
Translate this page into:
Telescoping Dual Covered Stent Graft Construct for Endovascular Treatment of a Giant Extracranial Carotid Artery Pseudoaneurysm
Address for correspondence: Dr. Dale Ding, Department of Neurosurgery, University of Virginia, P. O. Box: 800212, Charlottesville, VA 22908, USA. E-mail: dmd7q@hscmail.mcc.virginia.edu
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Large pseudoaneurysms which compress the parent vessel are challenging lesions to successfully treat with endovascular therapy. We describe the endovascular treatment of a giant extracranial carotid artery (ECCA) pseudoaneurysm resulting in substantial mass effect on the common carotid artery (CCA) bifurcation using a telescoping dual covered stent graft construct. A 56-year-old male was diagnosed with an 8.5 cm × 13 cm pseudoaneurysm arising from the left CCA bifurcation, which was causing luminal narrowing of the CCA and proximal internal carotid artery (ICA). The patient underwent endovascular intervention, during which a balloon-expandable covered stent was deployed within a heparin-bonded covered stent, such that the overall construct spanned from the CCA to the lower cervical ICA. The employment of a telescoping dual covered stent technique can successfully treat appropriately selected patients with large or giant ECCA pseudoaneurysms, with the concomitant goals of excluding the pseudoaneurysm and restoring the luminal caliber of the parent artery.
Keywords
Carotid artery
covered stent graft
endovascular procedures
pseudoaneurysm
stents

INTRODUCTION
Pseudoaneurysms of the extracranial carotid artery (ECCA) are uncommon, and many of these vascular lesions can be managed with medical therapy alone.[1] However, large or symptomatic ECCA pseudoaneurysms require intervention. Although ECCA lesions have traditionally been treated with surgery, the evolution and dissemination of endovascular techniques and technologies have shifted the management of ECCA pseudoaneurysms toward minimally invasive approaches.[2] Giant pseudoaneurysms resulting in compression and luminal narrowing of the parent vessel are difficult to treat with endovascular intervention since mass effect from the pseudoaneurysm can cause in-stent stenosis. The aim of this case report is to describe the use of a telescoping dual covered stent graft construct for the endovascular treatment of a giant ECCA pseudoaneurysm which was imposing a significant local mass effect on the common carotid artery (CCA) bifurcation.
CASE REPORT
A 56-year-old male presented with an enlarging left-sided neck mass over a period of 2 months. On initial examination, the patient had left cranial nerve X and XII palsies, as well as local oropharyngeal medialization and edema, which resulted in rightward displacement of the glottis and airway compromise. Neck computed tomography (CT) showed a very large left-sided neck mass extending from the level of the C2 transverse process superiorly to the supraclavicular fossa inferiorly, and measuring 8.5 and 13 cm in maximum transverse and craniocaudal dimensions, respectively [Figure 1a-c]. The mass resulted in considerable displacements of the larynx toward the right side, with mild airway narrowing.

- Neck computed tomography, (a) axial, (b) coronal, and (c) sagittal views, shows an 8.5 cm × 13 cm mass filling the majority of the left side of the neck. After a failed surgical biopsy of the mass resulted in significant intraoperative bleeding, neck computed tomography angiography, (d) axial, (e) coronal, and (f) sagittal views, shows an enlarging mass arising from the left common carotid artery bifurcation with a central, uniformly enhancing component measuring 5.2 cm × 5 cm × 5 cm, consistent with a partially thrombosed, giant extracranial carotid artery pseudoaneurysm
The initial diagnosis was suspected to be a necrotic, metastatic squamous cell cancer. The patient underwent an open biopsy, which revealed a large amount of organized hematoma. On further dissection, a large quantity of active hemorrhage was encountered, and therefore, establishing the diagnosis of a pseudoaneurysm. The intraoperative bleeding was controlled with pressure, the wound was closed, and the patient was transported to radiology, where neck CT angiography (CTA) demonstrated a giant, partially thrombosed ECCA pseudoaneurysm arising from the left CCA bifurcation [Figure 1d-f]. Mass effect from the pseudoaneurysm resulted in narrowing of the CCA just proximal to the carotid bulb as well as stenosis of the proximal internal carotid artery (ICA). After reviewing the findings of the neck CTA, the patient was transferred urgently to the neurointerventional suite for endovascular treatment.
Arterial access was established with a 7-French right femoral Cook Shuttle sheath (Cook Medical, Bloomington, Indiana, USA). Angiography showed a giant ECCA pseudoaneurysm, with a neck spanning the distal CCA, external carotid artery (ECA), and carotid sinus [Figure 2a and b]. A Headway 21 microcatheter (MicroVention, Tustin, California, USA) was navigated over a Synchro-14 microguidewire (Stryker Neurovascular, Fremont, California, USA) across the neck of the pseudoaneurysm into the left ICA. A Rosen exchange guidewire (Cook Medical) was then positioned high in the left ICA. A 7 mm × 50 mm Viabahn Endoprosthesis heparin-bonded covered stent graft (W. L. Gore and Associates, Flagstaff, Arizona, USA) was deployed from the lower cervical ICA to the distal CCA. Next, an 8 mm × 38 mm Atrium Advanta V12 balloon-expandable covered stent graft (Maquet, Rastatt, Germany) was deployed, within the first covered stent, from the carotid sinus to the CCA. The telescoping dual covered stent graft construct was then angioplastied along its length.
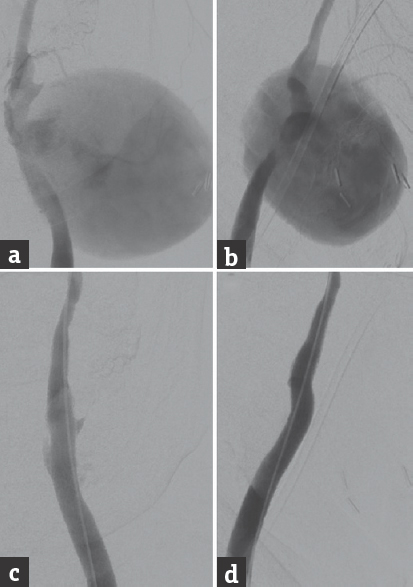
- Cerebral angiography, (a) anteroposterior and (b) lateral views of a left common carotid artery injection, shows a giant extracranial carotid artery pseudoaneurysm, with a neck spanning the distal common carotid artery, external carotid artery, and carotid sinus. Mass effect from the pseudoaneurysm is resulting in compression and luminal narrowing of the proximal internal carotid artery. The extracranial carotid artery pseudoaneurysm was treated with an 8 mm × 38 mm Atrium Advanta V12 covered stent telescoped within a 7 mm × 50 mm Viabahn Endoprosthesis covered stent. Poststenting control angiography, (c) anteroposterior and (d) lateral views of a left common carotid artery injection, shows occlusion of the pseudoaneurysm and improved caliber of the internal carotid artery
Final control angiography demonstrated obliteration of the pseudoaneurysm and improved caliber of the previously stenotic proximal ICA, without any evidence of intracranial complications [Figure 2c and d]. The patient was prescribed dual antiplatelet therapy (aspirin 100 mg and clopidogrel 75 mg daily) for 6 weeks postoperatively, followed by monotherapy with aspirin indefinitely. Carotid Doppler ultrasonography on postoperative day 2 showed patency of the dual stent graft construct spanning the left distal CCA and proximal ICA as well as occlusion of the pseudoaneurysm. Due to the patient's multiple medical comorbidities, he remained hospitalized for a month after the stenting procedure but was eventually discharged home without postoperative neurological complications.
DISCUSSION
Pseudoaneurysms are the most common aneurysmal lesions of the ECCA.[1] The goal of endovascular therapy for ECCA pseudoaneurysms is occlusion of the pseudoaneurysm while preserving flow through the affect portions of the CCA and ICA.[3] Although unilateral ECA occlusion is universally well tolerated due to extensive collateral supply, ICA occlusion can result in devastating thromboembolic and ischemic cerebral infarctions. Therefore, reconstructive approaches (i.e., stenting) are generally preferred over destructive approaches (e.g., ICA occlusion or ligation). In a cohort of 116 ECCA pseudoaneurysms, Fankhauser et al. reported that the mean diameter of symptomatic pseudoaneurysms was 1.7 cm.[1] The pseudoaneurysm in our case was substantially larger, with a maximum diameter of 13 cm. These giant lesions present unique challenges to both surgical and endovascular treatment, particularly when mass effect from the pseudoaneurysm is compressing the parent artery.
The use of covered stents has been previously reported for the treatment of ECCA pseudoaneurysms.[4] However, due to the size and extensive mass effect from pseudoaneurysm in our patient, we did not believe a single stent would provide sufficient radial force to maintain the patency of the compressed ICA. Therefore, we used a telescoping dual covered stent graft construct, in which a balloon-mounted covered stent was deployed within another heparin-bonded covered stent, to simultaneously achieve twin goals: (1) Exclusion of the ECCA pseudoaneurysm and (2) luminal restoration of the ICA.
CONCLUSIONS
A technique utilizing telescoping covered stents can be employed for the endovascular treatment of appropriately selected patients with large or giant ECCA pseudoaneurysms. However, further studies assessing the long-term patency of telescoping dual covered stent constructs are necessary.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Surgical and medical management of extracranial carotid artery aneurysms. J Vasc Surg. 2015;61:389-93.
- [Google Scholar]
- Endovascular treatment of carotid and vertebral pseudoaneurysms with covered stents. AJNR Am J Neuroradiol. 2008;29:983-7.
- [Google Scholar]
- Single-center experience on endovascular repair of noninfected extracranial internal carotid artery pseudoaneurysms. Ann Vasc Surg. 2013;27:672.e13-7.
- [Google Scholar]
- Use of covered stent grafts in the extracranial carotid artery: Report of three patients with follow-up between 8 and 42 months. AJNR Am J Neuroradiol. 2004;25:1760-3.
- [Google Scholar]




