
Translate this page into:
Management and Outcome of Infantile Hydrocephalus in a Tertiary Health Institution in Nigeria
Address for correspondence: Dr. Habeeb Kayodele Omokanye, Department of Otorhinolaryngology, College of Health Sciences, University of Ilorin/University of Ilorin Teaching Hospital, PMB 1459, Ilorin 240001, Kwara State, Nigeria. E-mail: habeebomokanye@yahoo.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Hydrocephalus is a leading cause of disability among children worldwide. The outcome depends on morphology and whether insult is pre- or post-natal. There has been improvement in morbidity in developed countries due to improved surgical care. A paucity of trained personnel impacts negatively on care and outcome of infants with hydrocephalus in many low-income countries resulting poorer outcome. We conducted an audit of patients with hydrocephalus managed in our institution to determine common etiology and outcome.
Object:
The objective of this retrospective review was to conduct an audit of hydrocephalus care in our institution.
Materials and Methods:
Information was retrieved from case notes, ward records, imaging results, operation notes, and follow-up clinic charts. Type of hydrocephalus, onset, treatment offered, outcome, complications, and follow-up duration were documented.
Results:
Management of 58 infants with complete data was analyzed. Most hydrocephalus 40 (69%) were congenital with 14 (35%) occurring in association with myelomeningocele and 8 patients confirmed with aqueductal stenosis. Ventriculoperitoneal shunts insertion 53 (91%) was the most common treatment modality.
Conclusions:
There is need to improve surgical intervention in the form of endoscopic third ventriculostomy in suitable patients. Subsiding cost of care may be considered for indigent patients.
Keywords
Cerebrospinal fluid shunt
hydrocephalus
infant

INTRODUCTION
Hydrocephalus is the most common condition treated by pediatric neurosurgeons.[1] Ventriculoperitoneal shunt (VPS) remains the most common treatment for hydrocephalus world over even though it is associated with several short- and long-term complications.[2] As shunt system continues to evolve over the years to improve the outcome of the procedure; surgeons have also devised other alternative and safer techniques for the treatment of hydrocephalus. The advent of endoscopes ushered in the endoscopic third ventriculostomy (ETV) technique and later endoscopic choroid plexus cauterization (CPC) as alternatives to shunting for hydrocephalus in 1995.[123] Even then, there had been reported low success rate when used alone in some patients.[456] Hence, the recent popularization of combined ETV + CPC technique as a relatively safe means of increasing the overall treatment outcome success and avoiding the need for a shunt in infants with hydrocephalus.[2789]
Despite of the recent advances in technology, VPS remains the most widely performed procedure for hydrocephalus in infants. Various shunt valve designed have been developed to improve the success rate of shunting for hydrocephalus. The general trends in developed country are the use of programmable shunt valves. In low-income country like Nigeria, however, low cost, fixed pressure shunt valve system is widely used.
This study was undertaken as an audit of infant hydrocephalus management in our institutions where fixed-pressure slit-in spring Chhabra ventriculoperitoneal shunt device is traditionally used.
MATERIALS AND METHODS
This study included infants (<12 months) with hydrocephalus managed in our neurosurgical division over 3 years. Our institution has a facility for transcranial ultrasound, computed tomographic scan, and magnetic resonant imaging machines. The diagnosis of hydrocephalus was based on clinical and neuroradiologic evaluations. Data were collected retrospectively through review of case files, imaging reports, ward records, operative notes, and follow-up clinic charts. Information on demography, etiology, type and onset of hydrocephalus, treatment offered, complication, and outcome of care were retrieved using a predesigned pro forma. The main outcome measures were developmental milestones attained for age, complications, and death. Data were entered into 2011 IBM SPSS (Statistical Package for social sciences) software for windows, version 20; Armonk, NY (IBM Inc.). Frequency tables and figures were used to illustrate results.
RESULTS
Fifty-eight infants constituting 76% of a total of 76 patients with hydrocephalus were treated between 2012 and 2014. Case files of these infants were retrospectively studied. There were 33 males (57%) and 25 females (43%) with male to female ratio of 1.3:1. Age of patient ranged between 3 and 12 months with a median age of 3 months (±standard deviation of 4.2 ± 2 months). The most common age group in this study was 1–6 months 33 (57%), while the 7–12 months age group had the least frequency 9 (15%) [Table 1].
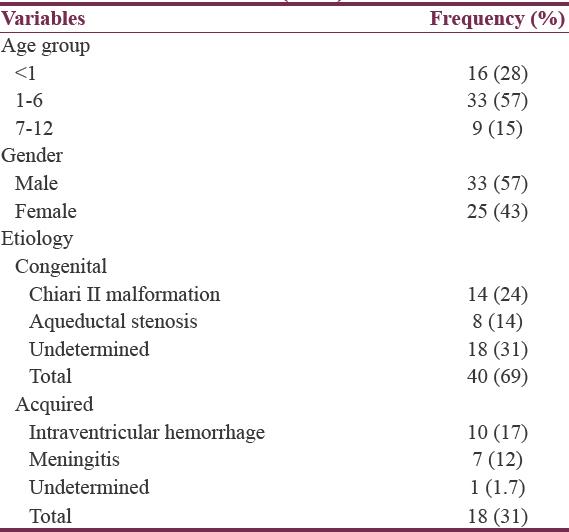
A large proportion had an undetermined cause of their hydrocephalus 18 (31%). Of those with an identifiable congenital cause, the majority was due to Chiari II malformation 14 (24%) while intraventricular hemorrhage (IVH) was the most common acquired cause 10 (17%) [Table 1 and Figure 1]. In general, congenital hydrocephalus was more common 40 (69%) than acquired type 18 (31%) [Figures 2–4].
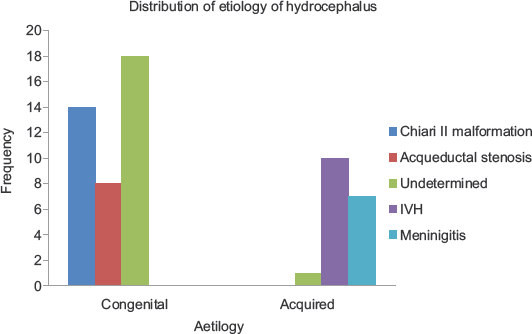
- Diagnosis and frequency of occurrence
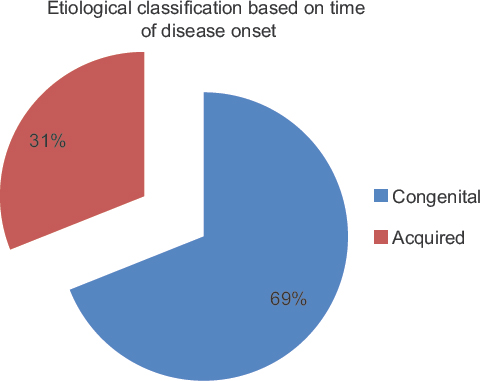
- Classification of hydrocephalus based on the time of onset

- Typical hydrocephalus

- Neglected congenital hydrocephalus
The majority of the patients 27 (47%) had communicating hydrocephalus, whereas noncommunicating type was seen in 17 (29%). VPS was the neurosurgical treatment offered in most of the cases 53 (91%), followed by 3 (3.4%) ETV, and 2 (1.7%) ventriculosubgaleal (VSG) shunt [Figure 5], respectively [Table 2].

- (a) Subgaleal pouch following ventriculosubgalial shunt. (b) Postconversion of ventriculosubgaleal shunt to ventriculoperitoneal shunt
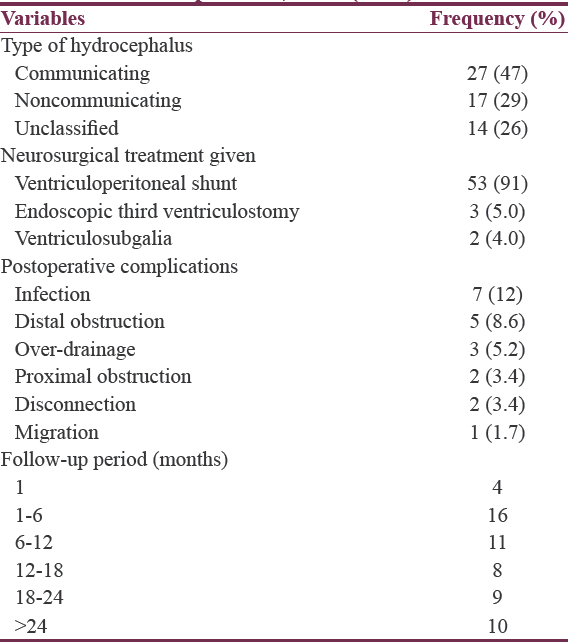
Infection was found to be the most common postoperative complication 7 (12%) in this series, followed by distal obstruction 5 (8.6%) while migration of shunt was the least complication experienced by patients 1 (1.7%). There were 2 perioperative deaths giving a mortality rate of 3.4%. One of the deaths was due to respiratory arrest in an infant with Chiari II malformation while the other patient was a preterm with IVH. The actual cause of death was not documented in the preterm. As at last follow up, most patients 38 (65.5%) were assessed has having satisfactory outcome based on developmental milestones attained for age.
DISCUSSION
A total of 76 patients with hydrocephalus were treated in our facility in 3 years between January 2012 and December 2014 under review. This figure is undoubted disproportionate to the incidence of the disease in the community. Poverty, stigmatization, traditional beliefs, and poor awareness of the amenability of hydrocephalus to orthodox medicine remain strong negative factors preventing hospital presentation in Sub-Sahara Africa. On the other hand, approximately 69,000 annual hospital admissions for hydrocephalus were recorded in the United States where awareness and access to health care are much better.[1011]
This series recorded a slight male preponderance in the incidence of hydrocephalus [Table 1] with a male to female ratio of 1.3:1 which is similar to the reports in other parts of Nigeria and America.[10121314] There was no obvious reason for this finding.
Hydrocephalus is predominantly a disease of infants; hence, the age range of 3–12 months with a median age of 3 months found in these studies. This is in keeping with findings in earlier studies.[1014] The most common age group in this study was 1–6 months 33 (57%), the cranial sutures are yet to fuse at this early age and pressure created by accumulation of cerebrospinal fluid (CSF) in the ventricles causes a back pressure effect on the cranium, widening the sutures, and expanding the head circumference (mega cranium); a feature pathognomonic of hydrocephalus in childhood.[15]
Chiari II malformation in infants with lumbosacral myelomeningocele was the most common cause of hydrocephalus, followed by IVH in these infants [Table 1 and Figure 1]. This is a reversal of the etiological pattern reported by Kulkarni et al. where IVH was the most common, followed by aqueductal stenosis.[2] In our series, however, the precise cause of the disease could not be determined in a significant number of cases 19 (32.7%). This is mostly due to financial constraints, which limited imaging and other necessary investigations that could have been done to confirm the diagnosis. In Nigeria, National Insurance scheme is yet to cover all citizens, especially the informal sector and the rural dwellers.[16] Hence, hospital bills are settled out of pocket with individual patient taking full responsibility for his or her hospital bills. For the same reason, indigent parents generally find it difficult to finance the care of their sick child [Figure 4]. Besides, hospital is usually the last point of call after exhausting their meager resources-seeking alternative healthcare at traditional homes and faith healing homes.[17]
In general, congenital hydrocephalus was more common than acquired type, and the majority of patients had communicating hydrocephalus, [Figure 2]. VPS was the neurosurgical treatment offered in most of the cases 53 (91%), followed by 3 (3.4%) ETV, and 2 (1.7%) VSG, respectively [Table 2]. VPS remains the most commonly performed treatment procedure for hydrocephalus despite all its pitfalls.[2] Endoscopic procedure is a relatively new technique in our practice, the 3 patients who had ETV had good outcome without complications. Good outcome from ETV among childhood hydrocephalus has been previously reported in Nigeria and other part of the world. There are on-going controversies on the efficacy of ETV in infant hydrocephalus management. A retrospective, multicenter North American study has suggested ETV + CPC as a relatively safe procedure with improve treatment success.[2] In Nigeria, a success rate of 75% has been reported with ETV + CPC in childhood hydrocephalus.[14] Our unit practice is likely to move toward ETV as preferred procedure in suitable infants following this audit. VSG procedure was undertaken for 3 of our patients with IVH as a temporizing measure. All of these were subsequently converted to VPS when the CSF became clear [Figure 5].
Infection was found to be the most common postoperative complication 7 (12%), in this series, followed by distal obstruction 5 (8.6%) while migration of shunt was the least complication experienced by 1 patient (1.7%). The prevalence of infection (12%) record in this study falls within the variable rates of 2.2%–39% reported in earlier studies.[1819] and it tallies with the overall infection rate of 11.7% reported by Simon et al. in a study of over 7000 children after shunt placement in America.[20] Even though it is higher than 6.98% observed by Wu et al. in a similar study in china.[21] The prevalence of infection is generally high in the developing tropical countries like Nigeria. However, Simon et al.'s study were done before the advent of antibiotics impregnated shunts which explain why the infection rate was close to our findings.[20] Aside from type of shunt implanted, other predisposing factors to shunt infection include age of patients at shunt insertion, cause of hydrocephalus and perioperative antibiotics, operative room traffic, duration of the shunt placement operation, experience of the neurosurgeon, and cause of hydrocephalus.[2223] Further studies of the role of these variables in etiology of shunt infections will be a valuable future research direction. Double gloving, prophylactic antibiotics, shunt impregnated with antibiotics usually rifampicin and clindamycin are reported to reduce shunt infections.[24] Most commonly implicated organisms in shunt-associated infections are coagulase-negative Staphylococcus and Staphylococcus aureus and other skin bacteria followed by Gram-negative bacteria.[21] Microbiology report was not studied in our series.
CONCLUSIONS AND RECOMMENDATION
There is need to improve surgical intervention in the form of ETV in suitable patients. Subsidizing cost of care may be considered for indigent patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Pediatric Hydrocephalus Systematic Review and Evidence-Based Guidelines Task Force. Pediatric hydrocephalus: Systematic literature review and evidence-based guidelines. Part 5: Effect of valve type on cerebrospinal fluid shunt efficacy. J Neurosurg Pediatr. 2014;14(Suppl 1):35-43.
- [Google Scholar]
- Endoscopic third ventriculostomy and choroid plexus cauterization in infants with hydrocephalus: A retrospective hydrocephalus clinical research network study. J Neurosurg Pediatr. 2014;14:224-9.
- [Google Scholar]
- Endoscopic adjuncts to intraventricular surgery. Neurosurg Clin N Am. 2003;14:547-57.
- [Google Scholar]
- Canadian Pediatric Neurosurgery Study Group. Endoscopic third ventriculostomy in pediatric patients: The Canadian experience. Neurosurgery. 2007;60:881-6.
- [Google Scholar]
- Long-term reliability of endoscopic third ventriculostomy. Neurosurgery. 2008;62(Suppl 2):614-21.
- [Google Scholar]
- Canadian Pediatric Neurosurgery Study Group. Endoscopic third ventriculostomy in the treatment of childhood hydrocephalus. J Pediatr. 2009;155:254-9.e1.
- [Google Scholar]
- Endoscopic third ventriculostomy in the treatment of childhood hydrocephalus in Uganda: Report of a scoring system that predicts success. J Neurosurg Pediatr. 2010;5:143-8.
- [Google Scholar]
- Combined endoscopic third ventriculostomy and choroid plexus cauterization as primary treatment of hydrocephalus for infants with myelomeningocele: Long-term results of a prospective intent-to-treat study in 115 East African infants. J Neurosurg Pediatr. 2008;2:310-6.
- [Google Scholar]
- Comparison of endoscopic third ventriculostomy alone and combined with choroid plexus cauterization in infants younger than 1 year of age: A prospective study in 550 African children. J Neurosurg. 2005;103(6 Suppl):475-81.
- [Google Scholar]
- Revision rate of pediatric ventriculoperitoneal shunts after 15 years. J Neurosurg Pediatr. 2013;11:15-9.
- [Google Scholar]
- Hydrocephalus Clinical Research Network. Hospital care for children with hydrocephalus in the United States: Utilization, charges, comorbidities, and deaths. J Neurosurg Pediatr. 2008;1:131-7.
- [Google Scholar]
- Treatment of cerebrospinal fluid shunting complications in a Nigerian neurosurgery programme. Case illustrations and review. Pediatr Neurosurg. 2008;44:36-42.
- [Google Scholar]
- Efficacy of endoscopic third ventriculostomy in the management of hydrocephalus in children under 2 years of age: Experience from a tertiary institution in Nigeria. Niger J Clin Pract. 2015;18:318-22.
- [Google Scholar]
- Early outcome of combined endoscopic third ventriculostomy and choroid plexus cauterization in childhood hydrocephalus. J Neurosurg Pediatr. 2015;15:524-8.
- [Google Scholar]
- Benign external hydrocephalus: A review, with emphasis on management. Neurosurg Rev. 2011;34:417-32.
- [Google Scholar]
- Nigeria's National Health Insurance Scheme: A critical reappraisal. Savannah J Med Res Pract. 2012;1:1-6.
- [Google Scholar]
- Vagal reflex stimulation complicating retrieval of an unusual foreign body from the laryngotracheal lumen: Case report. Egypt J Anaesth. 2016;32:237-40.
- [Google Scholar]
- Infection of cerebrospinal fluid shunts in infants: A study of etiological factors. J Neurosurg. 1992;77:29-36.
- [Google Scholar]
- Randomized trial of cerebrospinal fluid shunt valve design in pediatric hydrocephalus. Neurosurgery. 1998;43:294-303.
- [Google Scholar]
- Infection rates following initial cerebrospinal fluid shunt placement across pediatric hospitals in the United States. Clinical article. J Neurosurg Pediatr. 2009;4:156-65.
- [Google Scholar]
- Prevention options for ventriculoperitoneal shunt infections: A retrospective analysis during a five-year period. Int J Clin Exp Med. 2015;8:19775-80.
- [Google Scholar]
- Timing of cranioplasty after decompressive craniectomy for ischemic or hemorrhagic stroke. J Neurosurg. 2013;118:109-14.
- [Google Scholar]
- Ventriculoperitoneal shunt surgery and the risk of shunt infection in patients with hydrocephalus: Long-term single institution experience. World Neurosurg. 2012;78:155-63.
- [Google Scholar]
- Conservative management of patients with cerebrospinal fluid shunt infections. Neurosurgery. 2006;58:657-65.
- [Google Scholar]




