugs, lamotrigine, levetiracetam, oxcarbazepine, and topiramate: A comparison of the impact of age and comedication. Ther Drug Monit. 2012;34:440-5.
- [Google Scholar]
- Levetiracetam therapeutic monitoring in patients with epilepsy: Effect of concomitant antiepileptic drugs. Ther Drug Monit. 2004;26:375-9.
- [Google Scholar]
- Correlation between efficacy of levetiracetam and serum levels among children with refractory epilepsy. Pediatr Neurol. 2015;52:624-8.
- [Google Scholar]
- Population pharmacokinetics of levetiracetam in Japanese and Western adults. Clin Pharmacokinet. 2007;46:503-12.
- [Google Scholar]
- Levetiracetam: Relative bioavailability and bioequivalence of a 10% oral solution (750 mg) and 750-mg tablets. J Clin Pharmacol. 2003;43:1370-6.
- [Google Scholar]
- Therapeutic drug monitoring of levetiracetam and lamotrigine: Is there a need? Ther Drug Monit. 2015;37:437-44.
- [Google Scholar]
- Age and comedications influence levetiracetam pharmacokinetics in children. Pediatr Neurol. 2010;43:231-5.
- [Google Scholar]
- Levetiracetam in the treatment of epilepsy. Neuropsychiatr Dis Treat. 2008;4:507-23.
- [Google Scholar]




