
Translate this page into:
A Patient with Schizencephaly and Agenesis of Corpus Callosum with No Neurological Deficits
Address for correspondence: Dr. Rosette Jabbour, St. George Hospital University Medical Center, Faculty of Medicine, University of Balamand, Achrafieh, Beirut, Lebanon. E-mail: rajabbour@stgeorgehospital.org
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 23-year-old male presented to the emergency room (ER) for polytrauma after involvement in a motor vehicle accident with head trauma but no loss of consciousness. He was previously healthy with no history of seizures or other neurological problems and had not been taking any medications. He is a senior mass communication student who lives with his parents and plays football weekly. The investigations in the ER revealed a right femur fracture and right frontal skin laceration necessitating suturing. A computed tomography scan of the brain revealed no acute intracranial bleed; however, partial agenesis of the corpus callosum was noted with possible accompanying schizencephaly of the left frontal lobe. These findings were further evaluated by a brain magnetic resonance imaging [Figure 1] which confirmed the presence of the partial agenesis of the anterior part of the corpus callosum, but the splenium visualized and noted to be thin. The anterior aspect of the left cingulate gyrus was abnormal with evidence of focal communication between the anterior horn of the lateral ventricle and the left aspect of the interhemispheric fissure. All findings were compatible with chronic left open lip schizencephaly (Type II). The patient underwent femur surgery and received standard postoperative care. Postsurgery, a neurological examination was also conducted that investigated patient's mental status, cranial nerves, motor function, muscle strength and tone, sensation, reflexes, and coordination which were all negative. Gait was not assessed because of femur fracture. The patient was subsequently discharged.
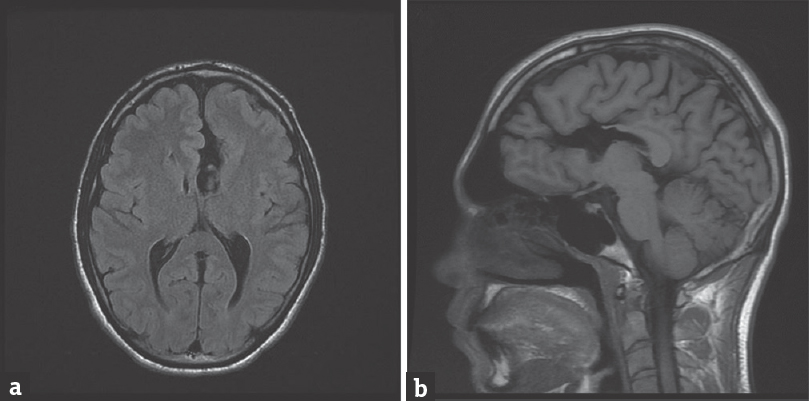
- (a) An axial T1-weighted image demonstrates left frontal lobe open-lip schizencephaly. (b) A sagittal T1-weighted image (to the left of the midline) demonstrates a cerebrospinal fluid-filled cleft. Agenesis of the anterior part of the corpus callosum is also noted
Schizencephaly is a rare disorder of cerebral cortical development with an incidence of 1.54/100,000.[1] It is caused by defective neuronal migration resulting in the formation of clefts that extend from the cerebral wall to the underlying ventricular surface. Types of schizencephaly include closed-lip clefts (Type I) and open-lip clefts (Type II). In addition, schizencephaly may occur as a unilateral or bilateral lesion.[12] Studies demonstrate multiple possible etiologies for schizencephaly ranging from intrauterine insults to possible genetic etiology.[12] This patient's prenatal history was negative for complications, maternal drug use or infection.
With regard to clinical presentation, patients could present with a variety of neurological and developmental defects. The correlation between imaging features and clinical outcome has been analyzed showing a correlation between the size of the cleft and motor deficits and mental retardation, but not seizures.[12] Although half of the patients present with epilepsy and especially those with unilateral lesions,[12] this patient had neither seizure activity nor a history of epilepsy.
A number of similar cases have been previously reported,[34] but all exhibit certain degrees of central nervous system manifestations such as cerebral palsy and epilepsy which are absent in this patient. This case demonstrates that it is possible for a patient to have schizencephaly along with partial agenesis of the corpus callosum and be without neurological deficits.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Schizencephaly: Clinical spectrum, epilepsy, and pathogenesis. J Child Neurol. 2005;20:313-8.
- [Google Scholar]
- Schizencephaly: Dramatic images in a normally functioning adult. PM R. 2015;7:901-2.
- [Google Scholar]
- Functional MRI of language-related activation in left frontal schizencephaly. J Comput Assist Tomogr. 2000;24:732-4.
- [Google Scholar]




