
Translate this page into:
The Epidemiology of Traumatic Brain Injury Due to Traffic Accidents in Latin America: A Narrative Review
 , Ethne Grey Still3, María N. Suarez4, José A. González-Soto5, David S. Vera6, Andrés M. Rubiano6,7
, Ethne Grey Still3, María N. Suarez4, José A. González-Soto5, David S. Vera6, Andrés M. Rubiano6,7
Andrés M. Rubiano, MD Instituto de Neurociencias, Universidad El Bosque Av. Cra 9 No 131 A-02, Bogotá 110121 Colombia andresrubiano@aol.com
This article was originally published by Thieme Medical and Scientific Publishers Private Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Objective Traumatic brain injuries (TBIs) are devastating injuries and represent a major cause of morbidity and mortality worldwide. Traffic accidents are one of the main causes, especially in low- and middle-income countries. The epidemiology of TBI due to road traffic in Latin America is not clearly documented.
Methods A narrative review was conducted using PubMed, SCOPUS, and Google Scholar, looking for TBI studies in Latin America published between 2000 and 2018. Seventeen studies were found that met the inclusion and exclusion criteria.
Results It was found that TBI due to road traffic accidents (RTAs) is more frequent in males between the ages of 15 and 35 years, and patients in motor vehicles accounted for most cases, followed by pedestrians, motorcyclists, and cyclists.
Conclusion Road traffic accidents is a common cause of TBI in Latin America. More studies and registries are needed to properly document the epidemiological profiles of TBI related to RTAs.
Keywords
brain injuries
epidemiology
Latin America
trauma
road traffic accidents

Introduction
Every year more than 10 million people are affected by traumatic brain injuries (TBIs). Despite efforts being made to improve TBI care, it remains a public health problem, continuing to cause high mortality and morbidity in a young population. The World Health Organization (WHO) considers TBI to be one of the most pressing and underrecognized areas in public health problems, with predictions that by 2020, it will be the third highest cause of death and disability. It has been shown that in low-middle income countries in the past 17 years, violence and road traffic accidents (RTAs) have been the main causes of TBI and have associated high mortality.1
There is a clear regional variation in the disease impact; not only low- and middle-income areas do have a higher incidence of TBI but also are associated with greater morbimortality. A reason for this may be the lower level of acute health care provision in these areas, lack of access to existing health care systems, and disjointed or nonexistent preventative measures.2
Although violence and industrial accidents account for a significant proportion of TBI worldwide, by far the greatest contributor is RTAs, which estimated 60% of the total TBI burden.1 Traffic accidents make up 2.5% of total deaths worldwide, and the WHO predicts that by 2030, RTA will become the seventh leading cause of death, with an increase from 2.5% in 2015 to 2.6% in 2030 of total world deaths.2 There is a clear regional variation in line with economic prosperity. Despite high-income countries having 46% of the total vehicles registered worldwide, they make up 10% of RTA deaths.2
Latin America is a region particularly in need of study. Despite knowing overall mortality from RTA in this area and that TBI is a common sequela of RTA, there are few studies on the impact of RTA on TBI in the Latin American region.3 Without these data, it is hard to know the extent of the problem, and to direct resources toward the acute care and rehabilitation of TBI victims. Although some valuable research has been done in this area, an accurate overall picture of the problem is hindered by small sample sizes, the heterogeneity of the data, and the lack of focus on epidemiology and etiology.
The purpose of this literature review was to describe the epidemiology of TBI as a result of RTA in Latin America. We limited our search to the 2000 to 2018 period.
Materials and Methods
Study Design
The electronic databases SCOPUS, PubMed, and Google Scholar were searched for articles containing epidemiological data on TBI related to RTA in Latin America (South America, Central America, and the Caribbean) between the years 2000 and 2018.
Search terms were divided into four broad term areas, as shown in Table 1.
|
Region |
Injury |
Scenario |
Statistics |
|---|---|---|---|
|
Caribbean region |
Brain injury |
Accidents, traffic |
Epidemiology |
|
South America |
Craniocerebral |
Demography |
|
|
Central America |
Trauma |
Trauma centers |
|
|
Latin America |
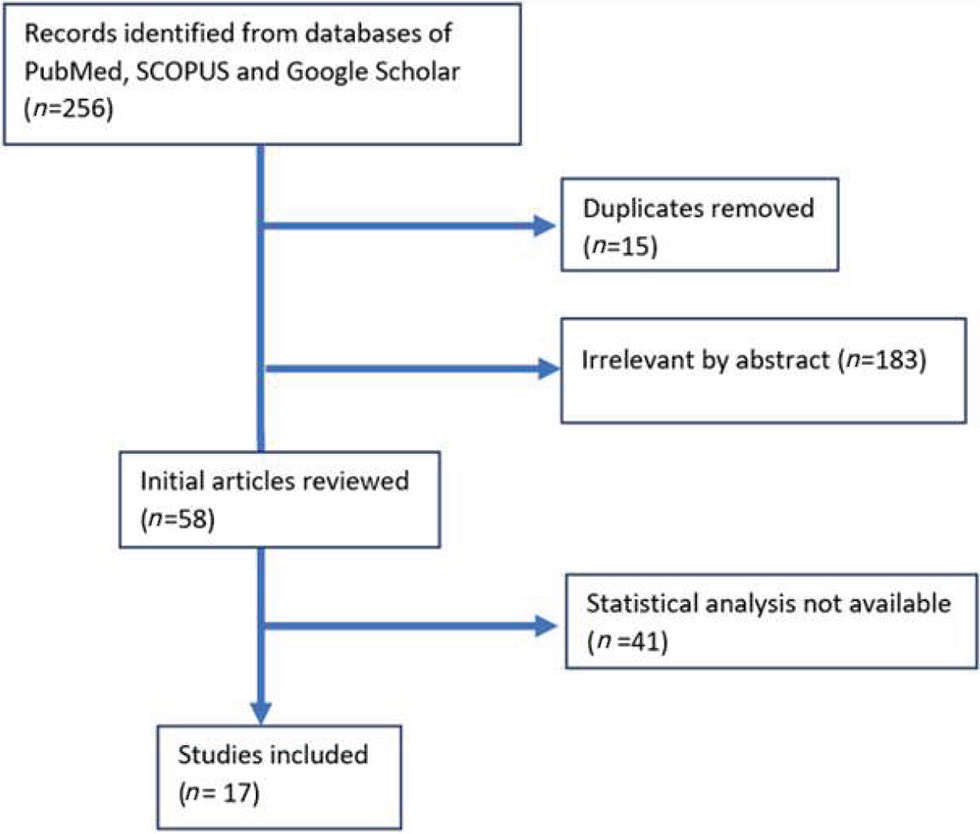
A total of 256 potentially relevant articles were found from the initial search of the journal databases. Inclusion and exclusion criteria were applied as seen in Table 2. These were assessed and analyzed by three of the authors and, after discussions, mutual agreement decided which articles should be included. Then, 198 abstracts were immediately excluded because they were duplicates and the summary was irrelevant. The remaining 58 articles were analyzed, out of which only 17 articles were deemed eligible for the statistical analysis as described in Fig. 1.
|
Inclusion criteria |
Exclusion criteria |
|---|---|
|
Abbreviations: RTA, road traffic accident; TBI, traumatic brain injury. |
|
|
Any language |
Studies not available in full text |
|
Published date: 2000–2018 |
Studies with only TBI data without RTA as cause of injuries |
|
Latin American study |
Studies with only RTA data without TBI data |
|
Studies containing both TBI and RTA data |
|
-
Fig. 1 Literature search flowchart. The literature search process in the different databases.
Fig. 1 Literature search flowchart. The literature search process in the different databases.
Data Analysis
To view the scope of the data available, we tabulated all the epidemiological data pertaining to TBI as a result of RTA. Once tabulated, the reviewers agreed to use the variables: sex, age, outcome post-TBI, severity of TBI, mode of transport, safety devices, and impact of helmets. These variables were the most widely recorded among the articles and were considered, by the reviewers, to be important for patient outcome.
Results
Patient Characteristics
We found seven studies that listed the patient’s sex. There were a total of 1,752 patients with a sex distribution of 77% males and 23% females. The range across the seven studies was from 75 to 94% male.4 The study with the largest sample size was a Brazilian study with 800 motor vehicle-associated TBI. In that, automobile accident was the most frequent. Across all vehicle types, there was a predominance of male sex, and a mean age in the 20 to 30 years range.
In a different Brazilian study, in the emergency department, the patients’ age brackets ranged from 15 to 85 years. There was a strong predominance of younger patients, with 15 to 25 and 26 to 35 age ranges making up 61% of the patients. In contrast to this, the 66 to 85 age bracket accounted for 6% of TBI.5
Mode of Transport
In 11 studies with a total population of 2,769 patients, classified as accidents to pedestrians, motorcycles, or cars, car (automobile) was involved in 43% of TBI, as compared with motorbike (30%) and pedestrian (27%). However, only six studies (1,753 patients) included a pedal bicycles category. Car dropped slightly to 40%, while motorbike and pedestrian were both associated with 23% of TBI. Pedal bike was associated with 14% of TBI.
TBI Severity
The severity of the TBI (as assessed by the Glasgow coma scale) was recorded for a total of 1,986 patients. Mild TBI was the most frequent type of TBI (90%), followed by severe (7%) and moderate (3%).
Outcome post-TBI
A study across six centers in Bolivia and Ecuador demonstrated a similar outcome trend in severe TBI when comparing vehicles involved. Most patients had an outcome of a Glasgow outcome scale extended (GOSE) of 5 to 8, indicating a good outcome. The second most frequent outcome was inpatient death, followed by a GOSE of 2 to 4. The least frequent outcome was late death. In an Argentinian study, also in patients with severe TBI, the most frequent outcome was mortality at 56%, with only 44% of patients being discharged home. A Jamaican study, which did not specify severity, found that 90% of motorcyclists suffering a TBI had an outcome of 3 to 5 GOSE, with 2% suffering a GOSE from 1 to 2, and there was an 8% mortality rate.
Role of Helmets in TBI Prevention
A Brazilian study measuring the impact of helmets usage in motorcycle accidents reported that TBI was present in 52.2% of patients with a full-face helmet, 76.5% of those with an open face helmet, and 69.2% of those with no helmet.
A Haitian study described the presence of safety devices in patients presenting with a TBI from an associated RTA; 95% of patients had no safety device associated, 4% had used a seatbelt, and 1% of patients were wearing a helmet.6
Discussion
Most studies on TBIs focus on the treatment and outcomes. Worldwide, epidemiological studies are scarce, and for our study, this obstacle was compounded by the lack of Latin American studies and our narrow focus on RTA-associated TBI. However, the results we did find do give us an overall view of the epidemiological base. Seven compiled studies7 indicate a much higher prevalence among males (77%) than female. This is notably similar to other studies on urban traumatic outcomes in Latin America, such as in maxillofacial fracture,8 implying a possibility that there is prevalence in males involved in traumatic events such as motor collisions rather a predisposition to TBI.
The most affected age range was within the 15 to 25 and 26 to 35 age brackets, making up 61% of the patients. In contrast to this, the 66 to 85 age bracket accounted for 6% of TBI. It is difficult to assume an increased vulnerability in younger age groups to TBI from these numbers, as these age groups are more populous and may be more likely to use motor vehicles. However, what is clear is that because of the high morbidity associated with the injury, those who are most affected are excluded from the work market and burden the social security and health systems. At this age, people begin to be economically and socially more active, and presenting a TBI at this age can have a profound long-term impact on them and their families. An epidemic that affects mainly the young damages a country’s future.9
From 11 studies,1 5 6 8 10 11 12 13 14 15 16 car accidents were involved in 43% of TBI, as compared with motorbike (30%) and pedestrian (27%). Of the six studies1 6 11 12 14 15 (n = 1,753) including a pedal bicycles category, car dropped slightly to 40%, while motorbike and pedestrian were both associated with 23% of TBI and pedal bike was related in 14% of TBI.
From a severity point of view, the best epidemiological data came from an urban Brazilian study17 measuring the impact of traffic prevention program. All traffic-related injuries treated in the emergency department were classified and documented extensively. It generated a large amount of data, especially detailing the severity of the TBI. With a total of 1,986 patients in a 2-year period, this study was more representative for the epidemiology of an urban area. It showed that mild TBI swerve by far the most frequent type, accounting for 90%. While severe TBIs only accounted for 7%, this is still a significant number given the frequency of RTA and the poor outcome associated with severe TBI.
Point-of-injury care is critical in a TBI. This is an area where a large amount of progress has been made, with most of Latin American countries providing a high coverage of prehospital care access (83.3%). In most countries, severely injured patients were transported to hospital via ambulance in more than 75% of the cases. Only the Dominican Republic, Honduras, and Peru had an ambulance transfer rate of less than 11%; 83.3% of countries have training for doctors and 50% have training for nurses in emergency-related trauma.18
The impact of the individual’s behavioral choices in RTA is important to recognize. Factors such as not using a helmet, driving under the influence of alcohol or drugs, reckless driving, and nonuse of seat belts by the driver, codriver, or rear seat occupants are all related to patient outcome.
After this analysis is clear, there is a need in Latin America for regional databases, for the reporting and monitoring of TBI related to RTA, and for gathering data on associated morbimortality, etiology, and epidemiology. The creation of an organized, region-wide database would make data reporting easier while standardizing the data for analysis. It would allow us to compare the impact of different geographical and demographic features on overall survival and disability. This would facilitate the improvement of regional and national management guidelines, and the exploration of new public health programs aimed at prevention, treatment, and rehabilitation. Ultimately, data-driven public health interventions would improve patient survival, decrease morbidity, and improve quality of life for both patients and families.
Limitations
Epidemiologic data vary depending on the population location, cultural variations, socioeconomic status, and in which time period, the study was conducted. The majority of articles reviewed had small patient populations, which give a less accurate portrayal of a region as populous as Latin America. On top of this is the variation between rural and urban health care and their populations. This analysis only contained studies from urban centers.
The Latin American region contains 33 countries; however, only 6 countries contributed studies to this analysis: Brazil, Argentina, Bolivia, Ecuador, Jamaica, and Haiti. Most studies, 10 in total, came from Brazil. Although the largest geographically and most populous country in Latin America, it is difficult to extrapolate the Brazilian epidemiological data with consistency to other countries, given the variable health care, population, and cultural norms across the region.
Conclusion
It was found that TBI due to RTAs is more frequent in males between the ages of 15 and 35 years, and patients in motor vehicles accounted for most cases, followed by pedestrians, motorcyclists, and cyclists. More studies and registries are needed in Latin America to properly document the epidemiological profiles of TBI related to RTAs.
Conflict of Interest
None declared.
References
- The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007;22:341-353.
- [Google Scholar]
- Global status report on road safety 2015 [Internet]. World Health Organization. 2015. Available at: http://www.who.int/violence_injury_prevention/road_safety_status/2015/en. Accessed November 3, 2018
- Road Safety in the Americas [Internet]. PAHO/WHO Institutional Repository. 2016. Available at: http://iris.paho.org/xmlui/handle/123456789/28564. Accessed November 3, 2018
- Occurrence of severe and moderate traumatic brain injury in patients attended in a Brazilian Teaching Hospital: epidemiology and dosage of alcoholemy. Arq Neuropsiquiatr. 2008;66(1):69-73.
- [Google Scholar]
- CT scan findings in mild head trauma: a series of 2,000 patients. Arq Neuropsiquiatr. 2002;60:204-210. (2-A)
- [Google Scholar]
- The impact of helmets on motorcycle head trauma at a tertiary hospital in Jamaica. BMC Res Notes. 2009;2(1):172.
- [Google Scholar]
- The conformation of the brain plays an important role in the distribution of diffuse axonal injury in fatal road traffic accident. Arq Neuropsiquiatr. 2004;62:406-412. (2B)(2b)
- [Google Scholar]
- Risk factors for maxillofacial injuries in a Brazilian emergency hospital sample. J Appl Oral Sci. 2010;18(1):23-29.
- [Google Scholar]
- Profile of organ donors in Ceará, northeastern Brazil, from 1998 to 2012. Transplant Proc. 2014;46(6):1692-1694.
- [Google Scholar]
- Predictors of quality of life after moderate to severe traumatic brain injury. Arq Neuropsiquiatr. 2016;74(5):409-415.
- [Google Scholar]
- Intracranial pressure monitoring in severe traumatic brain injury in Latin America: process and methods for a multi-center randomized controlled trial. J Neurotrauma. 2012;29(11):2022-2029.
- [Google Scholar]
- Disease burden and mortality estimates [Internet]. World Health Organization. 2016. Available at: https://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html. Accessed November 3, 2018
- Epidemiology of traumatic injuries at an urban hospital in Port-au-Prince, Haiti. World J Surg. 2017;41(11):2674-2680.
- [Google Scholar]
- Executive functions profiles in traumatic brain injury adults: implications for rehabilitation studies. Brain Inj. 2015;29(9):1071-1081.
- [Google Scholar]
- Glasgow outcome scale at hospital discharge as a prognostic index in patients with severe traumatic brain injury. Arq Neuropsiquiatr. 2012;70(8):604-608.
- [Google Scholar]
- Impact of a program for the prevention of traffic accidents in a Southern Brazilian city: a model for implementation in a developing country. Surg Neurol. 2009;72(1):6-13, discussion 13–14.
- [Google Scholar]
- Early prognosis of severe traumatic brain injury in an urban Argentinian trauma center. J Trauma. 2010;68(3):564-570.
- [Google Scholar]




