
Translate this page into:
A case of communicating rami between the median and musculocutaneous nerves passing through the substance of an accessory head of biceps brachii
Address for correspondence: Dr. Tripti Meriel Jacob, Department of Anatomy, Christian Medical College, Vellore - 632 002, Tamil Nadu, India. E-mail: triptimj@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
During routine dissection of a 60-year-old male cadaver in the Anatomy department, multiple neuro-muscular anomalies in the left arm were noted. The biceps brachii had an accessory head originating from the anteromedial surface of the middle of shaft of humerus. These muscle fibers inserted into the bicipital tendon from the medial aspect. The median nerve gave a variant high branch in the middle of the arm. The musculocutaneous nerve pierced the coracobrachialis, gave branches to the long and short heads and terminated in the accessory head of the biceps. Two communicating rami were seen between the terminal part of the musculocutaneous nerve and the high branch of the median nerve, located 18 and 19 cm from the corocoid process, respectively. These communications pierced the fibers of the accessory head [Figure 1]. The branch of the median nerve in the arm received the communicating branches from the musculocutaneous nerve, supplied the brachialis and continued as the lateral cutaneous nerve of the forearm [Figure 2].

- Dissection of the left arm. Note the median nerve (MN) giving an accessory branch (Ma) in the arm. The musculocutaneous nerve (McN) is seen piercing coracobrachialis (Cb) and giving a branch to supply the short (Bs) and long heads (Bl) of biceps brachii. It then ends in the accessory head of biceps brachii (Ba). Note the communicating rami (c) between the musculocutaneous nerve and the accessory branch of median nerve passing through the accessory head
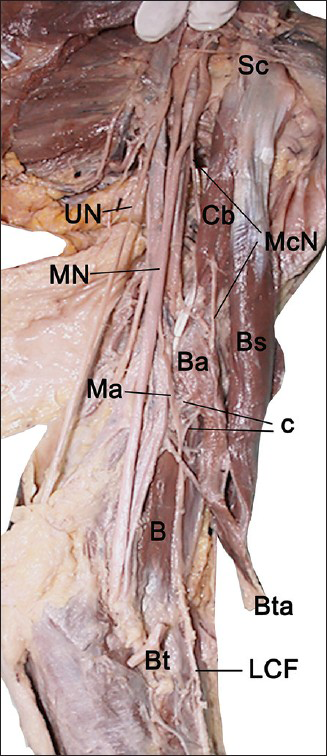
- View of dissected left axilla, arm and upper forearm. Notice how accessory branch (Ma) of the median nerve (MN) continues as the lateral cutaneous nerve of forearm (LCF) after supplying the brachialis (B). Sc-coracoid process of scapula; UN-ulnar nerve; McN-musculocutaneous nerve; c-communicating rami; Cb-coracobrachialis, Bs-short head of biceps brachii, Ba-accessory head of biceps brachii, Bta-biceps tendon and aponeurosis, Bt-cut end of tendon of biceps
Variations in the innervation of the flexors of the arm include absence of the musculocutaneous nerve wherein the flexors are supplied by the median nerve;[1] the musculocutaneous nerve supplying coracobrachialis and then joining the median nerve;[2] or communications between the two nerves without change in innervation of the flexors.[3] Differences in innervation are often associated with the presence of accessory head of biceps brachii.[4] One report described a proximal nerve supplying the coracobrachialis and the long and short heads of biceps brachii, while a distal branch from the median nerve supplied the third head of biceps brachii and brachialis, and continued as the lateral cutaneous nerve of the forearm.[5] This differs from the present case in the innervation of the third head of biceps brachii as well as the absence of communications between the two nerves. Knowledge of these variations is important while evaluating neurological deficits. High injuries to the median nerve could result in an unusual pattern of motor and sensory deficit including weaker flexion at the elbow and hyposthesia of the lateral aspect of the forearm. Similarly, injury to the musculocutaneous nerve may not present with the typically expected deficits. It is also important for surgeons to keep in mind the possibility of an aberrant high branch of median nerve while operating in the arm. The communicating branches, in this case, were found within the substance of the accessory head of biceps. This could potentially result in entrapment neuropathy.
In conclusion, for the first time, in a case of communication between the median and musculocutaneous nerves, we report the communications lying within the substance of the accessory head of biceps brachii. The median nerve gave a high branch in the arm and the distribution of the median nerve was variant, taking over part of the normal distribution of the musculocutaneous nerve. Knowledge of variations in innervation is important in clinical evaluation of peripheral nerve injuries as well as exploratory surgeries in the arm.
References
- Absence of musculocutaneous nerve along with accessory head of biceps brachii. Int J Recent Trends Sci Technol. 2011;1:45-48.
- [Google Scholar]
- Communication between median and musculocutaneous nerve. J Morphol Sci. 2011;28:246-9.
- [Google Scholar]
- Patterns of connections between the musculocutaneous and median nerves in the axilla and arm. Clin Anat. 2002;15:11-7.
- [Google Scholar]
- Supernumerary head of biceps brachii and branching pattern of the musculocutaneus nerve in Japanese. Surg Radiol Anat. 1992;14:175-85.
- [Google Scholar]
- Three-headed biceps brachii muscle associated with duplicated musculocutaneous nerve. Clin Anat. 2005;18:376-9.
- [Google Scholar]




