
Translate this page into:
Cranial index of children with normal and abnormal brain development in Sokoto, Nigeria: A comparative study
Address for correspondence: Mr. Muhammad Awwal Musa, Department of Anatomy, College of Health Sciences, Usmanu Danfodiyo University, PMB - 2346, Sokoto, Nigeria. E-mail: musa.muhammadawwal@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Abnormal brain development due to neurodevelopmental disorders in children has always been an important concern, but yet has to be considered as a significant public health problem, especially in the low- and middle-income countries including Nigeria.
Aims:
The aim of this study is to determine whether abnormal brain development in the form of neurodevelopmental disorders causes any deviation in the cranial index of affected children.
Materials and Methods:
This is a comparative study on the head length, head width, and cranial index of 112 children (72 males and 40 females) diagnosed with at least one abnormal problem in brain development, in the form of a neurodevelopmental disorder (NDD), in comparison with that of 218 normal growing children without any form of NDD (121 males and 97 females), aged 0-18 years old seen at the Usmanu Danfodiyo University Teaching Hospital, Sokoto, over a period of six months, June to December, 2012. The head length and head width of the children was measured using standard anatomical landmarks and cranial index calculated. The data obtained was entered into the Microsoft excel worksheet and analyzed using SPSS version 17.
Results:
The mean Cephalic Index for normal growing children with normal brain development was 79.82 ± 3.35 and that of the children with abnormal brain development was 77.78 ± 2.95 and the difference between the two groups was not statistically significant (P > 0.05).
Conclusion:
It can be deduced from this present study that the cranial index does not change in children with neurodevelopmental disorders.
Keywords
Abnormal brain development
brain growth
children
cranial index
head shape
neurodevelopmental disorder

Introduction
Biological variation allows for a unique craniofacial character and many asymmetries found in each individual.[1] A neurodevelopmental disorder has been defined as an impairment of the growth and development of the brain or central nervous system. A narrower use of the term refers to a disorder of the brain function that affects emotion, learning ability, and memory, which unfolds as the individual grows.[2] Disorders considered neurodevelopmental in origin or that have neurodevelopmental consequences when they occur in infancy and childhood include: Autism and autism spectrum disorders such as Asperger syndrome, Fetal alcohol spectrum disorder, Traumatic brain injury, (including congenital injuries such as those that cause cerebral palsy), Communication, speech, and language disorders, Genetic disorders, such as, fragile-X syndrome, and Down syndrome.[3]
The definition of children with a neurodevelopmental disorder or a neurodevelopmental impairment has varied in several studies.[4567] For the purpose of this study, we have tried as far as possible to apply a definition of children with abnormal brain development, due to neurodevelopmental disorder, to include all children who have been fully diagnosed with any form of abnormality that appears likely to affect day-to-day function, such as, a developmental quotient more than two standard deviations below the normal mean, a diagnosis of neuromotor impairment, including cerebral palsy (CP), speech and language disorders, hearing and vision impairment, attention-deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD), epilepsy, learning disorders (LD), and mental retardation (MR).[78] Neurodevelopmental disabilities (NDDs) among children have always been an important concern, but yet to be considered as a significant public health problem, especially in the low- and middle-income countries, including Nigeria. This is probably due to the fact that attention and resources are focused on more widely prevalent and visible vaccine-preventable childhood diseases, infections, nutritional deficiencies, and neonatal issues.[8] It is implicated that 85% of the children with NDDs live in low- and middle-income countries (LMICs) however; there is very little evidence to support this. Paucity of documented data regarding the prevalence of NDDs and their risk factors in LMICs, further aggravates the problem. There is also no comprehensive, valid, reliable, and culturally sensitive screening tool for multiple NDDs that can be used in resource-constraint environments.[8]
The importance of conducting craniometric or cephalometric studies cannot be overemphasized especially in the areas of pediatrics, plastic surgery, oral surgery, and forensic medicine.[910] Cranial index (CI) is one of the clinically recognized anthropometric parameters used in the investigation of a craniofacial skeleton, because of its validity and practicability.[11] The cranial index is the most investigated craniofacial parameter, as it utilizes the length and breadth of the head which are very helpful in the study of secular trends.[121314] The cranial index is used to determine variations in the shape of the head and face in newborns,[15] and to determine the head dimensions in fetuses.[16]
However, due to paucity of data on the physical or morphometric cranial indices of children with abnormal brain development due to neurodevelopmental disorders (NDDs) in the low- and middle-income countries, including Nigeria,[8] this study aims to discern whether abnormal brain development in the form of a neurodevelopmental disorder can cause any deviation in the cranial index of affected children, and thus, probably, serve as a baseline reference measurement for growth monitoring and evaluation.
Materials and Methods
Study location
This study was conducted in the Pediatric Neurology Clinic (PNC) of the Institute of the Child Health Unit, Usmanu Danfodiyo University Teaching Hospital, Sokoto, for over a period of six months, by applying the inclusion and exclusion criteria for the study.
Measurements and procedures
Cranial measurements such as head lengths and head widths were taken from 330 children of the pediatric age group 0-18 years, who visited the clinic during the period of study. The subjects comprised of 112 children who had been diagnosed with at least one form of abnormal brain development as a result of neurodevelopmental disorder by the Pediatric Neurology Department of UDUTH, and who attended the Pediatric Neurology Clinic. Two hundred and eighteen normal growing children without any abnormal brain development on routine check up at the center were also recruited in this study. Children with craniofacial malformations or a history or signs of craniofacial syndromes were excluded from this study. The bio-data of the subjects were obtained and this includes their names, hospital card numbers, sex, and age. Measurements were taken using the standard recognized anatomical landmarks. Internationally accepted anthropometric instruments were used to ensure great accuracy and reproducibility. All measurements were taken to the nearest 0.1 cm.
The head length (greatest anteroposterior diameter) and head width (maximum transverse diameter between two fixed points) were measured with the help of a spreading caliper.[1718] The head length was measured from the glabella to inion. The spreading caliper with rounded ends was used. The tips were made to touch the cranial points and the reading was observed on the scale.
The cranial index was calculated as the ratio of the head width to head length multiplied by 100. The cranial index was used to classify the head shapes into four international categories namely dolichocephalic (CI = <74.9), mesocephalic (CI = 75-79.9) brachycephalic (CI = 80-84.9) and hyperbrachycephalic (CI = >85).[919]
Ethical consideration
Ethical clearance was obtained from the relevant Institutions and Departments, for this study. The research was approved by the Ethics Committee of the College of Health Sciences, Usmanu Danfodiyo University, Sokoto. Ethical consideration included taking informed consent from the parents or guardians of study participants, using Hospital card numbers, to maintain confidentiality and making recommendations to the appropriate authorities.
Data analysis
The data obtained from the measurements of the head length and head width were used in determining the cranial index. The measurement values were entered and analyzed using the Statistical Package for Social Sciences (SPSS) Version 17 for Windows. Descriptive Statistics are presented in Tables 1–3. The student's t test was used for comparison between the means and the statistical significance was set at P < 0.05.

Results
Table 1 presents a summary of the neurodevelopmental disorders seen during the course of this study.
Tables 2 and 3 present the mean ± SD values of the cranial index of children with neurodevelopmental disorders (NDDs) and that of normal growing children without NDDs. All measurements were age-related. On an average, children with NDDs had a lower cranial index (mean CI = 77.78 ± 2.95) than those of normal growing children without NDDs (mean CI = 79.82 ± 3.35).
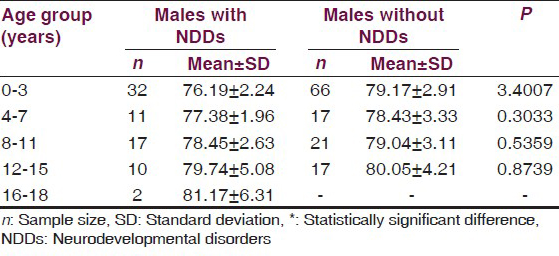
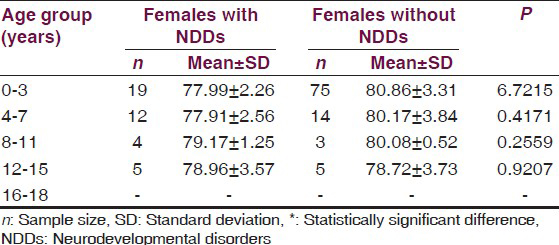
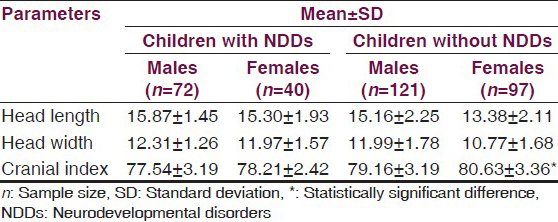
However, the mean cranial index for the males with NDDs was 77.54 ± 3.19 as against 79.16 ± 3.19 of the normal growing males without NDDs, while that of the females varied from 78.21 ± 2.42 for those with NDDs to 80.63 ± 3.36 in normal growing females without NDDs. Statistically, all the age groups in males with NDDs when compared to the normal growing children, showed no significant difference (P > 0.05) except for the age group of 16-18 years, where the difference was statistically significant (P < 0.05) as presented in Table 1. The female children with NDDs did not show any statistical significant difference in comparison to the normal growing female children without NDDs, as shown in Table 3.
Furthermore, the differences in cranial index between the sexes in children with NDDs was not significant (P = 0.2131), but it was statistically significant in the normal growing children without NDDs (P = 0.002).
Discussion
The present study shows that the cranial index values in children with NDDs are similar to those of the normal growing children without NDDs, in every age group. Generally, the children with NDDs had a lower cranial index (mean CI = 77.78 ± 2.95) than those of normal growing children (mean CI = 79.82 ± 3.35), but this difference was not statistically significant. These values were higher when compared to the 72.96 ± 6.12 cephalic index mean value found in the Ogbia children from Nigeria[20] and lower when compared to 80.42 from Chile.[19]
The overall minimum value for cranial index reported in this study was 68.39% and the maximum value was 89.29%. In the group of children with NDDs, the mean cranial index was 77.54 ± 3.19 in males and 78.21 ± 2.42 in females, while in the group of children without NDDs, the mean cranial index was 79.16 ± 3.19 in males and 80.62 ± 3.36 in females [Table 4]. It was observed from both groups that the mean values of females in this present study was higher than that of males and these differences were not statistically significant, with a P value > 0.05. These agreed with a previous study,[21] which reported higher cephalic index values in females than males, while our findings did not agree with any previous study that reported a statistically significant difference between the cephalic index of both sexes.[2022]
The mean cranial index values in both sexes are lower than the mean cephalic index values of 82.42 ± 5.38 (higher value) and 81.00 ± 5.35 (lower value) in males and females, respectively, found in children from Bangalore,[22] and also lower than the mean values of 83.10 in males and 84.60 in females from the Gurung community.[21] This implies that the cephalic index can be higher in any sex, depending on the peculiarity of the population under study.
The mean cranial index values observed in both males and females without NDDs are higher than those reported in the Ogbia children, who showed values of 73.68 ± 6.53 for males and 72.24 ± 5.60 for females.[20] Although, the mean cranial value for females in the group of children without NDDs is higher and very similar to the 80.08 mean cephalic index value found in females from Port Harcourt, Nigeria,[23] those of their male counterparts is lower than the 79.73 mean cephalic index value for males from Port Harcourt.[23]
The minimum cranial index value for females was 71.43% and maximum value 89.29%. The maximum cranial index value of females in this study is slightly higher than that reported in a previous study,[22] whose minimum and maximum cranial index values in females was 72 and 87%, respectively, while the minimum value of females in the present study is also slightly lower than that reported by Maria et al.[22] For the normal growing males without NDDs, the minimum and maximum cranial index values in this study (68.39 and 86.96%, respectively) are not the same as those in the study by Maria et al.,[22] even though the maximum cranial index value in males, 93%, is higher than the maximum value of cranial index of males in this study (86.96%) and the minimum cephalic index reported in male children,[22] (72%), is higher than the minimum cranial index value of 68.39% for males reported in this study. However, for both sexes in the group of children without NDDs, the minimum cranial index values in the present study are slightly lower when compared to the minimum values reported in previous studies.[22] An explanation for this is that it may be due to the difference in the range of the children's age group studied. However, the unsteady increase and decrease in the mean cranial index of females with NDDs, with an increase in age, observed in this study, agrees with the earlier study,[23] while the steady decrease in cranial index of females without NDDs does not agree with the study of Ligha and Fawehinmi.[23]
The increase in mean cranial index across all age groups observed in males with NDDs agrees with the reported increase in mean cephalic index with increase in age of normal growing male children from Port Harcourt, Nigeria,[23] while the unsteady increase and decrease seen in males without NDDs does not agree with the study by Ligha and Fawehinmi.[23] There was no statistically significant difference observed in the mean cranial index between the two groups and across the age ranges.
On an average, the mean cranial index values of females in the present study are higher when compared to those of males across all age groups. These higher mean head width values observed in females could be due to the nondominant lateral direction of expanding of the neural mass, by neural fibers, in females.[1324]
Conclusion
Conclusively, we can deduce from this present study that the Cephalic Index in children does not change due to neurodevelopmental problems. The present data can be of clinical importance in determining the timing and etiology of brain insults, especially during the critical period of brain development, as well as, help in the early identification and management of neurological abnormalities. It is recommended that further studies be conducted, possibly with a larger sample size, to corroborate these findings, so as to make further inference with regard to the clinical and anthropometric importance of such studies.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Handbook of Neurodevelopmental and Genetic Disorders in Children. New York: The Guilford Press; 1999. p. :3-8.
- [Google Scholar]
- Is schizophrenia a neurodevelopmental disorder? Br Med J (Clin Res Ed). 1987;295:681-2.
- [Google Scholar]
- A Controlled trial of dexamethasone in preterm infants at high risk for bronchopulmonary dysplasia. N Engl J Med. 1989;320:1505-10.
- [Google Scholar]
- Early dexamethasone therapy in preterm infants: A follow-up study. Pediatrics. 1998;101:E7.
- [Google Scholar]
- Randomized placebo-controlled trial of a 42-day tapering course of dexamethasone to reduce the duration of ventilator dependency in very low birth weight infants: Outcome of study participants at 1-year adjusted age. Pediatrics. 1999;104:15-21.
- [Google Scholar]
- The adverse neuro-developmental effects of postnatal steroids in the preterm infant: A systematic review of RCTs. BMC Pediatr. 2001;1:1.
- [Google Scholar]
- INCLEN Study (2011). Neuro developmental disabilities among children in India? Available from: http://inclentrust.org/pagephpid=246
- [Google Scholar]
- Gray's Anatomy. In: Skeletal System (38th ed). London: Elbs with Churchill Livingston; 1995. p. :607-12.
- [Google Scholar]
- Morphological evaluation of head in Turkman males in Gorgan-North of Iran. Int J Morphol. 2007;25:99-102.
- [Google Scholar]
- Size and shape measurement in contemporary cephalometrics. Eur J Orthod. 2003;25:231-42.
- [Google Scholar]
- Cephalometry in 14-18 years old girls and boys of Shiraz-Iran High School. Int J Morphol. 2009;27:101-4.
- [Google Scholar]
- The variation of head and face shapes in females newborns in the southeast of the Caspian Sea (mean Gorgam) Eur J Anat. 2005;9:95-8.
- [Google Scholar]
- Cephalic index of foetuses of Manipuri Population--A baseline study. J Anat Soc India. 2001;50:8-10.
- [Google Scholar]
- New scaphocephaly severity indices of sagittal craniosynostosis: A comparative study with cranial index quantifications. Cleft Palate Craniofac J. 2006;43:211-21.
- [Google Scholar]
- Practical Anthropometry. (4th ed). Philadelphia: The Wistar Institute of Anatomy and Biology; 1956. p. :87-9.
- [Google Scholar]
- Cephalic index in a group of mapuche individuals in the IX Region of Chile. Int J Morphol. 2005;23:241-6.
- [Google Scholar]
- Cephalic index of Gurung community of Nepal--an anthropometric study. Kathmandu Univ Med J (KUMJ). 2005;3:263-5.
- [Google Scholar]
- Cephalometry of mentally challenged subjects and correlation with intelligence quotient. Anatomica Karnataka. 2011;5:60-5.
- [Google Scholar]
- Canthal and cephalic indexes of children with homozygous sickle cell disease in Port-Harcourt. Niger J Med. 2011;20:33-8.
- [Google Scholar]
- Relationship between growth pattern and head dimensions in Nigerian children (5-15 years) Int J Biol Anthropol. 2008;2(1) DOI: 10.5580/a80
- [Google Scholar]




