
Translate this page into:
Syringomyelia secondary to cervical spondylosis: Case report and review of literature
Address for correspondence: Dr. Nupur Pruthi, Department of Neurosurgery, National Institute of Mental Health and Neurosciences, Bangalore, Karnataka, India. E-mail: pruthi_nupur@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Syringomyelia secondary to cervical spondylosis is a rare entity to encounter in clinical practice. We discuss the case of a 53-year-old lady who presented with a syringomyelic syndrome and was found to have cervical spondylosis on imaging. Cine-MRI revealed an obstruction of cerebrospinal fluid (CSF) flow in the cervical spinal subarachnoid space. Decompression of the same led to clinical and radiological improvement. There is a potential causal association between cervical spondylosis and syringomyelia. MRI CSF flow studies may help in deciding the course of treatment in such cases. A subset of patients with cervical spondylosis and concurrent spinal cord signal intensity changes may show reversal of the same following intervention.
Keywords
Cervical spondylosis
cine-magnetic resonance imaging
laminectomy
syringomyelia

Introduction
Syringomyelia has commonly been associated with the Chiari 1 malformation and is believed to be due to disequilibrium between the cranial and spinal subarachnoid spaces secondary to tonsilar impaction at the foramen magnum.[1] This condition may also occur secondary to cervical spinal cord trauma, tubercular arachnoiditis and as an idiopathic entity. Cervical spondylosis is classically seen as a disease which causes extradural spinal cord compression. We present a case in which a patient with cervical spondylosis presented with a near holocord syringomyelia.
Case Report
A 53-year-old housewife presented with history of weakness and wasting of the right forearm and hand since 1 year. She also complained of significant almost disabling parasthesias in all four limbs involving both hands and feet since 6 months. In addition, she noted impaired pain and temperature sensation in the right upper limb. Spinal examination was normal. Neurologically, she had weakness and wasting of the small muscles of the right hand, with normal tone. Deep tendon reflexes were diminished in both upper limbs and normal in the lower limbs. Plantar reflexes were bilaterally flexor. She had sensory loss to pain and temperature in bilateral C5 and C6 dermatomes.
Imaging
The patient was evaluated with an MRI of the craniovertebral junction and the whole spine, which revealed spondylotic changes in the cervical spine predominantly from C4-C6. A holocord syrinx, hypointense on T1 and hyperintense on T2 was seen. There was no evidence of tonsilar descent and the cistern magna was well seen [Figure 1aߝd].

- MRI of the cervical spine and CVJ showing a syrinx on T1 (a) and T2 (b) images. Normal position of the tonsils (c) and a holocord syrinx (d)
Cine MRI was performed to document CSF flow which showed obstruction of CSF flow in the spinal subarachnoid space opposite C4-C6 and free flow of CSF both anterior and posterior to the spinal cord at the foramen magnum [Figure 2a and b].
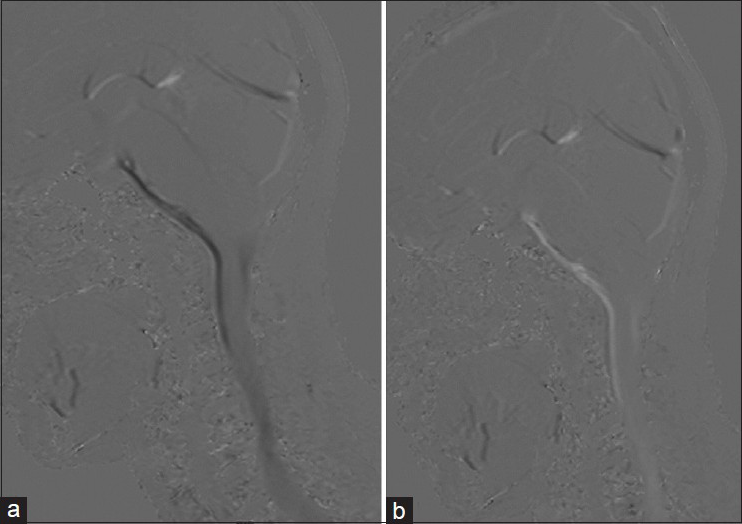
- Cine-MRI showing a block in CSF flow opposite C4-C6 (a and b)
Dynamic flexion-extension x-rays of the cervical spine did not show any instability. Normal lordosis was maintained.
Management
The patient underwent a decompressive laminectomy from C3-C6 and recovered uneventfully following surgery. She was followed up 6 weeks, 3 months and 6 months following surgery and reported significant reduction in the parasthesias. An MRI was performed 3 months following surgery which showed almost complete resolution of the syrnix with small residual signal changes opposite C4 [Figure 3a and b].

- MRI at 3 months following surgery showing resolution of syrinx. T1 (a) and T2 (b) images
Discussion
The association of cervical spondylosis with syrinx is an extremely rare entity with very few previous reports in literature. Lucci, et al. in a description of three cases of neurogenic osteopathy secondary to a syringomyelia found that one of their cases had an associated cervical compressive element at C4.[2] Kimura et al., in 2004, reported a patient with radicular symptoms and a syringomyelic syndrome who was found to have cervical spondylosis with focal C4-5 instability who underwent decompression and stabilization. The patient improved following surgery and a post operative MRI 2 months following surgery showed marked resolution of the syrinx.[3] Rebai et al. reported a 70-year-old patient with features of syringomyelic syndrome who had evidence of cervical cord compression secondary to multiple cervical disc bulges and an associated syringomyelobulbia. The patients symptoms and the syrinx resolved following extensive decompressive lamimectomy, similar to the case reported herein.[4] Kameyama and colleagues described cervical cord changed in nine patients of ossified posterior longitudinal ligament and had one case with a cervical syrinx with significant compression, who improved with immobilization of the neck.[5]
Kaar et al. reported a patient with cervical spondylotic radiculomyelopathy with significant cord compression at C4-6, who underwent anterior decompression and fusion. The patient improved symptomatically but post operative MRI did not show any significant alteration in cord changes.[6]
In 2006, Butteriss, et al. reported another patient of cervical spondylosis who had presented with spastic quadriparesis and was found to have severe cervical spondylosis with compression at C5/6 and C6/7 with an additional syrinx from C7 to D6. Their patient, however, declined surgical intervention.[7]
In a paper on seven cases of syringomyelia without Chiari malformation, Lee et al. noted arachnoiditis, post laminectomy kyphosis, hydrocephalus and focal compressive lesions at D7 and L1 to be associated with syrinxes. Patients were evaluated with pre and post intervention cine MRI and in the cases of post laminectomy kyphosis and compression at D7, surgical decompression at the appropriate level showed improvement in CSF flow post operatively.[8]
Most recently Landi et al. have described a patient who had a cervical syrinx and compression secondary to multiple prolapsed discs demonstrated on a dynamic MRI. The patient underwent decompression and stabilization but on a follow-up MRI the syrinx showed progression.[9]
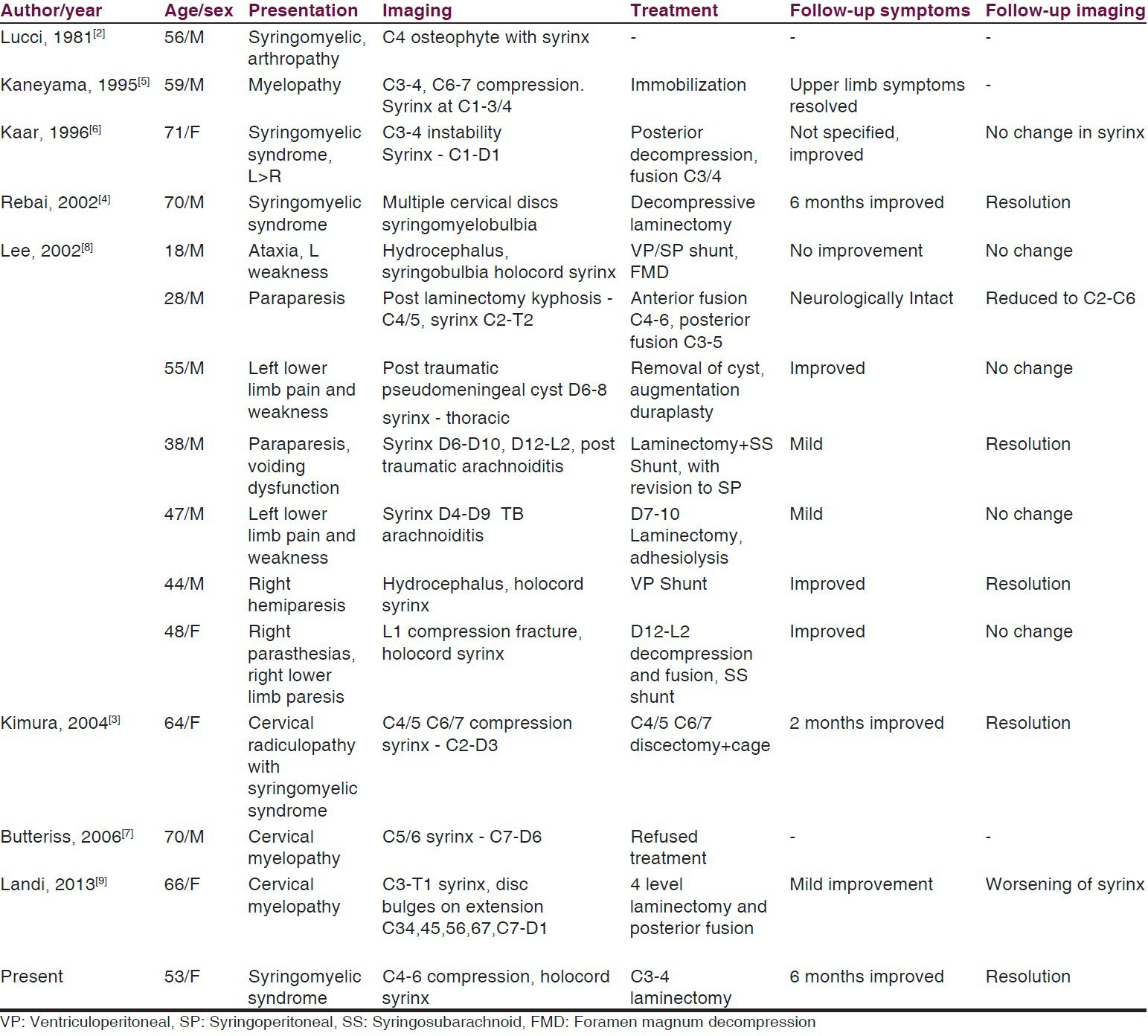
The clinical characteristics, imaging findings, treatment and outcome of patients with these conditions are shown in Table 1.
The theories of genesis of syrnix secondary to cervical spondylosis include ischemia causing degeneration of tracts,[2] microtrauma at the site of compression causing myelomalacia and caviation,[610] a sloshing effect secondary to a local block in CSF flow[311] and dissociation of pressure above and below the block leading to transmural movement of fluid.[12] An extensive review by Klekamp outlines these theories.[13] The most recent theory is the one where the syrinx itself is formed by extracellular fluid movement into the spinal cord parenchyma due to a dissociation of intraparenchymal and subarachnoid pulse pressure.[14] The formation of a syrnix in Chiari I malformations has been attributed to the Bernoulli theorem and an increased velocity of CSF flow across the foramen magnum leading to reduced spinal subarachnoid space pressure and subsequent distension of the cord itself.[14] The various theories of generation of a syrinx in spinal cord compression only point to the fact that our understanding of this pathology is still incomplete. This fact is further endorsed by reports of spontaneous regression of syringomyelia even with Chiari malformations.[15] There is therefore a definite association of syringomyelia with cervical spondylosis and reports of clinical and radiological improvement following decompression with or without stabilization points toward an etiological relationship between the two conditions.
Another valid inference from this case is that historically the presence of myelomalacic changes in the cervical cord, namely hyperintensity on T2w images has been associated with poor prognosis following surgery.[1617] The prognosis is considered worse if there is a corresponding hypointensity on T1w sequences. We propose that some of these patients with limited local changes may represent a “pre-syrinx” stage, as theorized by Fishbein et al., and may therefore have a better prognosis following treatment.[18]
Conclusion
The association of cervical spondylosis with syringomyelia is possibly an etiological one and Cine-MRI with CSF flow studies in addition of evaluation of the CVJ and whole spine to rule out coincidental causes of a syrinx is a valuable diagnostic tool to plan treatment. Decompression of the local pathology often leads to resolution of the syrinx and clinical improvement. The existing concept of cord signal changes in cervical spondylosis being a poor prognostic factor may not be strictly true and a small subset of patients with such changes do show resolution of both clinical symptoms and radiological findings.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Syringomyelia and syringomielic syndrome by cervical spondylosis. Report on three cases presenting with neurogenic osteoarthropathies. J Neurosurg Sci. 1981;25:169-72.
- [Google Scholar]
- Syringomyelia caused by cervical spondylosis. Acta Neurochir (Wien). 2004;146:175-8.
- [Google Scholar]
- Syringomyelobulbia associated with cervical spondylosis. Pathophysiology and therapeutic implications. Neurochirurgie. 2002;48:120-3.
- [Google Scholar]
- Spinal cord morphology and pathology in ossification of the posterior longitudinal ligament. Brain. 1995;118:263-78.
- [Google Scholar]
- A case of syringomyelia associated with cervical spondylosis. Br J Radiol. 2006;79:e123-5.
- [Google Scholar]
- Decompression of the spinal subarachnoid space as a solution for syringomyelia without Chiari malformation. Spinal Cord. 2002;40:501-6.
- [Google Scholar]
- Syringomyelia associated with cervical spondylosis: A rare condition. World J Clin Cases. 2013;1:111-5.
- [Google Scholar]
- Myelopathic cervical spondylotic lesions demonstrated by magnetic resonance imaging. J Neurosurg. 1988;68:217-22.
- [Google Scholar]
- The pathogenesis of syringomyelia associated with lesions at the foramen magnum: A critical review of existing theories and proposal of a new hypothesis. J Neurol Sci. 2004;220:3-21.
- [Google Scholar]
- The pathophysiology of syringomyelia-historical overview and current concept. Acta Neurochir (Wien). 2002;144:649-64.
- [Google Scholar]
- Spontaneous regression of syringomyelia in a young patient with Chiari type I malformation. Neuroradiol J. 2012;25:593-7.
- [Google Scholar]
- Comparison of prognostic value of different MRI classifications of signal intensity change in cervical spondylotic myelopathy. Spine J. 2010;10:475-85.
- [Google Scholar]
- Effect of intramedullary signal changes on the surgical outcome of patients with cervical spondylotic myelopathy. Spine J. 2003;3:33-45.
- [Google Scholar]
- The “presyrinx” state: Is there a reversible myelopathic condition that may precede syringomyelia? Neurosurg Focus. 2000;8:E4.
- [Google Scholar]




