
Translate this page into:
The sociodemographic, clinical and pharmacotherapy characteristics influencing quality of life in patients with epilepsy: A cross-sectional study
Address for correspondence: G. Ranjana, Department of Pharmacology, St. John's Medical College and Hospital, Bangalore - 560 034, Karnataka, India. E-mail: ranjugurumurthy@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
Quality of life (QOL) assessment in patients with epilepsy (PWE) is increasingly recognized as an important component in the management of epilepsy.
Aims:
The objective of the present study was to assess influence of sociodemographic, clinical and pharmacotherapy characteristics collectively on QOL in adult PWE.
Settings and Design:
This was a cross-sectional, observational study in patients with confirmed diagnosis of epilepsy.
Materials and Methods:
QOL was assessed using modified QOLIE-10 questionnaire for epilepsy. Univariate and multiple regression analysis were done to determine factors associated with poor QOL, respectively.
Results:
There were 451 PWE, with a mean age 27.3 ± 8.15 years, 251 (56%) males and 191 (42%) had monthly income < 5000 Indian national rupees (INR)/month. The QOLIE score was 64.1 ± 15.97 (Mean ± SD). The univariate analysis showed factors such as lower monthly income, focal epilepsy, seizure frequency, antiepileptic drug (AED) polytherapy, conventional AEDs and frequent adverse drug reactions (ADRs) had significant negative influence on various domains of QOLIE-10 questionnaire. Multiple regression analysis showed seizure frequency as a significant predictor of most QOL domains and overall score, while ADRs as a significant predictor of all the domains. Seizure type was a predictive factor for domains like emotional well-being and overall score.
Conclusion:
Present findings showed patients on monotherapy had better QOL while those having lower monthly income, having focal epilepsy and who received conventional AEDs had negative influence on QOL scores. Further, higher seizure frequency and occurrence of ADRs were significant predictors of all the domains of QOL in PWE.
Keywords
Adverse drug reactions
antiepileptic drugs
epilepsy
monotherapy
polytherapy
quality of life

Introduction
Epilepsy is a major non-communicable disorder reported to affect nearly 50 million population worldwide.[1] It is estimated that there are 55,00,000 persons with epilepsy in India, 20,00,000 in USA and 3,00,000 in UK. Three to five percent of the population have a seizure sometime in their life and nearly one percent have “active epilepsy.”[2]
Antiepileptic drug (AED) monotherapy and their combinations are used for the treatment of various types of epilepsy. Treatment is aimed at controlling seizures with the lowest possible occurrence of AED adverse effects, thus allowing the person to become an active member in the community and at the lowest possible overall cost.[3]
Recently, the concept of quality of life (QOL) assessment has led to the development of generic and disease specific questionnaires to evaluate patient reported outcomes. Patients with epilepsy (PWE) are reported to have poor self-esteem and higher levels of anxiety, depression, problems with social interaction and involvement. Therefore, the goal in the management of epilepsy is not only cessation of seizures with minimal AED side effects but also an improved overall QOL.[4]
Several tools have been developed to estimate QOL in PWE in different settings such as drug trials, epilepsy surgery programs and for general purposes – QOLIE-31,[5] QOLIE-10,[6] or short form 36-SF36.[7]
There have been few studies reported in Indian literature examining the influence of selected factors independently on QOL. The present study was therefore designed to collectively address the influence of sociodemographic, clinical and pharmacotherapy characteristics on QOL in PWE.
Materials and Methods
This cross-sectional study was conducted by the Division of Clinical Pharmacology at the out-patient and inpatient Department of Neurology, St John's Medical College and Hospital, Bangalore, over a period of one and half years from January 2012 to July 2013. Patients receiving AED treatment ≥ 18 years of age who have consented to participate were enrolled. Pregnant/lactating women and those with co-morbidities which might be a confounding factor in QOL assessment in PWE were excluded from the study. Ethical clearance was obtained from Institutional Ethical Review Board. Data was collected using a specially designed case record form [CRF] which included detailed demographic/family history, AEDs prescribed and degree of seizure control including adverse drug reactions (ADRs). Patients were classified according to age, gender, and monthly income. The epilepsy diagnosis was based on electrophysiological (EEG) and neuroimaging (CT and MRI) by a qualified neurologist with experience in the field of epilepsy. Details of AED treatment included generic name, dose, duration and ADR profile.
QOL was assessed using responses to modified QOLIE-10 questionnaire for epilepsy derived from the QOLIE-31 which comprises seven domains, namely seizure worry, emotional well-being, energy/fatigue, cognitive function, overall QOL, medication effects (physical and mental state), and social function (work, driving, social functions). Responses were averaged out to provide total scores.
Data was analyzed using descriptive statistical analysis and was expressed as Mean (±SD) and percentages. In univariate analysis categorical variables were compared using Chi-square test and continuous variables using Student's t-test and ANOVA.
Monthly income within group differences regarding QOLIE score were assessed by means of ANOVA with post hoc Bonferroni test.
The significant variables in univariate analysis were entered into stepwise multiple regression model to identify the significant predictors of poor QOL for each domain of QOLIE-10. The independent variables were monthly income, type of epilepsy (focal/generalized) seizure frequency, type of AED therapy (mono/poly), type of AEDs (conventional/new/combined), ADRs (Yes/No) and dependent variables were domain scores analyzed using SPSS for windows version 16 software. Statistical significance was set at P < 0.05.
RESULTS
Sociodemographic and clinical characteristics [Table 1]
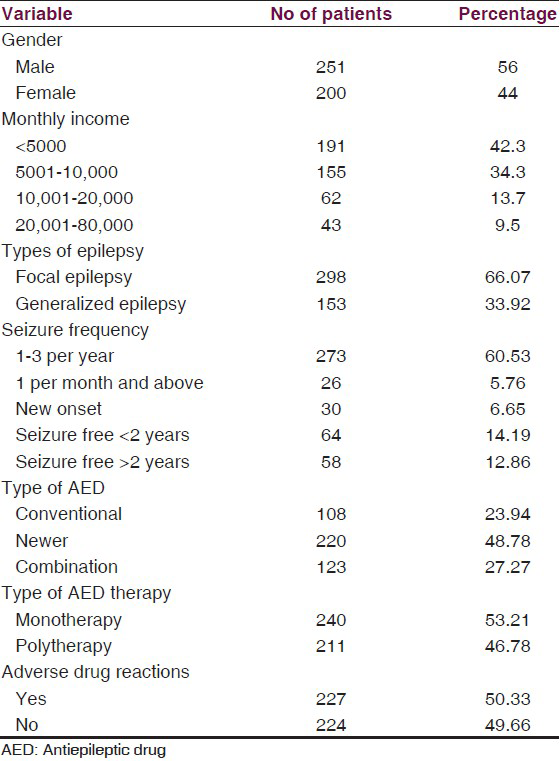
The present cross-sectional study involved 251/451 (56%) male patients and majority (53.8%) in the age group of 21-30 years.
Mean duration of epilepsy was 7.5 ± 4 years. Two-hundred ninety eight (66%) patients had focal epilepsy and 153 (33.9%) generalized epilepsy. Seizure frequency was 1-3 per year in 273 (60.4%) patients and 122 (27%) were seizure free for more than 12 months.
The pattern of use of AEDs showed 108 (23.9%) patients who received conventional AEDs and 220 (48.7%) newer AEDs and the remaining 123 (27.2%) combination AED therapy. AED monotherapy was received by 240 (53.2%) PWE, 160 (35.4%) received two drug combination, 47 (10.4%) triple therapy and 4 (5.1%) >3 AEDs.
The most frequently prescribed conventional AED monotherapy was phenytoin (PHT) 34/240 [14.1%], followed by carbamazepine (CBZ) 25/240 (10.41%). The pattern of use of newer AEDs included oxcarbazepine (OXCBZ) in 70/240 (29.1%) followed by levetiracetam (LEV) 49/240 (20.4%) and topiramate (TPM) in 6 (2.5%).
For the treatment of focal epilepsy PHT, CBZ, OXCBZ and LEV were used and for the treatment of generalized epilepsy valproic acid (VPA), OXCBZ, LEV and lamotrigine (LMT) were used.
Most common AED dual therapy was OXCB with clobazam (CLB) 31/211 [14.6%] and most frequently used AED as add-on was clobazam (58.2%).
ADRs involving central nervous system (39.9%) were impaired memory, tiredness, drowsiness, headache and depression. Other adverse effects included aphthous ulcer (3.3%), weight gain (2.2%), gastritis (1.5%), bone pain (1.3%), rashes (1.1%). and pimples (0.8%).
QOLIE - 10 scores and its correlation with sociodemographic and clinical characteristics
The overall QOLIE-10 score ranged from 15.97 to 100 with a Mean ± SD 64.1 ± 15.97. QOLIE score > 50 was considered as optimal and >70 considered as better QOL.
The mean QOLIE-10 score was significantly lower in patients with monthly income < 5000 INR in emotional (P = 0.003) overall (P = <0.01) and social (P = 0.002) domains, as well as for the total score (P = 0.002) [Table 2].
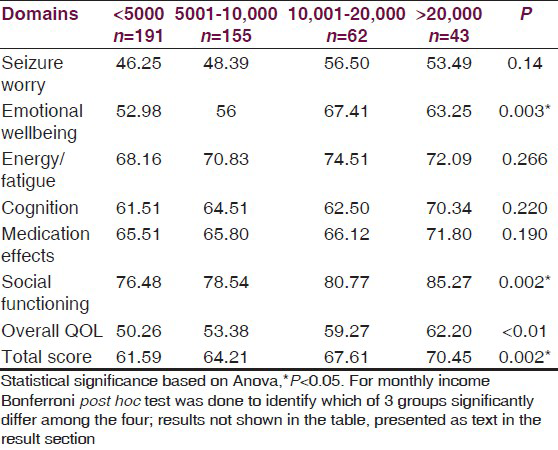
The post hoc test showed that emotional well-being domain score was significantly low in patients with monthly income of <5000 INR compared to 10,001-20,000 INR (P = 0.004) and 5001-10,000 INR compared to 10,001-20,000 INR.
Social function domain score was significantly low in patients with monthly income of < 5000 INR compared to >20,000 INR (P = 0.01).
Overall score was significantly low in patients with monthly income > 5000 compared to10,001-20,000 INR (P = 0.04), <5000 INR compared to 20,000 INR (P = 0.001) and 5001-10,000 INR compared to 20,000 INR (P = 0.02).
Total score was significantly low in patients with monthly income of > 5000 INR compared to 10,001-20,000 INR (P = 0.056) and <5000 INR compared to <20,000 INR (P = 0.006).
No significant relationship was observed between QOLIE-10 scores with other demographic characteristics.
In relation to type of epilepsy, patients with focal epilepsy exhibited significantly lower scores for emotional well being (P = 0.007), medication effects (0.001), overall QOL (P = 0.01) domains and total scores (P = 0.002) when compared to patients with generalized epilepsy [Table 3].
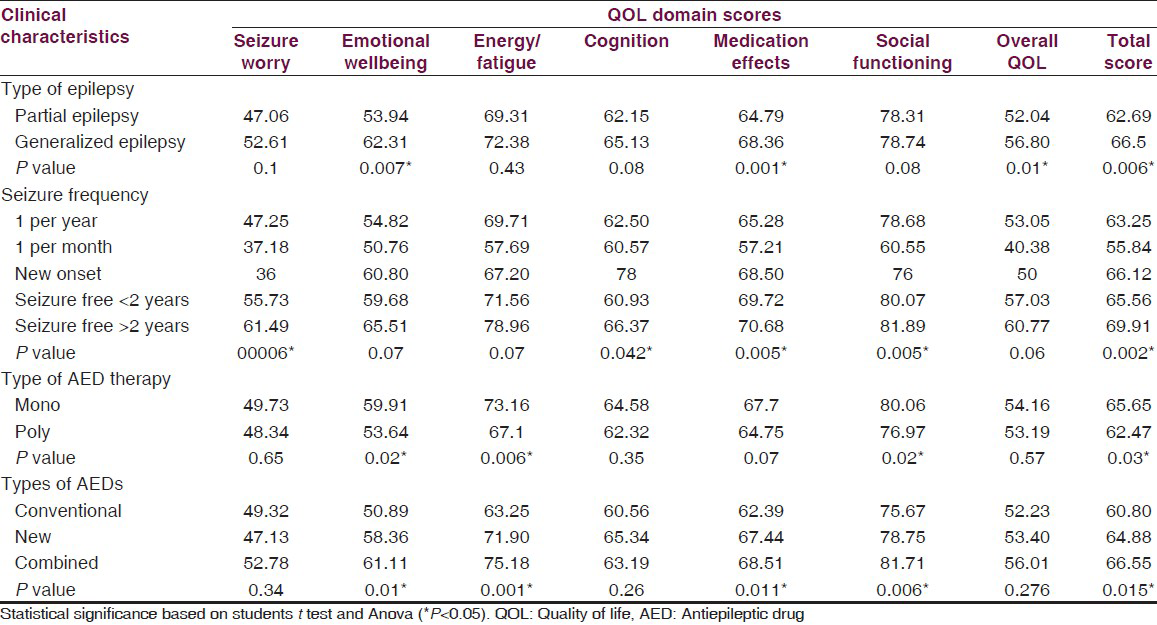
There were differences in QOL scores between the groups [Table 3] with respect to frequency of seizures for domains—seizure worry (P = 0.04), medication effects (P = 0.005) and social functioning (P = 0.005) with lower scores for the groups having 1 seizure per month in relation to other groups.
The patients on AED mono-therapy had significantly higher QOLIE-10 scores, when compared to those on polytherapy, in the domains of emotional well being (59 vs. 53.6, P = 0.02), energy/fatigue (73.1 vs. 67.1, P = 0.006), social functioning (80.0 vs. 76.9, P = 0.02) and total score (65.6 vs. 62.4, P = 0.03) [Table 3].
With regards to patients receiving conventional AEDs the scores for emotional (P = 0.01), energy (P = 0.0001), medication (P = 0.01) domains and total score (P = 0.015) were significantly lower compared to those receiving newer and combination AEDs (New + Old AEDs) [Table 3].
On analysis type of individual AEDs used to treat different types of epilepsy did not have any significant association with QOLIE score.
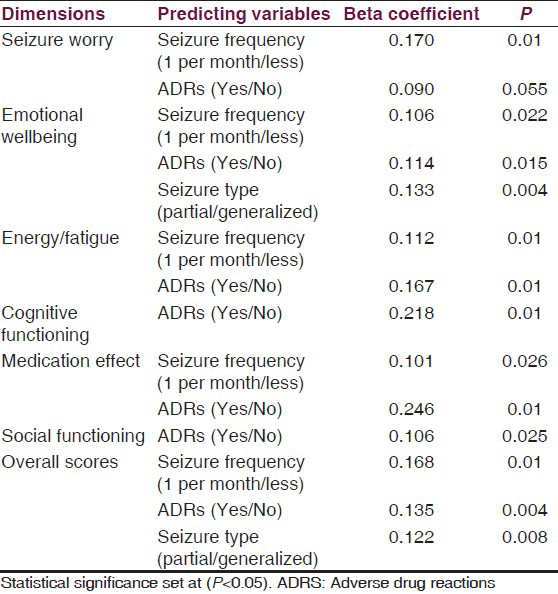
Multiple regression analysis showed that the seizure frequency was a significant predictor of poor QOL for domains like seizure worry, emotional wellbeing, energy/fatigue, medication effects, and overall score. Seizure type was a significant predictor of poor QOL for domains like emotional wellbeing and overall score. Occurrence of ADRs was found to be a significant predictor for all the domains [Table 4].
Discussion
A careful consideration of the frequency, type of seizures, appropriate selection of AEDs with minimal side effects are important and relevant for the optimal management of epilepsy. More recently for clinical assessment, evaluation of QOL is considered as an important parameter that can contribute to better understanding of the problems faced by PWE, including those with uncontrolled epilepsy.[8] Hence, in the present study we assessed the influence of demographic, clinical and pharmacotherapy characteristics collectively on QOL in adult PWE.
The assessment of QOL using QOLIE-10 showed mean QOLIE score of 64.1 ± 15.97 which is similar to that reported by Rakesh et al.[9] with the highest mean total score for social functioning [78 ± 25.14] domain and lowest for seizure worry domain [47 ± 32.1]. However, the mean total score in our study was higher than the study conducted in Australia[10] (52.9 ± 23.1), which may be due to the fact that respondents of their study were of the older age group. Also, the social function domain score was highest while energy/fatigue scores were the lowest. Difference in study methods using different questionnaires to assess QOL along with variation in inclusion and exclusion criteria may account in addition to the age for observed differences.
The influence of low monthly income among PWE, was found to be significantly associated with poor QOL, in contrast to patients with higher monthly income who showed better QOL a finding similar to the study done by Nagarathnam et al.[11] In another study done by Daniel et al.[12] patients with higher annual income showed better QOL.
No significant relationship was observed in the present study between QOLIE-10 scores with other demographic characteristics, a finding similar to the study done by Tracy et al.[13]
In our study the patients with focal epilepsy were found to have significantly lower QOL scores in contrast to observations by Herodes et al.[14] who reported lower scores in patients with GTCS. However, Thomas et al.[15] using QOLIE-31 on Indian and Guekht et al.[16] in Russian patients have found that localization-related epilepsy patients had lower QOL scores than those with generalized seizures which is similar to our findings. While, a study done by Mohamadi et al.[17] showed that type of seizure do not correlate significantly with QOL and these authors have instead attributed the observed difference to the seizure frequency, duration of seizure and its severity in their study groups.
Duration of epilepsy did not show statistically significant impact on QOL scores in our study, similar to the findings of a study done by Norsa’adah et al.[18] which also found no significant association between duration of epilepsy and QOL, although they noted lower scores of QOL in those who had longer duration of illness. As opposed to our study, Dijbuti et al.[19] have found that longer duration of disease has a significant positive impact on QOLIE scores as well as seizure worry and social functioning.
The negative influence of AED polytherapy on social interaction, energy level, and emotional disturbance is in agreement with another study in India by Thomas et al. which showed positive association between polytherapy and poor QOL.[15]
Haroon[20] et al. have shown that the energy level, fear of future seizure and parameters indicating general wellbeing of a person were comparable between PWE who received both older and newer drugs. However, in contrast, findings of our study showed patients on conventional drugs had lower scores in the domains such as emotional wellbeing, energy and medication effects. Since both studies are reported from India, it is difficult to explain what contributed to this differential observation therefore further studies are warranted. It has been proposed that newer AEDs are considered superior to conventional AEDs due to their improved pharmacokinetic profile with convenient dosage administration schedule as well as acceptable tolerability. Therefore, findings of our study where newer AEDs showed positive influence on QOL may be considered to add further evidence to this proposal. Studies in the past have evaluated impact of newer drug lamotrigine on QOL in PWE using various tools such as SF-36, QOLA, QOLIE-89 and QOLIE-31 in variety of clinical settings and have consistently demonstrated an improvement in QOL.[21] Similarly, studies with levetiracetam as add-on therapy have suggested an improvement in QOL.[22] However, the effect of individual AEDs on analysis did not have any statistically significant association with QOLIE score results similar to the study done by Mehtha et al.[23]
Our results with regards to the clinical characteristics such as seizure frequency which exerted markedly negative influence on the QOL and the same was identified as a significant predictor for domains such as seizure worry, emotional well being, energy/fatigue, medication effects and overall score. These observations are similar to the reports from Guekht et al.[16] who concluded that high seizure frequency was clearly responsible for limited daily activity leading to impairment of social function, physical activity, and in addition caused psychological problems in their study. Further Vickery et al.[24] have also reported sustained improvement in QOL following long-term absolute freedom from convulsive episodes in patients with refractory epilepsy. Sinha et al.[25] in a study done at Kolkata India also found poor QOL to be associated with higher seizure frequency.
AEDs are often prescribed on a long-term basis and hence have a higher potential to produce ADRs. Studies in the past have reported on ADR profile with use of AEDs. In a study done by Roopa et al.[26] at the same center showed more numbers of ADRs following polytherapy with no significant difference in frequency and severity of ADRs between conventional verses newer AEDs. However, there are not many studies which have explored influence of ADRs on QOL. ADRs were found to be significant predictor of all the domains of QOLIE-10, a finding similar to the study done by Luoni et al.[27] where among many variables that were investigated, adverse effects and depressive symptoms were identified as the most important determinants of health related QOL and the strongest predictors of scores in each of the seven QOLIE-31 subscales in PWE.
Conclusion
Our study population with low monthly income, suffering from focal epilepsy, having greater seizure frequency, who received conventional AEDs and reported ADRs had poor QOL, while PWE on AED monotherapy had better QOL. Greater seizure frequency and ADRs were the main predictors influencing the QOL in PWE. Although, the number of patients was adequate, the limitation of our study was cross sectional design and exclusion of psychiatric co morbidity which can be the important predictor of QOL in PWE. Therefore, further studies involving long-term follow up would be appropriate to identify factors that would contribute to improved QOL and hence effective management of PWE.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- The Treatment of epilepsy in developing countries: Where do we go from here? Bull World Health Organ. 2001;79:344-51.
- [Google Scholar]
- Antiepileptic drug utilization and seizure outcome among paediatric patients in a Malaysian public hospital. Singapore Med J. 2010;51:21-7.
- [Google Scholar]
- Cost effective analysis of dual therapy in epilepsy, a study from India. Neurol Asia. 2011;16:309-14.
- [Google Scholar]
- Development and cross-cultural translations of a 31-item quality of life in epilepsy inventory. Epilepsia. 1998;39:81-8.
- [Google Scholar]
- A brief questionnaire to screen for quality of life in epilepsy: The QOLIE-10. Epilepsia. 1996;37:577-82.
- [Google Scholar]
- The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-83.
- [Google Scholar]
- Quality of life among people with epilepsy: A cross-sectional study from rural southern India. Natl Med J India. 2012;25:261-4.
- [Google Scholar]
- Stigma, seizure frequency and quality of life: The impact of epilepsy in late adulthood. Seizure. 2008;17:281-7.
- [Google Scholar]
- Assesment of quality of life in epilepsy in Andra Pradesh. Neurol Asia. 2014;19:249-55.
- [Google Scholar]
- Quality of life among patients living with epilepsy attending the neurology clinic at Kenyatta National Hospital, Nairobi, Kenya: A comparative study. Health Qual Life Outcomes. 2013;11:98.
- [Google Scholar]
- The association of mood with quality of life ratings in epilepsy. Neurology. 2007;68:1101-7.
- [Google Scholar]
- Frequent seizures and polytherapy can impair quality of life in persons with epilepsy. Neurol India. 2005;53:46-50.
- [Google Scholar]
- Factors influencing on quality of life in people with epilepsy. Seizure. 2007;16:128-33.
- [Google Scholar]
- Psychometric evaluation of the Persian version of the quality of life in epilepsy inventory-31. Iran J Neurol. 2013;12:144-8.
- [Google Scholar]
- The quality of life of people with epilepsy at a tertiary referral centre in Malaysia. Health Qual Life Outcomes. 2013;11:143.
- [Google Scholar]
- Influence of clinical, demographic, and socioeconomic variables on quality of life in patients with epilepsy: Findings from Georgian study. J Neurol Neurosurg Psychiatry. 2003;74:570-3.
- [Google Scholar]
- Antiepileptic drugs prescription utilization behaviour and direct costs of treatment in a national hospital of India. Ann Indian Acad Neurol. 2012;15:289-93.
- [Google Scholar]
- A systematic review of the effects of lamotrigine on cognitive function and quality of life. Epilepsy Behav. 2001;2:85-91.
- [Google Scholar]
- Effect of levetiracetam on cognitive functions and quality of life: A one-year follow-up study. Epileptic Disord. 2008;10:297-305.
- [Google Scholar]
- Study of inter-relationship of depression, seizure frequency and quality of life of people with epilepsy in India. Mental Illness. 2014;6:5169.
- [Google Scholar]
- Relationship between seizure severity and health-related quality of life in refractory localization-related epilepsy. Epilepsia. 2000;41:760-4.
- [Google Scholar]
- Factors associated with quality of life of patients with epilepsy attending a tertiary care hospital in Kolkata, India. Neurol Asia. 2011;16:33-7.
- [Google Scholar]
- Patterns of adverse drug reactions to anti-epileptic drugs: A cross-sectional one-year survey at a tertiary care hospital. Pharmacoepidemiol Drug Saf. 2008;17:807-12.
- [Google Scholar]
- Determinants of health-related quality of life in pharmacoresistant epilepsy: Results from a large multicenter study of consecutively enrolled patients using validated quantitative assessments. Epilepsia. 2011;52:2181-91.
- [Google Scholar]




