
Translate this page into:
Sphenopalatine ganglion block for the treatment of spontaneous intracranial hypotension without demonstrable cerebrospinal fluid leak: A report of two cases
-
Received: ,
Accepted: ,
How to cite this article: Khandelwal A, Sarma S, Hussain M. Sphenopalatine ganglion block for the treatment of spontaneous intracranial hypotension without demonstrable cerebrospinal fluid leak: A report of two cases. J Neurosci Rural Pract. doi: 10.25259/JNRP_30_2024
Abstract
Spontaneous intracranial hypotension (SIH) is a condition characterized by orthostatic headache associated with nausea, vomiting, tinnitus, vertigo, hypoacusis, neck pain/stiffness, and photophobia. Usual treatment includes bed rest, hydration, caffeine, analgesics, epidural blood patch, steroids, fibrin glue (N-butyl-cyanoacrylate), and surgical repair. In this series, we report two cases, who presented to us with features of SIH and were managed successfully with sphenopalatine ganglion block. This is a novel modality of management of SIH and has not been reported before.
Keywords
Cerebrospinal fluid
Intracranial hypotension
Orthostatic headache
Sphenopalatine ganglion block

INTRODUCTION
Spontaneous intracranial hypotension (SIH) is a debilitating condition that occurs spontaneously secondary to cerebrospinal fluid (CSF) leak and/or CSF hypotension (lumbar puncture opening pressure <60 mm CSF) and typically manifests as orthostatic headache associated with nausea, vomiting, tinnitus, vertigo, hypoacusis, neck pain/stiffness, and photophobia.[1,2] Treatment options include bed rest, hydration, caffeine, analgesics, epidural blood patch (EBP),[3,4] steroids,[5,6] fibrin glue (N-butyl-cyanoacrylate),[7,8] and surgical repair.[9,10] In this series, we report two cases, who presented to us with features of SIH and were managed successfully with sphenopalatine ganglion (SPG) block. To the best of our knowledge, SPG block for the management of SIH has never been reported before. Written informed consent was obtained from the two patients for reporting the findings and consequent management.
CASE REPORT
Case 1
A 44-year-old man without any comorbidities presented to us in the outpatient department with three days of progressive worsening of occipitocervical headache. The headache was spontaneous in onset, associated with neck stiffness, aggravated on sitting and standing, and relieved in the recumbent position. However, the patient was afebrile and hemodynamically stable. There was no history of trauma, recent surgery or any spinal intervention. He was advised to undergo radiological investigations. Contrast magnetic resonance imaging (MRI) of the brain [Figure 1a and b], and spine revealed mild pachymeningeal thickening and enhancement, particularly involving the convexity meninges, tentorium, and the cervicodorsal cord with normal signal intensity. Further, constructive interference in the steady state (CISS) sequence did not show any CSF leak in the brain and the cervicodorsal spine. Central disc protrusion was noted in C5–C6 level causing mild thecal compression, however, not correlating with the symptoms. Routine blood investigations did not reveal any significant findings. Lumbar puncture was declined by the patient. Further, investigations could not be done due to financial constraints. Based on clinical and radiological findings, a diagnosis of SIH was made.
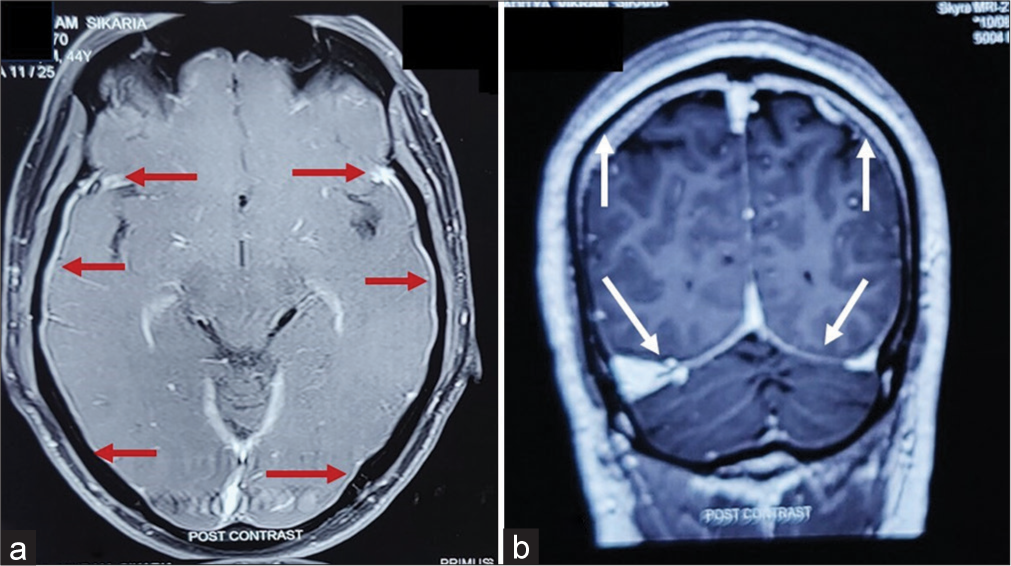
- (a) Arrows in the axial section of magnetic resonance imaging (MRI) (Post-contrast) show mild pachymeningeal thickening and enhancement without obvious cerebrospinal fluid (CSF) leak. (b) Arrows in the coronal section of MRI (Post-contrast) show mild pachymeningeal thickening and enhancement without obvious CSF leak.
Since the pathophysiology and symptomatology of SIH are similar to post-dural puncture headache (PDPH), we decided to perform an SPG block. The patient was placed in the supine position with neck hyperextended. The applicator was inserted in each nostril. We sprayed 2 puffs of 10% lignocaine spray (20 mg on each side) into each nostril of the patient while the patient took a deep breath through the nose. Then, the patient was kept supine for some minutes. This technique of SPG block was described by López et al.[11] Along with it, the patient was advised to take oral tablets of acetaminophen (650 mg) and caffeine (50 mg) combination every 8 hours and maintain adequate hydration. The next day, the patient reported of 60–65% reduction in pain. Another session of bilateral SPG block was performed, and the patient was advised to continue oral analgesics. On the third day, the patient reported around 80% pain relief with mild pain only on prolonged ambulation (telephonic follow-up). The patient was advised to stop oral analgesics. On the fourth day, the patient reported complete pain relief even during prolonged ambulation. The patient did not report a recurrence of the same discomfort or any visible CSF leak during the one-month or three-month follow-up appointments in the outpatient department (OPD).
Case 2
The second case was a 37-year-old female, who presented to us with a similar history of gradually progressive orthostatic headache, neck stiffness, nausea, and vertigo for the past four days. Similar to case 1, she did not give any history of trauma, recent surgery or any spinal intervention. A contrast MRI of the brain revealed pachymeningeal thickening and enhancement throughout without subdural effusions and tonsillar herniation. No changes were noticed in the MRI of the cervicodorsal area. Further, the CISS sequence did not show any CSF leak in the brain and the cervicodorsal spine. A diagnosis of SIH was made. Similar to case 1, the management included a bilateral SPG block, analgesics, and adequate hydration. Around 45–50% and 70–75% of the pain was relieved in 24 h and 48 h, respectively. Another session of bilateral SPG block was performed. There was a progressive reduction in pain intensity and by day five, she reported complete pain relief and resumption of her day-today activities. During the one-month and three-month follow-up visits, the patient remained asymptomatic.
DISCUSSION
SIH is one of the important causes of orthostatic headache that typically occurs in young- and middle-aged adults.[1,2] Symptomatically, the headache resembles PDPH and manifests primarily due to the sagging of the brain into the pain-sensitive structures, particularly dura mater, and secondarily due to vasodilation that occurs as a compensatory response to intracranial hypotension.[11,12] However, the course of spontaneous CSF leak in SIH does not necessarily follow the same trajectory as PDPH (both are different entities). In our cases, the CSF leak was spontaneous and did not follow any trauma or any intervention. Nevertheless, given the similarities between the headache mechanism in PDPH and SIH, as well as the efficacy of SPG block in PDPH, we proceeded to execute SPG block on both of our patients. The SPG block reduces headaches by inhibiting parasympathetic-mediated cerebral vasodilation.[11,12] The technique is simple and effective, minimally invasive, repeatable if necessary, and does not need any expertization. There is no previous literature mentioning the role of SPG block in the management of SIH. Therefore, our report is unique and opens a new door to conduct large studies in the future.
Prior studies have demonstrated that the majority of SIH patients recover in two weeks with conservative treatment, which entails bed rest, fluids, analgesics, and caffeine. However, if the headache is incapacitating or continues beyond —one to two weeks of conservative care, an EBP is usually indicated.[1,2] However, it is imperative to understand that EBP has its own risks and complications (intracranial hypertension, infectious or chemical aseptic meningitis, subdural hematoma, etc.). Moreover, it warrants multiple sessions at times, absolutely sterile conditions, and expertization. Furthermore, the reported efficacy is highly variable between 30% and 90%.[13] In our study, both the patients reported at least a 50% reduction in headache by as early as 24 h following SPG block and merely needed a second session for complete relief of the headache by the fourth day in case 1 and by the fifth day in case 2.
SIH is typically caused by CSF leakage from a spinal dural tear, a meningeal diverticulum or a CSF venous fistula. However, the previous reports have shown that 10–15% of SIH patients do not demonstrate CSF leakage despite typical orthostatic symptoms and craniospinal imaging findings.[13,14] This could possibly be due to cranial-to-spinal CSF shift rather than actual CSF leak and may occur secondary to increased spinal compliance, decreased intracranial CSF volume, low CSF outflow resistance, and decreased venous pressure.[13-15] Another reason could be that MRI findings tend to become less noticeable with time and may not demonstrate a minuscule CSF leak in every one out of three to five individuals.[14] In both our cases, MRI could not demonstrate CSF leak, and there was no recurrence of symptoms at one-month and three-month follow-up visits.
CONCLUSION
The SPG block seems to be an effective modality for the treatment of SIH. The technique is simple, minimally invasive, does not require expertization, and can be performed on an OPD basis. Further reports, particularly randomized studies, are necessary to improve the quality of the evidence.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Headache Classification committee of the international headache society (IHS) the International classification of headache disorders. In: Cephalalgia Vol 38. (3rd edition). 2018. p. :1-211.
- [CrossRef] [PubMed] [Google Scholar]
- A review of spontaneous intracranial hypotension. Curr Neurol Neurosci Rep. 2019;19:22.
- [CrossRef] [PubMed] [Google Scholar]
- Epidural blood patch for spontaneous intracranial hypotension with chronic subdural haematoma: A case report and literature review. J Int Med Res. 2016;44:976-81.
- [CrossRef] [PubMed] [Google Scholar]
- Targeted epidural blood patch treatment for refractory spontaneous intracranial hypotension in China. J Neurol Surg B Skull Base. 2018;79:217-23.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous intracranial hypotension: Two steroid-responsive cases. Pol J Radiol. 2018;83:e229-33.
- [CrossRef] [PubMed] [Google Scholar]
- First-line steroid treatment for spontaneous intracranial hypotension. Eur J Neurol. 2022;29:947-9.
- [CrossRef] [PubMed] [Google Scholar]
- Successful treatment of spontaneous intracranial hypotension by plugging the cerebrospinal fluid leak with percutaneous cyanoacrylate injection: A report of 2 cases. World Neurosurg. 2016;91:390-8.
- [CrossRef] [PubMed] [Google Scholar]
- Targeted epidural patch with n-butyl cyanoacrylate (n-BCA) through a single catheter access site for treatment of a cerebral spinal fluid leak causing spontaneous intracranial hypotension. BMJ Case Rep. 2015;2015:bcr2015011778.
- [CrossRef] [PubMed] [Google Scholar]
- Successful surgical treatment of intractable spontaneous intracranial hypotension due to a calcified thoracic disc prolapse. J Clin Neurosci. 2013;20:1773-5.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical intervention for spontaneous intracranial hypotension Type 4 CSF leak: A case report. Surg Neurol Int. 2020;11:421.
- [CrossRef] [PubMed] [Google Scholar]
- Sphenopalatine block with lidocaine spray for treatment of obstetric postdural puncture headache. J Clin Anesth. 2021;68:110069.
- [CrossRef] [PubMed] [Google Scholar]
- Sphenopalatine ganglion block for relieving postdural puncture headache: Technique and mechanism of action of block with a narrative review of efficacy. Korean J Pain. 2017;30:93-7.
- [CrossRef] [PubMed] [Google Scholar]
- A classification system of spontaneous spinal CSF leaks. Neurology. 2016;87:673-9.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous intracranial hypotension without CSF leakage-concept of a pathological cranial to spinal fluid shift. Front Neurol. 2021;12:760081.
- [CrossRef] [PubMed] [Google Scholar]
- Factors predicting response to the first epidural blood patch in spontaneous intracranial hypotension. Brain. 2017;140:344-52.
- [CrossRef] [PubMed] [Google Scholar]




