
Translate this page into:
Using Multistate Observational Studies to Determine Role of Hypertension and Diabetes as Risk Factors for Dementia
Address for correspondence: Dr. Sunil Kumar Raina, Department of Community Medicine, Dr. R. P. Government Medical College, Kangra, Tanda, Himachal Pradesh, India. E-mail: ojasrainasunil@yahoo.co.in
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Evidence suggests that modifiable risk factors which can be targeted by prevention are vascular diseases, such as diabetes, midlife hypertension (HTN), midlife obesity, midlife cholesterol, mid- and late-life depression as well as lifestyle factors such as smoking, physical inactivity, and poor diet.
Methods:
A comprehensive search of the National Library of Medicine's PubMed database and Google Scholar was conducted. A combinations of medical subject headings and free text words that included search terms related to the exposure (e.g., prevalence, HTN, raised BP, high BP, diabetes, high blood sugar, DM, India, state), were combined with search terms related to the outcomes (e.g., prevalence, disease burden, estimate, dementia, India). The filters included were English for the language category and humans for the study category.
Results:
The PubMed search initially identified 269 references, and a total of 204 abstracts were screened by inclusion criteria. Full-text assessment of 136 articles on prevalence of dementia resulted in 20 relevant articles from which the different regions of the country were identified. Based on the search conducted according to the regions; 287abstracts of the prevalence of HTN and 577 on the prevalence of diabetes mellitus were screened. There were 43 full-text articles on the prevalence of HTN and diabetes from the regions where the prevalence of dementia was available. Of these potentially relevant articles were 14 in number.
Conclusion:
Despite the uncertainty in the role, the data analysis, therefore, points to a role in the prevention of HTN and diabetes to prevent dementia.
Keywords
Dementia
diabetes
hypertension
multi-state
observational studies
risk

INTRODUCTION
The World health organization defines dementia as a syndrome; usually of a chronic or progressive nature, in which there is deterioration in cognitive function (i.e., the ability to process thought) beyond what might be expected from normal aging. It affects memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgment. Dementia is one of the major causes of disability and dependency among older people worldwide.[1]
Worldwide, 47.5 million people have dementia, with just over half (58%) living in low- and middle-income countries. The estimated proportion of the general population aged 60 and over with dementia at a given time is 5–8 per 100 people.[1] In 2010, it is estimated that over 3.7 million people are affected by dementia in India.[2] This is expected to double by 2030. India's demographic dividend is shifting to aging population and with this the numbers of persons with dementia will double every 5 years of age. Hence, India will have one of the largest numbers of elders with this problem.
Evidence suggests that modifiable risk factors which can be targeted by prevention are vascular diseases, such as diabetes, midlife hypertension (HTN), mid-life obesity, midlife cholesterol, mid- and late-life depression as well as lifestyle factors such as smoking, physical inactivity, and poor diet.[1]
Midlife HTN is a highly predictive parameter of subsequent cognitive deterioration.[3] In the Framingham study, cognitive functioning was negatively correlated with the initial systolic and diastolic blood pressure (SBP and DBP, respectively) values measured 12–14 years before.[4] Diabetes mellitus (DM) causing micro and macrovascular complications is a well-known risk factor for stroke which if they accumulate or strike vital brain segments may cause dementia.[5] A better understanding of the risk factors and identification of factors which would protect or may reduce the risk for dementia is essential for controlling this “silent epidemic.”[1]
This article reviews major modifiable risk factor such as HTN and DM for dementia through a combination of observational studies.
METHODS
Search strategy
We comprehensively searched the National Library of Medicine's PubMed database and Google Scholar from February to July 2016. We used combinations of medical subject headings (MESH) and free text words that included search terms related to the exposure (e.g., prevalence, HTN, raised BP, high BP, diabetes, high blood sugar, DM, India, state), which were combined with search terms related to the outcomes (e.g., prevalence, disease burden, estimate, dementia, India). The filters included were English for the language category and humans for the study category. We identified articles eligible for further review by performing an initial screen of identified titles or abstracts, followed by a full-text review.
Selection criteria
Articles included in the review were cross-sectional or cohort; studies conducted among adult populations (≥18 years old) published after year 1995. Articles on the prevalence of dementia were searched first and were segregated region wise. The states or regions with reported dementia prevalence were added in the MESH to search-related exposure (DM and HTN) in that state. Since chronic conditions such as cognitive decline start developing years after the incidence of HTN,[6] the studies on risk factors obtained were those published before or during the prevalence data of dementia.[7891011121314151617181920212223] HTN was defined as SBP more than or equal to 140 and or DBP more than or equal to 90 mmHg, and DM was defined as fasting blood sugar ≥126 mg/dl or postprandial blood sugar ≥200 mg/dl. Articles were excluded if they were letters, abstracts, conference proceedings, case series, case–control studies, reviews, and meta-analysis; not conducted on humans; not community-based studies, and not pertaining to regions with reported dementia prevalence.
Study selection
Two independent reviewers (Desraj and Mitasha Singh) screened the titles and abstracts of the initially identified studies to determine whether they would satisfy the selection criteria. Any disagreements about selection were resolved through consensus or consultation with a third author (Manoj Kumar Gandhi). Full-text articles were retrieved for the selected titles. Reference lists of the retrieved articles were searched for additional publications. The retrieved studies were assessed again by two independent authors (Sunil Kumar Raina and Vishav Chander) to ensure that they satisfied the inclusion criteria.
Data extraction
A data collection form was designed before the implementation of the search strategy. This form was used by two independent reviewers to extract the relevant information from the selected studies (Des Raj and Mitasha Singh). The data collection form included questions on year of publication, design, geographic origin and setting, and information on the reported exposure and outcomes (e.g., percentage of population with dementia, percentage of hypertensive patients, and percentage of diabetic patients).
Statistical analysis
Regression analysis was run for each of exposure variable (DM and HTN) in linear regression analysis. Pearson's correlation coefficient was presented for both the factors.
RESULTS
The PubMed search initially identified 269 references, and a total of 204 abstracts were screened by inclusion criteria. Full-text assessment of 136 articles on the prevalence of dementia resulted in 20 relevant articles, from which the different regions of the country were identified. Based on the search conducted according to the regions, 287abstracts of the prevalence of HTN and 577 on the prevalence of DM were screened. There were 43 full-text articles on prevalence of HTN and diabetes from the regions where the prevalence of dementia was available. Of these potentially relevant articles were 14 in number.
The prevalence of dementia has been studied using different criteria in different regions of the country. The highest prevalence in the above Table 1 was observed from the Southern State of Tamil Nadu from district Vellore (rural area) reported prevalence of 10.6% and from Chennai (urban) reported a prevalence of 7.5% using 10/66 dementia diagnosis criteria.[2] The study (10/66) which reported dementia prevalence also reported prevalence of HTN and diabetes in Tamil Nadu.[24] The prevalence of HTN (68.6%) and diabetes (12.1%) was higher in urban area as compared to rural (45.6% and 6.6%, respectively).
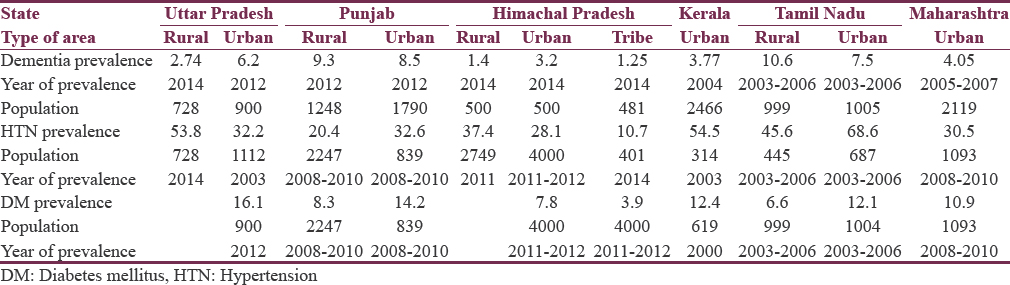
In north, Punjab reported a high prevalence of dementia in district Ludhiana, 8.5% in urban, and 9.3% in rural area using Hindi version of Mini-Mental State Examination (HMSE).[19] Another study in same region reported a prevalence of 35.9% and 20.9% of HTN in the rural and urban area, respectively.[18] The prevalence of DM was also reported to be higher in urban area as compared to rural area (14.2% and 8.3%, respectively).[20]
A higher prevalence of dementia was observed in the north, in the state of Uttar Pradesh in an urban area of Lucknow city; 6.2% using MMSE scale followed by Cambridge Examination for Mental Disorders of the Elderly Revised.[15] Another study also reported prevalence of dementia as 2.74% using a series of tests from rural area of Varanasi.[14] The prevalence of HTN was reported to be higher in rural area of Varanasi; 53.8%[14] as compared to urban area of Lucknow (32.2%).[16] The prevalence of diabetes in urban area of Lucknow was reported to be 16.1%.[15]
The state of Maharashtra in West in a study from urban region of Pune reported the prevalence of dementia to be 4.05%, and the prevalence of HTN and diabetes in this region as reported by India, AB study was 30.9% and 10.9%, respectively.[22]
A study by Mathuranath et al.[12] from Kerala in the south reported a prevalence of dementia to be 3.77% in an urban area of Thiruvananthapuram using a cognitive screening battery followed by diagnostic evaluation, whereas another study from the same region reported 54.5%[13] prevalence of HTN and 12.4% prevalence of DM.[11]
A study from Himachal Pradesh in north reported the prevalence of dementia as 3.2% from urban area, 1.4% from rural area, and 1.25% from tribal area using HMSE scale.[10] Other studies from same region reported a higher prevalence of HTN from rural area (37.4%) as compared to urban (28.1%)[8] and tribal area (10.7%).[9] The prevalence of DM was reported to be 7.8% from urban area and 3.9% from tribal area.[7]
The prevalence of diabetes and HTN with dementia from Table 1 was subjected to linear regression analysis. Table 2 depicts the Pearson's correlation coefficient of the relation between the prevalence of exposure and outcome. An imperfect positive association was observed for both HTN (r - 0.17, P - 0.62) and diabetes (r - 0.22, P - 0.57) with dementia. The same has been shown in scatter plots of Figures 1 and 2.

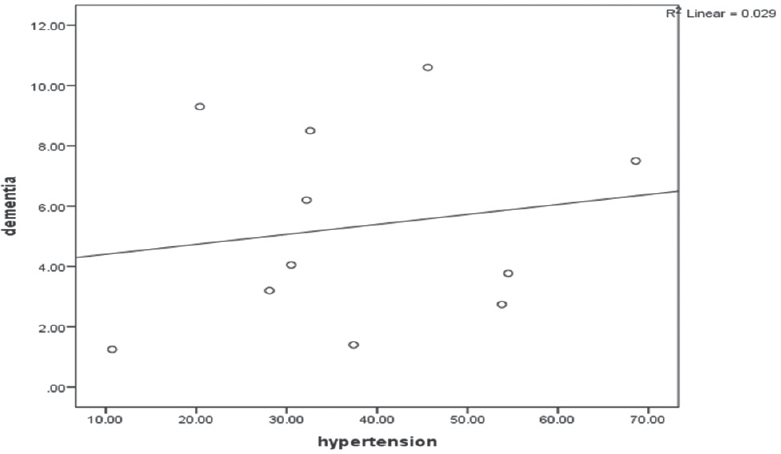
- Correlation between prevalence of hypertension and dementia
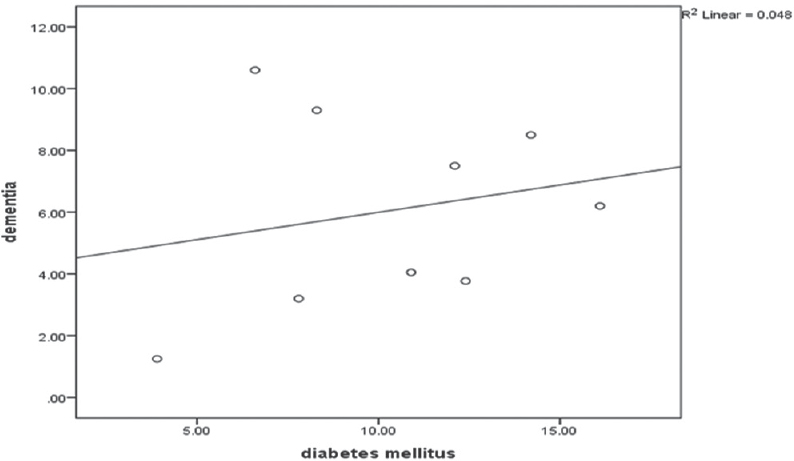
- Correlation between the prevalence of diabetes mellitus and dementia
DISCUSSION
HTN has been identified as one of the most important controllable risk factors for stroke, which in turn can result in vascular dementia. According to Barnes and Yaffe,[25] given the available literature from epidemiological studies and randomized controlled trials only mid-life, not late-life HTN is associated with an increased risk of AD and dementia. About 5% (1.7 million) of AD cases worldwide are potentially attributable to mid-life HTN according to Barnes and Yaffe. According to a review by Biessels et al., of 14 eligible longitudinal population-based studies, the risk of dementia is, in general, increased in patients with DM, and this increased risk seems to include both Alzheimer's disease and vascular dementia.[26] On analysis by Pasquier et al. of prospective and cross-sectional studies, found evidence of an elevated risk of both vascular dementia and AD in patients with strong interaction of other factors such as HTN, dyslipidemia, and ApoE genotype.[27] Pasqueler et al. also found that DM type 2 to be an independent predictor of poststroke dementia.[27] The current study points to a positive association between diabetes, HTN, and Dementia even though the association is not perfect. The results from a study conductive by us previously also pointed to an association between raised BP and dementia although we were not able to establish a relation between diabetes and dementia.[28] Although there is uncertainty regarding the relationship between BP and risk of dementia, AlzRisk does promote that the benefits of BP control on cardiovascular risk are sufficient to justify the role of preventing HTN to prevention of dementia. However the same cannot be said of diabetes and dementia.[29] According to Biessels et al., there is still a need for studies on large population-based cohorts of elderly people with diabetes.[26]
CONCLUSION
Despite the uncertainty in the role, the data analysis, therefore, points to a role in the prevention of HTN and diabetes to prevent dementia.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 2016. World Health Organization. Fact Sheet on Dementia. Available from: http://www.who.int/mediacentre/factsheets/fs362/en/
- Alzheimer's and Related Disorders Society of India. The Dementia India Report: Prevalence, Impact, Costs and Services for Dementia: Executive Summary. New Delhi: ARDSI; 2010.
- Untreated blood pressure level is inversely related to cognitive functioning: The Framingham Study. Am J Epidemiol. 1993;138:353-64.
- [Google Scholar]
- Diabetes mellitus and the risk of dementia: The Rotterdam Study. Neurology. 1999;53:1937-42.
- [Google Scholar]
- Neurovascular regulation in the normal brain and in Alzheimer's disease. Nat Rev Neurosci. 2004;5:347-60.
- [Google Scholar]
- Prevalence of diabetes mellitus and its risk factors among permanently settled tribal individuals in tribal and urban areas in Northern State of Sub-Himalayan Region of India. Int J Chronic Dis 2014 2014:380597.
- [Google Scholar]
- Feasibility of development of a cohort in a rural area of Sub-Himalayan Region of India to assess the emergence of cardiovascular diseases risk factors. Int J Chronic Dis 2014 2014:761243.
- [Google Scholar]
- Prevalence of hypertension in a tribal land locked population at high altitude. Scientifica (Cairo) 2016 2016:3589720.
- [Google Scholar]
- Is dementia differentially distributed? A study on the prevalence of dementia in migrant, urban, rural, and tribal elderly population of Himalayan region in Northern India. N Am J Med Sci. 2014;6:172-7.
- [Google Scholar]
- Type 2 diabetes in Southern Kerala: Variation in prevalence among geographic divisions within a region. Natl Med J India. 2000;13:287-92.
- [Google Scholar]
- Dementia in Kerala, South India: Prevalence and influence of age, education and gender. Int J Geriatr Psychiatry. 2010;25:290-7.
- [Google Scholar]
- Prevalence, correlates, awareness, treatment, and control of hypertension in a middle-aged urban population in Kerala. Indian Heart J. 2003;55:245-51.
- [Google Scholar]
- A clinico-epidemiological study of cognitive function status of community-dwelling elderly. Indian J Psychiatry. 2014;56:365-70.
- [Google Scholar]
- Diabetes mellitus: A risk factor for cognitive impairment amongst urban older adults. Ind Psychiatry J. 2012;21:44-8.
- [Google Scholar]
- Prevalence and risk factors of pre-hypertension and hypertension in an affluent north Indian population. Indian J Med Res. 2008;128:712-20.
- [Google Scholar]
- Prevalence of psychiatric morbidity amongst the community dwelling rural older adults in northern India. Indian J Med Res. 2013;138:504-14.
- [Google Scholar]
- Prevalence of hypertension and its risk factors among urban Sikh Population of Amritsar. Int J Sci Res. 2014;3:827-32.
- [Google Scholar]
- Prevalence and correlates of cognitive impairment in a North Indian elderly population. WHO South East Asia J Public Health. 2014;3:135-43.
- [Google Scholar]
- Prevalence of diabetes and prediabetes (impaired fasting glucose and/or impaired glucose tolerance) in urban and rural India: Phase I results of the Indian Council of Medical Research-INdia DIABetes (ICMR-INDIAB) study. Diabetologia. 2011;54:3022-7.
- [Google Scholar]
- ICMR-India Diabetes Study (INDIAB), Phase1 Report. New Delhi: Indian Council of Medical Research; 2016.
- An epidemiological study of dementia under the aegis of mental health program, Maharashtra, Pune chapter. Indian J Psychiatry. 2010;52:131-9.
- [Google Scholar]
- Prevalence of dementia in Latin America, India, and China: A population-based cross-sectional survey. Lancet. 2008;372:464-74.
- [Google Scholar]
- The prevalence, correlates, detection and control of diabetes among older people in low and middle income countries. A 10/66 dementia research group population-based survey. PLoS One. 2016;11:e0149616.
- [Google Scholar]
- The projected effect of risk factor reduction on Alzheimer's disease prevalence. Lancet Neurol. 2011;10:819-28.
- [Google Scholar]
- Risk of dementia in diabetes mellitus: A systematic review. Lancet Neurol. 2006;5:64-74.
- [Google Scholar]
- Hypertension and diabetes as risk factors for dementia: A secondary post-hoc analysis from North-West India. Ann Indian Acad Neurol. 2015;18:63-5.
- [Google Scholar]
- Policy Brief-Risk Factors for Dementia. Available from: http://www.alzrisk.org/riskfactordoc.aspx?rfid=5




