
Translate this page into:
An Uncommon Cause of Dysarthria in an Elderly Gentleman
Shakya Bhattacharjee, MRCP (UK) Department of Neurology, Plymouth Hospital NHS Trust Plymouth PL6 8DH United Kingdom bubai.shakya@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Private Ltd. and was migrated to Scientific Scholar after the change of Publisher.
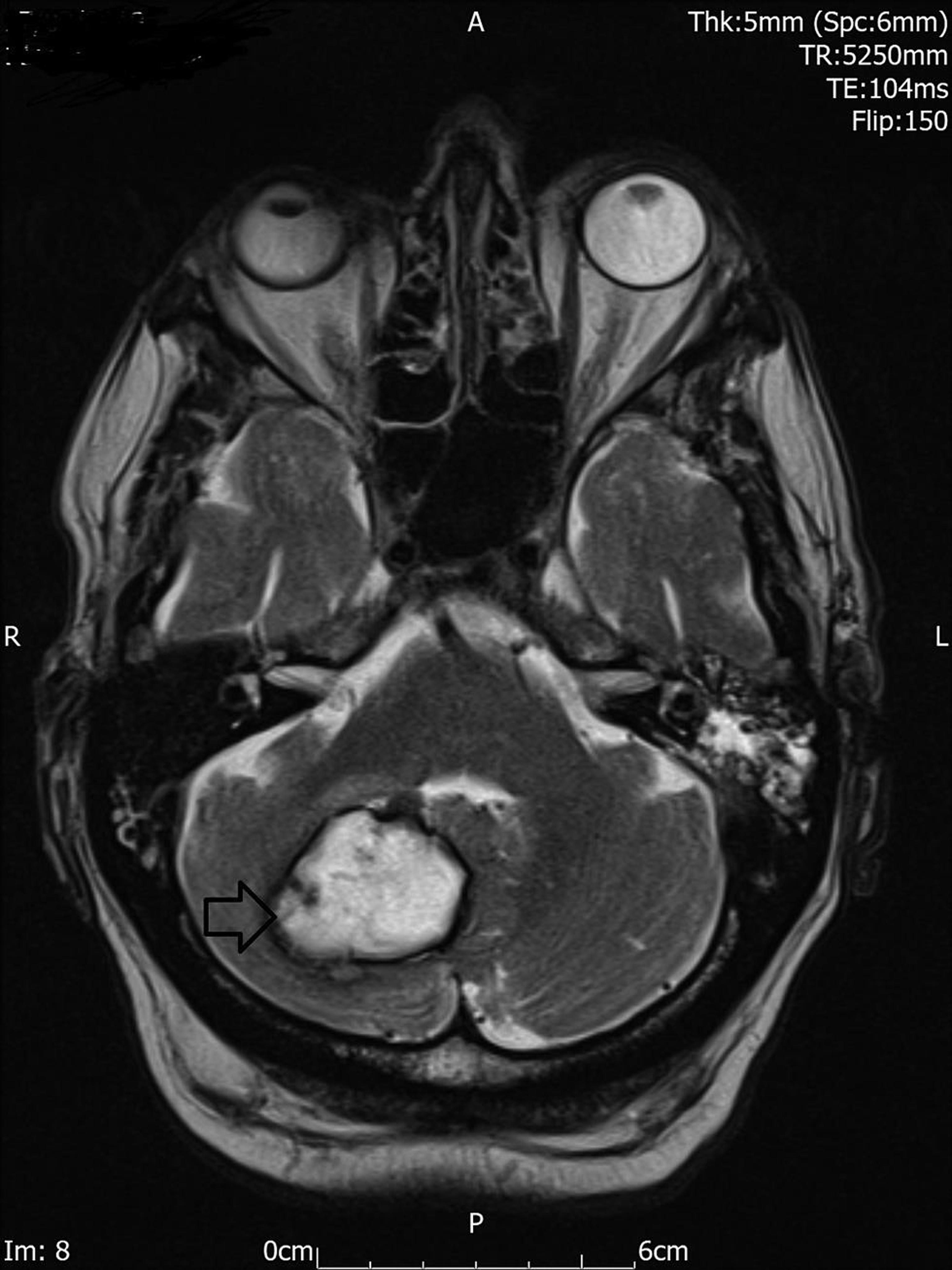
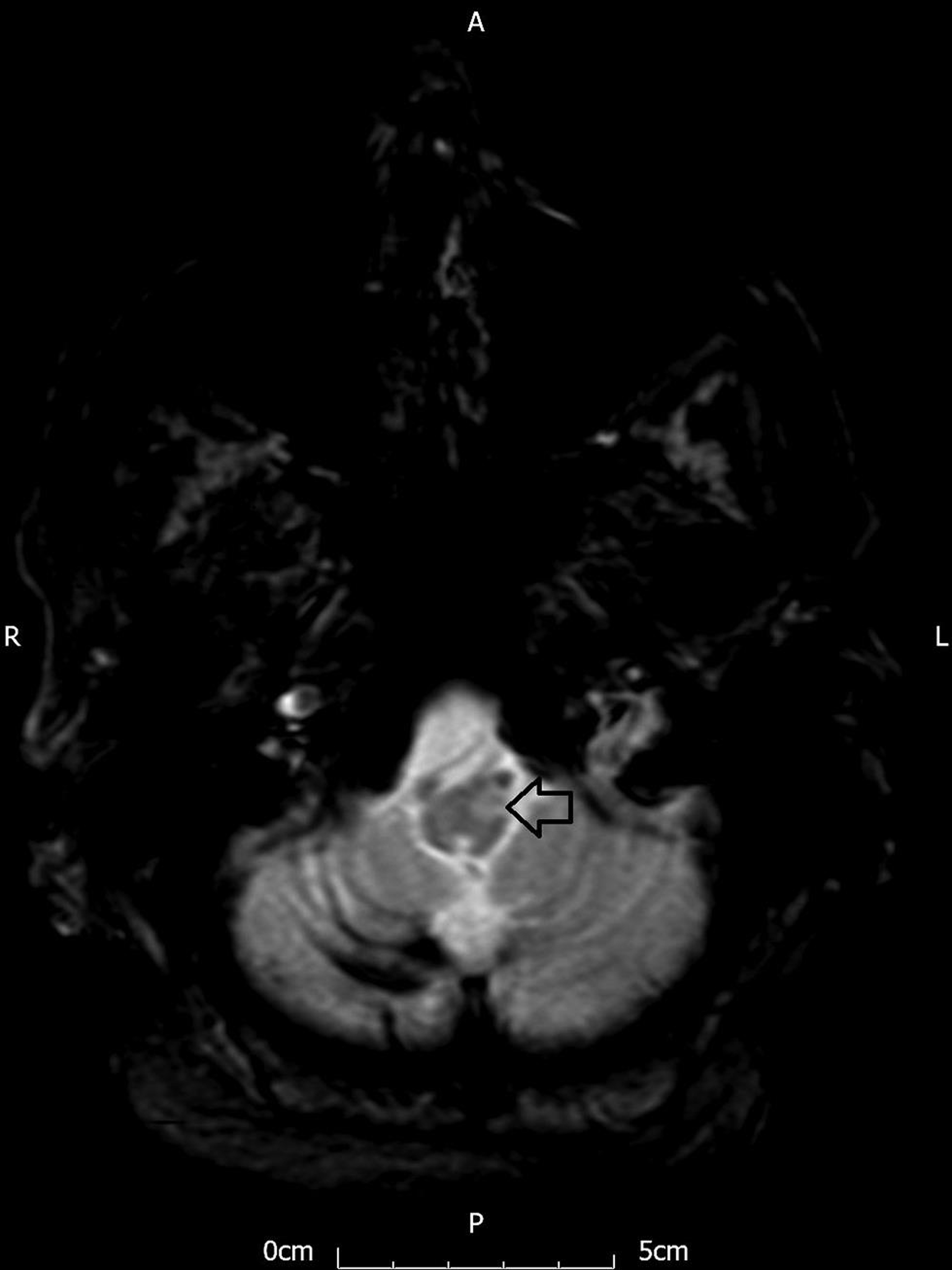
A 76-year-old gentleman presented with mild slurred speech. Five months earlier, he had vomiting and unsteady gait. Magnetic resonance imaging (MRI) head then showed hematoma of the dentate nucleus of the right cerebellum (Fig. 1, black arrow). Now the clinical examination revealed mild dysarthria, asymmetric palatal tremor predominantly involving the right palatal arch, and pharyngeal myoclonus (Video 1). The current MRI head showed hypertrophy of the contralateral inferior olivary nucleus of the medulla (Fig. 2, black arrow). He had symptomatic palatal tremor because of the contraction of the levator veli palatine muscle.1 We postulate that the pharyngeal myoclonus was due to the common vagal nerve supply. Hypertrophic olivary degeneration occurred secondary to a lesion in the Guillain–Mollaret triangle.2 The hallmark clinical feature of a lesion of the Guillain–Mollaret triangle is the palatal tremor. The unilateral palatal tremor happened due to the hypertrophic degeneration of the contralateral olivary nucleus.3 However, though bilateral symmetrical palatal tremor is common but an asymmetric bilateral tremor described in our patient was rarely reported in literature.
-
Fig. 1 Axial T2-weighted magnetic resonance imaging (MRI) sequence showing right cerebellar hemorrhage involving the dentate nucleus (black arrow) (dentate nucleus is a part of the Guillain–Mollaret triangle).
Fig. 1 Axial T2-weighted magnetic resonance imaging (MRI) sequence showing right cerebellar hemorrhage involving the dentate nucleus (black arrow) (dentate nucleus is a part of the Guillain–Mollaret triangle).
-
Fig. 2 Axial T1-weighted magnetic resonance imaging (MRI) sequence showing the hypertrophic olivary degeneration of the inferior olivary nucleus of the left hemimedullar (black arrow).
Fig. 2 Axial T1-weighted magnetic resonance imaging (MRI) sequence showing the hypertrophic olivary degeneration of the inferior olivary nucleus of the left hemimedullar (black arrow).
The palatal tremor can be essential or idiopathic and symptomatic. The essential palatal tremor occurs due to the contraction of the tensor veli palatine muscle, supplied by the trigeminal nerve.3 Often patients complain of an audible ear click. The MR head reveals no abnormalities in a patient with essential palatal tremor. Symptomatic palatal tremor occurs due to the contraction of the levator veli palatine, supplied by the vagus nerve. Many other clinical signs like Holme’s tremor, ocular tremor or flutter, or ataxia are found in patients with symptomatic palatal tremor.
Conflict of Interest
None declared.
Funding None.
References
- Symptomatic and essential palatal tremor. 2. Differences of palatal movements. Mov Disord. 1994;9(6):676-678.
- [Google Scholar]
- Hypertrophic olivary degeneration: the forgotten triangle of Guillain and Mollaret. Neurol India. 2009;57(4):507-509.
- [Google Scholar]
- Unilateral symptomatic palatal tremor due to pontocerebellar infarction. Ann Indian Acad Neurol. 2011;14(3):219-221.
- [Google Scholar]




