
Translate this page into:
Proprioceptive-Induced Reflex Postinfarct Seizures: A Rare Occurrence
Address for correspondence: Dr. Rohan Mahale, Department of Neurology, M.S. Ramaiah Medical College, Bengaluru - 560 054, Karnataka, India. E-mail: rohanmahale83@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
In reflex epilepsies, seizures are provoked by specific stimuli or, less commonly, mental processes and have seizures exclusively in response to particular stimuli without spontaneous seizures. It may coexist with spontaneously occurring seizures. Clinically, they manifest as partial or generalized seizures with either focal or generalized ictal epileptic discharges at onset.[1] Reflex seizures are precipitated by following stimuli: visual, somatosensory and proprioceptive, auditory, thinking, reading, music, startle, hot water, and eating. Proprioceptive-induced seizures are provoked by passive or active movement and are simple partial attacks presenting as tonic or clonic motor movements of a limb.[2] Here, we report a patient who had clonic movement of the left upper limb on forward abduction against gravity with corresponding epileptiform discharges from the right frontal region suggestive of possible proprioceptive-induced reflex seizures.
A 58-year-old man presented with involuntary movements of the left upper limb of 2 days duration. The movements used to appear on holding objects in the left upper limb or keep the limb abducted against gravity, aborted by keeping the limb at rest, or by holding the limb with the other. There were no sensory symptoms, twitching of face, or weakness in limbs. He had left faciobrachial weakness 3 months back which improved subsequently over 1 month. He was hypertensive on medication. On examination, he was conscious, alert, and oriented. Speech and cranial nerves were normal. Motor and sensory examination was normal. There was clonic/myoclonic movement of the left upper limb on forward abduction of limb against gravity, aborting on rest with no overflow to other region. He was fully alert and responsive during the attack [Video 1]. Deep tendon reflexes were normal and plantar responses were flexors. Complete hemogram, renal, liver and thyroid function tests, and serum electrolytes were normal. Glycosylated hemoglobin level was 6.5%. Brain magnetic resonance imaging showed right frontotemporal gliosis. Electroencephalogram (EEG) showed sharp wave discharges from the right frontal/anterior temporal region [Figure 1]. He was started on sodium valproate (1000 mg/day) and responded well.
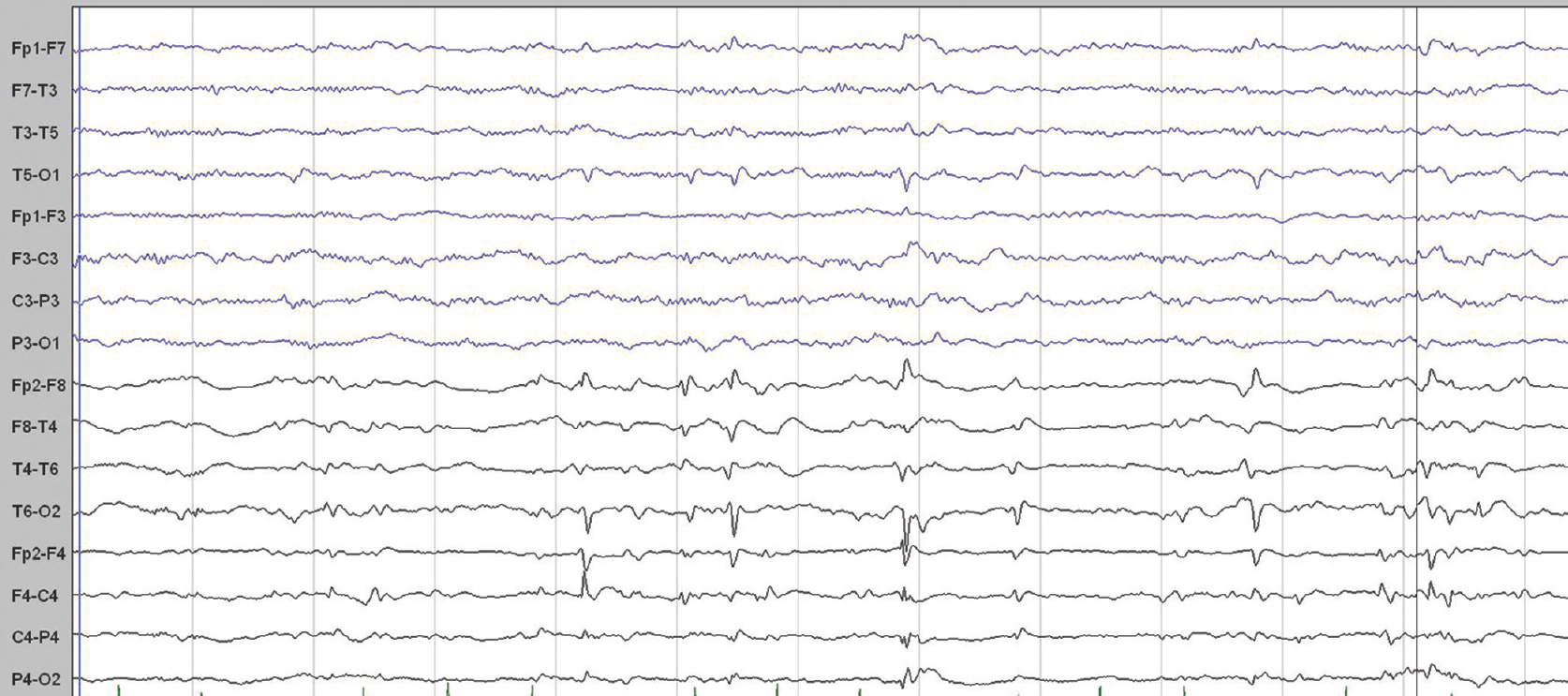
- Electroencephalogram (bipolar longitudinal montage, sensitivity 7.5 mV/mm, low-frequency filter 1 Hz, high-frequency filter 70 Hz, notch 50 Hz, speed 30 mm/s) shows sharp wave discharges from the right frontal/anterior temporal region
Proprioceptive-induced reflex seizures have been described more than 100 years ago by Gowers in 1901. They represent a specific group of epilepsy with the involvement of only a single anatomo-functional system; the sensorimotor network. The provoking stimulus and seizure seem to remain localized to the same functional brain network. Usually, the rolandic sensorimotor area or the supplementary motor area, contralateral to the clinical seizure onset, is involved. The proprioceptive information reaches the sensorimotor cortex which sends modifying impulses to influence the segmental monosynaptic reflex circuit and is termed as “long loop reflexes.”[3] The specific feature of the long loop activated during a proprioceptive-induced reflex seizure is the epileptic hyperexcitability of the involved cortical area. At present, these seizures are considered to represent “system epilepsies” wherein seizures remain in a closed anatomo-functional system showing their specific features. However, some consider this type of seizures as epileptically-enhanced stretch reflexes.[4] However, some refute that these types of seizures are dependent on the proprioceptive afferents as these seizures are not prevented by brachial plexus block. Clinically, proprioceptive-induced seizures are tonic or tonic–clonic with epileptiform discharges in the EEG as an accompaniment.
In our patient, the posture of the left upper limb was a possible trigger that resulted in increased stretch reflex afferent impulses to the hyperexcitable contralateral sensorimotor cortex which resulted in the focal motor seizure. The attacks could be aborted by keeping the limb in the resting position. The probable mechanism may be due to the modification of the central hyperexcitable circuit by the removal of proprioceptive inputs.
Postinfarct seizures can occur soon after the onset of ischemia or can be delayed. Early postinfarct seizures are defined as those first occurring within 2 weeks and late postinfarct seizures as those occurring after 2 weeks. Approximately, 50%–90% of early onset seizures appear to be simple partial seizures. Moreover, <1% of patients with ischemic stroke develop status epilepticus. Proprioceptive-induced reflex seizures have not been reported as subtype of postinfarct seizures.
Proprioceptive-induced seizures are a form of reflex focal motor epilepsy and are uncommon. Our patient had focal motor clonic seizures that were posture dependent with corresponding epileptiform discharges from the contralateral frontotemporal region. This may represent proprioceptive-induced reflex postinfarct seizure.
Video available on: www.ruralneuropractice.com
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- International League Against Epilepsy (ILAE). A proposed diagnostic scheme for people with epileptic seizures and with epilepsy: Report of the ILAE Task Force on Classification and Terminology. Epilepsia. 2001;42:796-803.
- [Google Scholar]
- Compulsive somatosensory self-stimulation inducing epileptic seizures. Epilepsia. 1992;33:509-16.
- [Google Scholar]
- Primary motor cortex and feedback control: Long-loop reflexes reflect joint mechanics and not joint motion. Eng Med Biol. 2003;4:3840-2. [Proceedings of the 25th Annual International Conference of the IEEE]
- [Google Scholar]
- Are proprioceptive-induced reflex seizures epileptically-enhanced stretch reflex manifestations? Epileptic Disord. 2012;14:149-54.
- [Google Scholar]




