
Translate this page into:
Tuberculous meningoencephalitis with severe neurological sequel in an immigrant child
Address for correspondence: Dr. Kadriye Kart Yasar, Department of Clinical Microbiology and Infectious Diseases, Haseki Training and Research Hospital, Adnan Adivar Street, Aksaray 34300, Istanbul, Turkey. E-mail: kadriyeyasar@hasekihastanesi.gov.tr
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Central nervous system tuberculosis (TB) is the most devastating manifestation of TB. It is a challenge for clinicians because of the difficulty in making an early diagnosis and the severe consequences of delayed treatment. The aim of this report is to point out the relation between migration and TB based on a 14-year-old child with tuberculous meningoencephalitis (TBM) of an immigrant family. Migration, crowded living conditions and positive family history contribute to the severe course of TB as TBM and miliary TB forms. TB control may prevent these severe manifestations of the disease among immigrants. Prompt diagnosis with helpful early diagnostic tools like polymerase chain reaction in TBM is crucial due to the high mortality and morbidity.
Keywords
Immigrant
neurological sequel
PCR
tuberculosis
tuberculous meningoencephalitis

Introduction
Tuberculosis (TB) continues to be a major global health problem worldwide. The World Health Organization (WHO) reported 9.27 million new cases of TB and 1.3 million TB-related deaths among human immunodeficiency syndrome (HIV)-negative populations in 2007.[1] In addition, the migration is expected to contribute to the spread of the disease in both industrialized and resource-poor countries. The disease especially appears in younger objects and generally involves the lungs in the immigrant populations from high-prevalence countries.[2] Central nervous system TB is the most destructive form of TB and is associated with high mortality rates up to 60% and neurological sequel in 25% of the survivors despite the new neuroimaging techniques and effective antituberculous therapy.[3]
With this report, we aimed to create awareness about TB – especially its serious forms and complications – among clinicians who deal with immigrants.
Case Report
A 14-year-old child of an immigrant family, a native of Azerbaijan who had been living in Turkey for 10 years, presented to our clinic in September 2009 with complaints of fever, persistent headache and vomiting that lasted for 10 days. Physical examination was normal except for neck rigidity, meningeal irritation sign and mild confusion. The emergent cranial computerized tomography (CT) without contrast on admission scan showed no pathological findings. Thereby, lumbar puncture was performed to examine the cerebrospinal fluid (CSF). The findings were: CSF cell count, 57/mm3; leukocyte (60% lymphocyte), 18/ mm3; erythrocyte and glucose, 13 mg/dl (simultaneous blood glucose 109); protein, 243 mg/dl. The India ink stain was negative. Miliary pattern was suspected in the chest X-ray. Laboratory tests: WBC 12,300/mm3; hemoglobin 11.7 g/dl; CRP 12 mg/dl; anti-HIV antibody negative. On the same day, sudden loss of consciousness, bradycardia and hypotension developed and the patient was transferred to the intensive care unit (ICU). Ceftriaxone and acyclovir therapy was started due to clinical deterioration, loss of consciousness and seizure on the same day. A negative Herpes Simplex Virus (HSV) test result was obtained on the seventh day. Since the patient's mother had a pulmonary TB history and her clinical condition did not improve, antituberculous therapy with four drugs and dexamethasone was started on the second day. Then, the vital findings were found to have improved on the seventh day and she transferred to the infectious diseases ward. She was evaluated as stage III and cranial magnetic resonance imaging (MRI), which was performed on the seventh day with gadolinium, showed multiple tuberculoma in the basal ganglions, cerebral and cerebellar hemispheres, basal meningitis and minimal hydrocephalus [Figure 1]. Miliary pattern was detected in the thorax CT (HRCT) [Figure 2]. CSF polymerase chain reaction (PCR) for TB (GeneXpert MTB-RIF, Cepheid®, Sunnyvale, CA, USA) and Quantiferon TB gold test (Cellestis®, Australia) were positive on the third day. Mycobacterium tuberculosis was isolated from the CSF on the 21st day in Loewenstein Jensen (L-J) medium. During the hospitalization period, convulsion, hearing loss, aphasia and motor deficits developed and the patient was discharged from the hospital on the 34th day with neurological sequel (aphasia, motor deficits, mild mental defect and hearing loss). She has been followed-up in our outpatient clinic ever since.
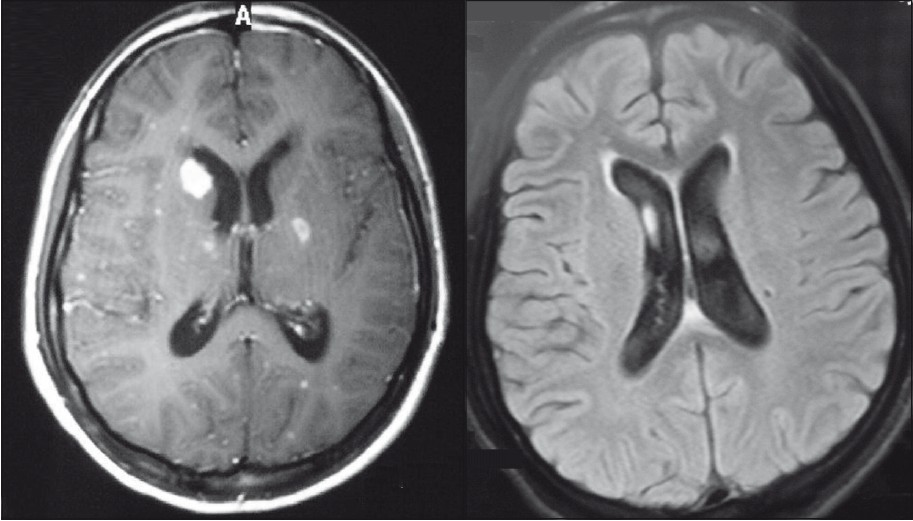
- a: Multiple tuberculomas and basal meningitis b: Hydocephalus in cranial imaging
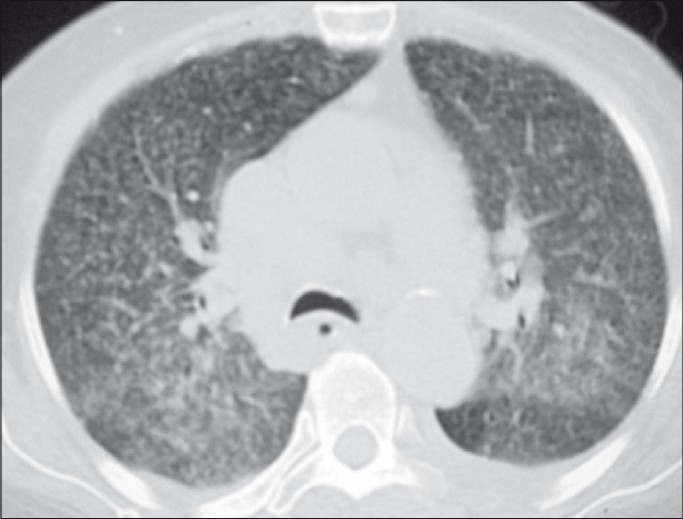
- Miliary pattern in high resolution computed tomography
Discussion
Tuberculous meningoencephalitis (TBM) is the most severe, life-threatening form of TB and usually carries a subacute or chronic form. Headache, vomiting, fever and neck rigidity are the most common complaints and findings.[3] Complaints of this case lasted for 10 days and, therefore, her disease was accepted as an acute/subacute form. On admission, there was no neurological deficit except confusion, but she was transferred to the ICU with comatose mental status on the second day. There were some factors known as predictors of poor outcome, including extreme ages, stage of illness and hydrocephalus[4–6] Hosoglu and colleagues[5] showed that drowsiness on admission is also an important predictor for neurological sequel. Confusion of the case on admission was considered as a clue for poor outcome according to this report, and neurological sequel developing in the subsequent days supported this knowledge.
The rate of TB history in the family or close contact with persons with active pulmonary TB is generally high in adult TBM patients in developing countries. In this case, family history was positive. Living in poor socioeconomic conditions and crowded areas results in a high rate of positive family histories. Positive family history, miliary TB, presence of hydrocephalus and multiple tuberculoma and younger age were predictive values for TBM. In addition to altered sensorium, these factors might be considered as poor prognostic factors in this case, which has clinical deterioration and neurological sequel.
A definitive diagnosis of TBM is made by isolating the organism from the CSF. But, isolation of the agent may not be possible by this time-consuming process in every patient. Antituberculous therapy (ATT) was started empirically on the second day in this case. However, Quantiferon and TB PCR were positive on the third day while culture positivity in L-J medium was obtained on the 21st day. Helpful diagnostic procedures like PCR or neuroradiological findings or presence of pulmonary TB may shorten this duration and provide early diagnostic advantages.[78] Basal meningitis and multiple tuberculoma were detected in cranial MRI in this case, whereas urgent cranial CT scan was normal. In addition, miliary pattern was shown in lung CT. Indeed, a recent study mentioned the more diagnostic and more predictive facilities of MRI for poor outcome in patients with TBM than CT.[6] Therefore, we suggest that clinicians should perform cranial MRI and chest X-ray to detect radiological clues for TB or other helpful laboratory tests like PCR and Quantiferon® as soon as possible to shorten the diagnosis period.
Tuberculomas are the most common forms of central nervous system TB and comprise 5–34% of all intracranial masses, which may be confused with other space-occupying lesions. They may be seen solitary, but multiple ones are more common.[9] In this case, multiple tuberculomas that were noncaseating, located both in cerebral and cerebellar regions and sized less than 2 cm were detected in cranial MRI.
Basal meningeal enhancement, hydrocephalus and basal ganglia infarctions consist of the common triad of neuroradiological findings.[10] Hydrocephalus was associated with neurological deterioration of this patient. Although early diagnostic procedures and follow-up CT were performed and steroid treatment was administered in the early stage, developing neurological sequel could not be prevented in this case. Thus, we suggested that there may be other poor prognostic factors such as immune system of the patient. The detailed evaluation on admission and early diagnosis may contribute to the prevention of severe complications and death arising from delayed therapy in TBM, but this attitude is not valid every time and in all patients.
TB is a global disease that travels in and between populations due to migration.[211] In conclusion, physicians should be aware of central nervous system TB besides the pulmonary forms of TB in immigrant populations. Severe neurological status on admission may result in permanent neurological sequels. Detailed evaluation of these patients on admission may prevent poor outcomes of TBM related with delayed diagnosis and therapy.
Source of Support: Nil
Conflict of Interest: None declared.
References
- World Health Organization. Global Tuberculosis Database. Available at: <http://www.who.int/research/en/>
- [Google Scholar]
- Transmission dynamics of pulmonary tuberculosis between autochthonous and immigrant sub-populations. BMC Infect Dis. 2009;9:197.
- [Google Scholar]
- Prognostic factors of neurological sequel in adult patients with ntuberculous meningitis. Neurosciences. 2010;15:262-7.
- [Google Scholar]
- Predictors of death in tuberculous meningitis: A multivariate analysis by 160 cases. Int J Tuberc Lung Dis. 2010;14:330-5.
- [Google Scholar]
- Predictors of outcome in patients with tuberculous meningitis. Int J Tuberc Lung Dis. 2002;6:64-70.
- [Google Scholar]
- MRI to demonstrate diagnostic features and complications of TBM not seen with CT. Childs Nerv Syst. 2009;25:941-7.
- [Google Scholar]
- British Infection Society guidelines for the diagnosis and treatment of tuberculosis of the central nervous system in adults and children. J Infect. 2009;59:167-87.
- [Google Scholar]
- Efficient diagnosis of tuberculous meningitis by detection of Mycobacterium tuberculosis DNA in cerebrospinal fluid filtrates using PCR. J Med Microbiol. 2009;58:616-24.
- [Google Scholar]
- Tuberculous meningitis: Many questions, too few answers. Lancet Neurol. 2005;4:160-70.
- [Google Scholar]
- Asylum seekers: Do we need new approaches to their health problems? Nobel Medicus 2010
- [Google Scholar]




