
Translate this page into:
Parkisonism followed by burr hole drainage for chronic subdural hemorrhage
Address for correspondence: Dr. Cheng-Chia Lee, Department of Neurosurgery, Taipei Veterans General Hospital, No. 201, Sec. 2, Shih-Pai Road, Taipei 112, Taiwan. E-mail: yfnaughty@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Abstract
There have been few reports on secondary parkisonism caused by chronic subdual hemorrhage (CSDH). In most reports, rigidity-bradykinesia syndrome resolved gradually after decompressive operation for CSDH. We report a 74-year-old male patient who suffered from CSDH status post burr hole drainage twice, and followed secondary parkinsonism thereafter. Decompression by burr hole drainage was successful. However, the conscious level was still altered and the patient began to present with rigidity and bradykinesia. Fortunately, the symptoms dramatically improved after taking L-dopa. CSDH-related parkinsonism may have pre-operative nigrostriatal dysfunction, which can not compensate further insults to the basal ganglia. Prescription of L-dopa may be helpful in these patients
Keywords
Bradykinesia
burr hole drainage
chronic subdural hemorrhage
parkinsonism
rigidity

Introduction
Chronic subdural hematoma (CSDH) is not uncommon in the senior population. Burr hole drainage is the most widely used procedure to treat these patients. The efficacy of this procedure is excellent, although the recurrent rate is 2–18.5%. The clinical symptoms often improve dramatically. However, if not improved, or even progressed, the underlying cause must be evaluated carefully.
Case Report
A 74-year-old male veteran had type II diabetes mellitus, hypertension, vertebral-basilar insufficiency, and prostate cancer status post radical prostatectomy with complete cure. He could not manage his daily life and also went hiking in the mountains every week. One day, he had an accidental fall from the stairs. There was no initial loss of consciousness or any neurological deficits. Brain computerized tomography (CT) showed a normal aging appearance without hemorrhage. However, sudden-onset conscious loss was noted 1 week later, and a repeat brain CT showed left subdural hematoma with mass effect and midline shift [Figure 1a]. Emergent burr hole drainage was performed, but was still in drowsy status 10 days after the operation (E4V1M4). Brain CT showed mild residual hematoma, but no compression. Three weeks later, the left-side subdural hematoma was progressed [Figure 1b]. Moderate midline shift and ventricular dilation with sudden-onset declined conscious level (E1V1M1) demanded another operation. Emergent burr hole drainage and V-P shunt implantation were performed simultaneously. Conscious level returned to E4V1M5 [Figure 1c]. Dysarthria, mask face, rigidity, and bradykinesia were gradually present, especially over the left side. The patient was alert to verbal stimulus but could barely make any sound. Although his eye contact improved, cogwheel rigidity was progressively severe. Magnetic resonance imaging of the brain was performed to exclude the possible acute fine lesions such as infarctions, but could not identify any new organic lesion. Under the impression of secondary parkinsonism, L-dopa was prescribed (62.5 mg tid, titrated to 250 mg tid). The dysarthria, mask face, rigidity, and bradykinesia improved dramatically after the initiation of L-dopa treatment. Under ongoing rehabilitation, he can move with a walker and speak lots of stories.
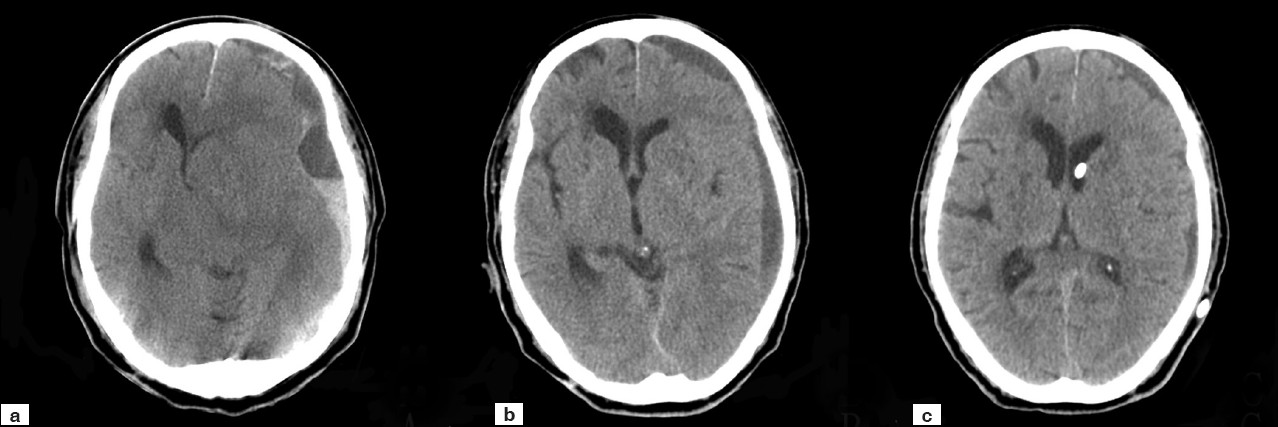
- Brain computed tomography series: (a) 1 week after falling down. Subdural hematoma (SDH) 16 mm in thickness at the left frontotemporoparietal area with midline shift. (b) Before the second operation of burr hole drainage and V-P shunt. SDH 10 mm in thickness at the same area with midline shift. Moderate ventricular dilatation with periventricular lucency. (c) Ten days after the second operation. Chronic SDH was in regression
Discussion
Secondary parkinsonism is a description of a group of symptoms including tremor, rigidity, bradykinesia, and postural instability. Parkinsonism is mainly caused by degeneration or damage of dopaminergic neurons in the basal ganglia. Rarely, parkinsonism may occur in CSDH patients. There have been about 20 cases of CSDH causing parkinsonism reported in the literature.[1–6] Some of them have underlying parkinsonism, and the others have newly onset parkinsonism after the development of CSDH. In the majority, the parkinsonism markedly improved after evacuation of the hematoma. However, the course of our patient is significantly different. He walked well without tremor, rigidity, and bradykinesia before the accident. After burr hole drainage performed twice for CSDH, the parkinsonism syndromes were gradually present, and improved after taking L-dopa. The mechanism causing parkinsonism in CSDH patients was not understood well. Mechanical compression of basal ganglia, vascular disturbances, and metabolic changes may be involved.[7–10] These possible causes may lead to a disturbance of the nigrostrial axis at different levels: the substantia nigra, nigrostriatal pathways, and the striatum.[8] Reduction of dopaminergic receptors has been reported in a patient with parkinsonism secondary to intracranial tumor who did not benefit from L-dopa.[7] Vascular disturbances resulted in impaired perfusion and decreased oxygen extraction and utilization. As a result, local increased tissue pressure onto the basal ganglia may also be relevant.[9] This hypothesis is supported by the biochemical and neuropathological findings in one case of parkinsonism due to brain tumor. Garcia de Y’ebenes et al. concluded that tumor compression resulted in damage to both the presynaptic dopaminergic nigrostriatal neurons and the postsynaptic dompamine receptors.[7] Likely, our patient with CSDH-related parkinsonism may have preoperative nigrostriatal dysfunction, which cannot compensate further insults to the basal ganglia. As soon as the intracranial pressure is elevated, even mild and transient, it may result in clinical symptoms.[610]
In conclusion, CSDH may cause or aggravate parkinsonism, and the symptoms could persist even after decompressive surgery. When the patient's recovery is not satisfactory after decompressive surgery, parkinsonism must be considered as a possible cause. The rigidity and bradykinesia should not be present in this group of patients, especially in an asymmetric pattern. Medical treatment with L-dopa may cause dramatic improvement.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Dopa-responsive parkinsonism after acute subdural hematoma. Eur J Neurol. 2006;13:e10-1.
- [Google Scholar]
- [Parkinsonism secondary to chronic subdural hematoma. A case report] No To Shinkei. 2006;58:873-8.
- [Google Scholar]
- Bilateral chronic subdural haematoma: A reversible cause of parkinsonism. J R Soc Med. 2006;99:91-2.
- [Google Scholar]
- Chronic subdural haematomas and Parkinsonian syndromes. Acta Neurochir (Wien). 1999;141:753-7. discussion 757-8
- [Google Scholar]
- Parkinsonism due to chronic subdural hematoma. Neurol Med Chir (Tokyo). 1996;36:99-101.
- [Google Scholar]
- Biochemical findings in a case of parkinsonism secondary to brain tumor. Ann Neurol. 1982;11:313-6.
- [Google Scholar]
- Striatal glucose metabolism and [18F]fluorodopa uptake in a patient with tumor-induced hemiparkinsonism. Neurosurgery. 1993;32:838-41.
- [Google Scholar]
- Parkinsonism associated with acute intracranial hematomas: An [18F]dopa positron-emission tomography study. Mov Disord. 1997;12:1035-8.
- [Google Scholar]




