
Translate this page into:
Quality of life of cerebral palsy patients and their caregivers: A cross sectional study in a rehabilitation center Khartoum-Sudan (2014 – 2015)
Address for correspondence: Dr. Fadwa M. S. Mohammed, Department of Community Medicine, Faculty of Medicine, University of Khartoum, Omdurman, Khartoum, Sudan. E-mail: fadwamdsaad@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Cerebral palsy (CP) is group of disorders characterized by long-term disabilities that affect the quality of life (QoL) of both patients and those caring for them.
Objective:
The objective of this study was to measure the QoL of CP patients and their caregivers and determine the factors affecting both of them.
Methods:
This was a cross-sectional facility-based study. 65 caregivers of children with CP aged 4–18 years completed a self-structured questionnaire. Descriptives of the samples were displayed, and logistic regression was used in the analysis.
Results:
The scores of overall QoL of both children and caregivers were low, however, variations were observed among different domains. Both health-related and sociodemographic factors were found to affect the QoL of children and caregivers. The increase in the degree of disability and presence of complications decreased the children QoL while the availability of health insurance improved it. Whereas the QoL of the caregiver was affected by his/her occupation, the degree of child disability did not affect it.
Conclusions:
This study showed that many feasible changes can be adopted to improve the QoL of CP patients and their caregivers.
Keywords
Caregivers
cerebral palsy
quality of life

Introduction
“Quality of life (QoL) is a person's subjective well-being and physical health, material well-being, interpersonal relationships within and outside the family, work and other activities in the community, personal development and fulfillment, and active reaction.”[1]
Cerebral palsy (CP) is the most common physical disability of childhood. “Cerebral” refers to the brain and “palsy” to muscle weakness/poor control. CP itself is not progressive (i.e., brain damage does not get worse); however, secondary conditions, such as muscle spasticity, can develop which may get better over time, get worse, or remain the same.[2] The exact cause of CP is not known yet, however, a group of risk factors has been identified.[34]
CP is a disease that imposes a high burden on the patients, their families, and the health system. This burden is due to both mortality and high rate of disabilities and complications. Factors affecting children with CP QoL include: Factors related to the child (age, gender, and severity of the disease; comorbidity and complications), factors related to the family (socioeconomic status, relationships and support, coping mechanisms, parenting style, and knowledge about the disease), availability of management and rehabilitation services and other environmental factors.[567]
Parents of children with CP in most of the times are those who provide care for their physically challenged children and mostly mothers rather than fathers play the major role in doing this. However, this may be done by a sibling, an aunt or uncle or any other family member. Taking care of a physically challenged child is regarded to be a full-time job with great demands, and it exerts a great stress on the caregiver. Unfortunately, this happens without prior preparation, and the caregiver finds himself suddenly in this demanding situation. The effect of this extends from the economic burden and time spent to the physical, psychological and social aspects of the caregiver. If this issue is not well addressed, it may exert bad effects on the QoL of both the children and their caregivers. Accordingly caregivers QoL and the factors affecting it should be studied thoroughly to improve the care provided and to improve the outcomes of patients and their families. Many factors interact together to shape the effect on the QoL of caregivers; child-associated, caregiver and family associated, environmental and other factors. The aim of this study is to investigate the QoL of CP patients attending a tertiary care center (Cheshire center for physically challenged children) and their caregivers, in Khartoum-Sudan during the study period.
Methods
Study design and area
This study was a cross-sectional; facility based qualitative study conducted in Cheshire center for physically challenged children in Khartoum-Sudan, which is a rehabilitation center that provides physiotherapy, surgeries, and other services for CP and other patients.
Study population
Children with CP attending Cheshire center during the study period and their caregivers. All CP patients, both males and females in the age range from 4 to 18 years attending the center during the study period and their caregivers were included. Caregivers were defined as: The one who spend most of the time with the patient and the main care provider. Patients aged <4 years or >18 years old were excluded.
Sampling
Total coverage over a 5 weeks period started on the 5th of February was done.
Data collection
Data were collected by the primary investigator and two other data collectors (friend doctors for whom items of the questionnaire were discussed and clarified). An interview with each of the caregivers was done to fill the questionnaire, which lasted on average from 15 to 25 min. Only one caregiver completed the questionnaire by herself. The questionnaire consisted of two parts: The first part was structured to collect data about the child and the second for caregiver data. In each section, the first questions collected data about the sociodemographics. The child QoL was assessed in 4 domains: Physical, schooling, social, and emotional. Each domain contained a set of questions that assess it. The same was done for caregivers QoL, however, domains included physical, social, support for care and financial burden.
Scoring
Low responses were given 0 and high ones 1. The total score was computed for each domain separately and overall QoL. The median score for each domain and the total QoL was set as a cutoff to classify scores into low and high. The questionnaire also contained 3 questions to assess the caregiver knowledge about CP; a right answer was given 1 and a wrong one 0. Those who score 3 were classified to have good knowledge, 2 or 1 average and <1 as poor knowledge. Finally, the questionnaire contained questions about the factors to be studied. This questionnaire was self-structured by the authors. Unfortunately, we could not use a standard questionnaire due to the different context in which we conducted our study. However, this questionnaire was developed with the help of the following standard questionnaires: CP QoL Questionnaire, Adult Carer QoL Questionnaire, Pediatric QoL Inventory, Child Health Questionnaire, QoL Index (Generic Version III-Arabic language copy) and Life Style Assessment Questionnaire for Children.
Data entry and analysis
The data were entered into the Statistical Package of Social Sciences (SPSS) version 20 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.) for windows 32-bit. Descriptive statistics (mean, standard deviation [SD], frequencies, and percentages) were computed for sociodemographics, overall and domain-specific QoL and other factors. A series of binary logistic regression models were structured to test the effect of the proposed factors on the two primary outcomes; children QoL and caregivers QoL. Hosmer-Lemeshow Test (HLT) was used to test the goodness of fit of the models.
Ethical issues
This study was approved by the board of community medicine department-Faculty of medicine university of Khartoum and the managers of Cheshire center for physically challenged children. After discussing the objective of the study to the parents/caregivers their oral consent was obtained.
Results
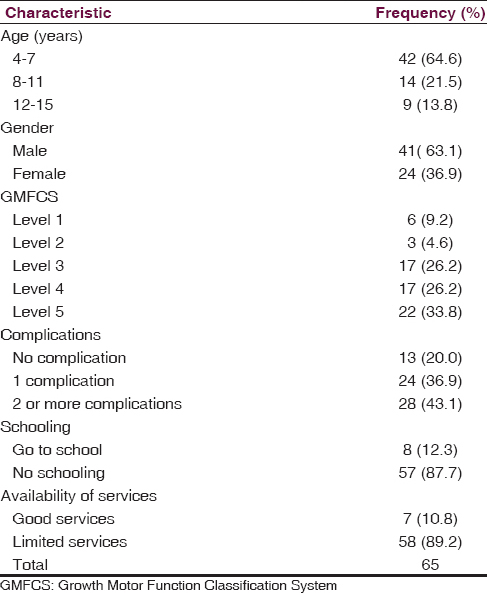
The number of eligible individuals who came during the data collection period was 76, of whom 4 refused to participate, and 7 were missed. Accordingly the final sample consisted of 65 children and their caregivers whose sociodemographic characteristics are shown in Table 1. The most frequently observed complications were: Speech alone, speech and convulsions and a combination of speech, feeding and convulsions.
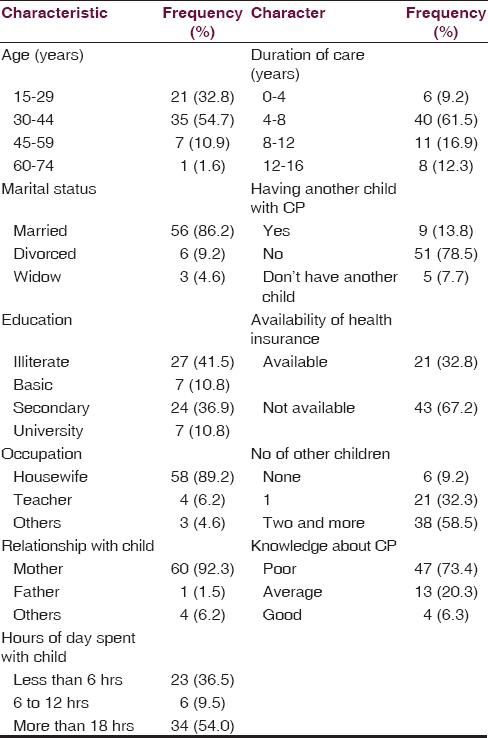
The sociodemographic and other characteristics of caregivers are shown in Table 2. Father was the caregiver in one case. Relatives other than the parents who took care of the child were grandmothers mostly. Activities caregivers did while spending time with their children included: Moving them, feeding, bathing, playing, chatting, going out together, watching television and in few instances teaching the child.
Patients' quality of life
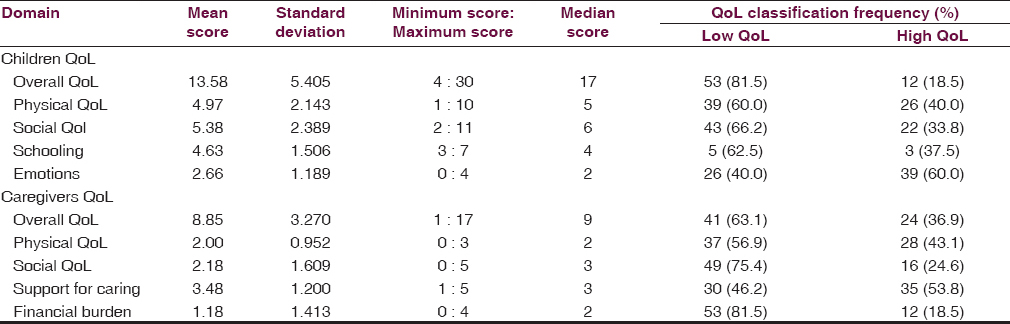
With regard to the primary outcomes of this study; QoL of children and caregivers the results are shown in Table 3. Overall QoL scores of children with CP were low (mean score: 13.58, SD: 5.405). When classified into two groups based on a cutoff (set as the median score which is 16.5), 53 (81.5%) out of the 65 children were in the low QoL class. Score was lowest for the physical domain; however, emotion and schooling domain scores were high.
Caregivers' quality of life
With regard to the QoL of caregivers it was assessed in 4 domains: Physical, social, support for caring, and financial burden. Again the overall mean score was low (8.85, SD: 3.270). Highest scores were observed in the support for care domain and lowest in financial burden.
Of the 65 children, only 8 went to school; 5 of them went to mainstream schools, 1 went to a school specialized in caring for children with disability and the information was missing in the remaining 2. Most of them went to schools nearby their homes. Reasons given by parents that prevented their children from being in school were diverse Figure 1.
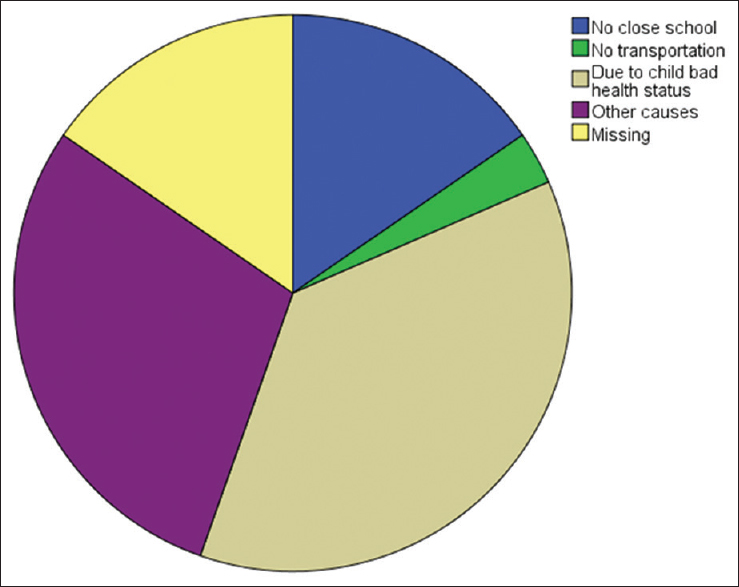
- Distribution of the reasons that led to children inability to go to school
Other causes that forbade children from schooling included: Limited financial resources, unawareness about the presence of specialized schools, and the lack of good and suitable schools.
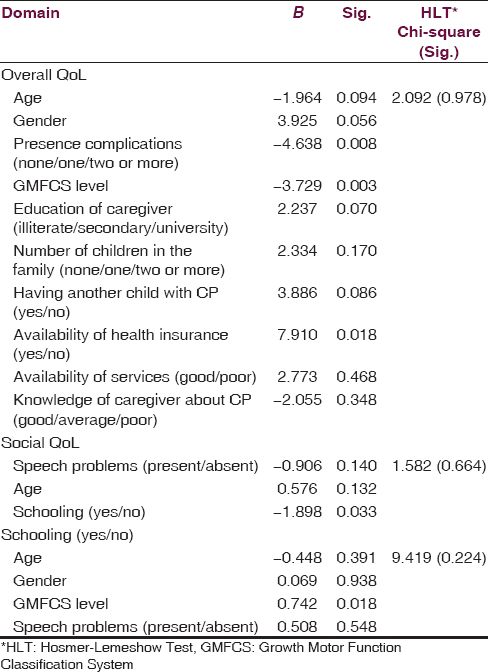
First logistic regression model series: Factors determining children with cerebral palsy quality of life
Three binary logistic regression models were constructed to test the effect of certain factors on children overall QoL [Table 4]. HLT was conducted to test the goodness of fit of the model. It yielded a Chi-square of 2.092 and a Sig. level 0.978, which indicates a good fitting model. 3 of the 10 factors showed a significant effect; the presence of complications was associated with decreased QoL (P = 0.008), increased physical disability as measured with Growth Motor Function Classification System (GMFCS) also was associated with decreased QoL (P = 0.003). Availability of health insurance improved the children QoL (P = 0.018). Age and gender of the patient did not affect overall QoL, nor other family sociodemographics and factors. Although the level of caregiver education, the presence of another child with CP in the family and the age of the child did not reach a significance level, however, they were very close to reach it with P value 0.070, 0.086 and 0.094, respectively. The second regression model in this series tested the effect of age, presence of speech problems and whether going to school or not on the social QoL. Only going to school was associated with improved social performance. The 3rd regression model was structured to test the effect of certain factors on children ability to go to school. Children who have greater physical disability are more likely to not go to school (P = 0.018).
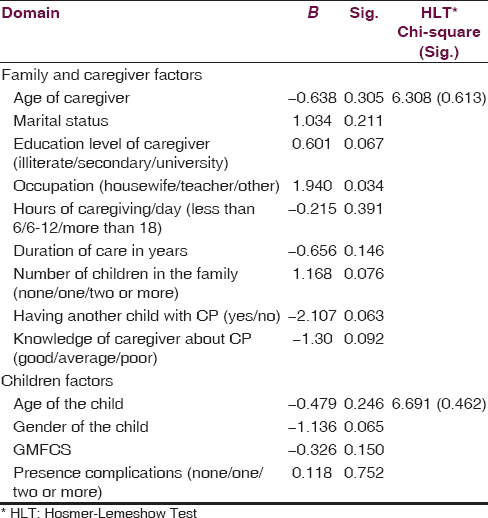
Second logistic regression model series: Factors determining caregivers quality of life
Another two regression models were structured to test the factors determining caregivers' QoL [Table 5]. The first model was specified to test caregiver associated factors. HLT of this model yielded a Chi-square equal to 6.308 with a significance level of 0.613 indicating good fitness of the model. The results of this model showed that caregiver occupation explained some of the variation in their QoL. Although the presence of another child with CP in the family, the level of caregiver education, the number of children in the family and knowledge of caregiver about CP did not reach a significance level, however, they were very close to reach it with P value 0.063, 0.067, 0.076, and 0.092, respectively. The second model was specified for child associated factors. HLT indicated good fitness of the model with a Chi-square value of 6.691 and a significance level of 0.462. None of the child factors studied explained the variation in the caregiver QoL. GMFCS level was far from significance level with a P = 0.752.
Discussion
The overall QoL scores were low in both children and their caregiver with variations observed across domains. Factors related to the health status of the child and sociodemographic factors of children and caregivers were found to affect the QoL of both. The physical disability of CP and the associated co-morbidities impair the QoL; however, these are not the only two reasons why CP patients and their families suffer from a poor QoL. In this study the low socioeconomic status of most of the families attending Cheshire center and the lack of basic services (such as consultation from pediatricians, physiotherapy, and assisting devices) contributed to further decrease the QoL of the children and families. The observed low scores of overall children QoL is in accordance with two previous studies; one in Nigeria[8] and the other in Latvia.[9] On the other hand, our findings are in contrast with a European survey which relied on children's report.[5] They found that children with CP had similar QoL to children in the general population in all domains except schooling, in which evidence was equivocal, and physical wellbeing, in which comparison was not possible. As sated earlier, QoL is a subjective assessment of the person feelings toward his different life aspects. The context in which the individual live greatly influence his norms and values and expectations from life. In Sudan, we are still at the level of providing the basic services to those children and families. The lowest scores obtained were in the physical domain while the highest ones were in the emotions and schooling domain. Although the disabling nature of CP is expected to decrease the QoL of CP patients, the regular and efficient physiotherapy can markedly improve the physical health of the patients. Unfortunately in our study, few of the patients received a regular session of physiotherapy. This was mostly due to financial obstacles and far centers. In our results, we found a significantly better social QoL in those children who go to school. School constitutes a good medium for making new relations and friendships and exposes the child to varying social and personal experiences. The effect of patients' age and gender, GMFCS level and the presence of speech problems on the ability of children to go to school were assessed. Only the increase in physical disability was associated with decreased school enrollment. Although we cannot ignore the effect of physical disability, it should not deprive those children from activities of life. Many of children with CP have apparently normal IQ and can communicate in speech or other ways, in addition many speech therapy techniques are available to improve their ability.
In our study, another significant association was found between availability of health insurance and overall QoL. This can be explained by the fact that health insurance improves the availability of health services. In addition, those who are health insured are more likely to have good financial resources. None of the reviewed studies assessed this factor; however, Greitane et al.[9] found that QoL was influenced by medical interventions which facilitate gross motor functions. Our findings did not reveal a significant association between QoL and services availability.
Although did not reach a significance level in this data it was close to it (P = 0.07); increase in caregiver educational level is expected to improve the QoL of their children. A higher educational level provides opportunities to good occupations, increase the family income and its overall socioeconomic status. In addition, educated parents are more likely to understand the disease of their children which may help them to respond better to their children needs. This finding is contrary to the results of the European study[5] which demonstrated an inverse relationship between parents' education and psychological well-being, autonomy and relationship with parent domains. However, it showed a positive association between education and social acceptance domain. Accordingly, this relationship between caregiver education and QoL seems to be a complicated one with many factors interplaying in the middle to shape the final outcome.
With regard to caregivers QoL, the reported mean score was low. This finding is in accordance with previous studies.[1011] The best score domain was obtained in the support for care, a finding that is matching our country culture of the extended family system and society cooperation. The second best scores were obtained in the physical health domain. In our sample, 87.5% of the caregivers were aged < 45 years. This may explain their good physical health. However, caring for a child with long-term disabilities exposes caregivers to high levels of stress, which may exert itself in the form of an overt organic disease like hypertension, gastritis, and even ulcers. Another problem that deserves special attention in caregivers of children with mobility restriction is the spine and other joints pains. Many of the caregivers reported that they feel fatigue during and at the end of the day, sometimes they find it difficult to do other home activities, however they managed to adapt with the situation. Adding to the problem the fact that parents may ignore their own complaints when their children are sick.
The only factors among caregivers that showed a significant association was the occupation of the caregiver. Majority of the mothers in this study were homemakers. The possible explanation to this finding is that occupation determines the socioeconomic status which in turn affects the QoL. Other factors did not reach the significance level, but they were very close to it. One of these is the level of education. As the level of the education increases the caregiver QoL improves. Well educated caregivers are expected to be in a higher socioeconomic status which may explain this association.
Another factor that was close to show significance is the knowledge of the parents about CP. The knowledge assessed included basic information about the name of the disease, its causes, and management. Many of the mothers did not know that their children can go to special schools. Many did not know other types of management rather than medications, surgery, and physiotherapy. The increase in caregivers' knowledge about the risk factors of CP may prevent the occurrence of the disease in another child. Knowledge about the range of symptoms, diagnosis procedures, management options and expected outcomes helps parents to cope and improve their situation. The failure to demonstrate an association between QoL and knowledge may be attributed to the small sample size.
The results of this study may be limited by the use of a self-structured questionnaire by the investigators instead of using a standard one. However, most of the standard questionnaires were developed in European countries which have a very different context, values, and infrastructure. For example the issue of providing access to schools for those children is no longer a big problem. They are now addressing the issue of improving the performance and QoL of these children with regard to schooling. In our country, the issue is still enabling those children to go to school.
Conclusions and Recommendations
The overall QoL of CP patients and their caregivers was found to be low. Most of the children in our study (87%) did not go to school while those who went to school were found to have a significantly better social QoL. In children increase in the degree of physical disability (GMFCS) and the presence of more complication decreased their QoL, however they had no effect on the QoL of the caregivers which was found be affected by their occupation.
Some interventions can be done to improve the QoL of CP patients: Increasing the focus on treating the associated complications of CP and the provision of adequate physiotherapy services. Ministry of education should exert more effort to enroll the children in schools either mainstream ones – which is better – or in specialized schools and to ensure welcoming and helpful environments in the schools. On the other hand families, QoL can be improved by: More attention addressed to the families in planning the care of their children and the involvement of a psychotherapist in the managing team to improve parents self-efficacy and coping strategies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- What is Cerebral Palsy. Available from: http://www.ucpri.org/who-we-are/what-is-cp
- A systematic review of risk factors for cerebral palsy in children born at term in developed countries. Dev Med Child Neurol. 2013;55:499-508.
- [Google Scholar]
- Intra-partum fever and cerebral palsy in Khartoum, Sudan. BMC Res Notes. 2013;6:163.
- [Google Scholar]
- Self-reported quality of life of 8-12-year-old children with cerebral palsy: A cross-sectional European study. Lancet. 2007;369:2171-8.
- [Google Scholar]
- Factors related to psychosocial quality of life for children with cerebral palsy. Int J Pediatr. 2014;2014:204386.
- [Google Scholar]
- Determinants of quality of life in children with cerebral palsy: A comprehensive biopsychosocial approach. Res Dev Disabil. 2014;35:520-8.
- [Google Scholar]
- Health-related quality of life of Nigerian children with cerebral palsy. 2011. Disabil CBR Inclusive Dev. 22:95-104. Available from: http://www.dx.doi.org/10.5463/dcid.v22i2.24
- [Google Scholar]
- Influence of accessibility of services on quality of life of school children with cerebral palsy in Latvia. EDP Sci. 2012;2:7.
- [Google Scholar]
- Quality of life and mental health among parents of children with cerebral palsy: The influence of self-efficacy and coping strategies. J Clin Nurs. 2013;22:1579-90.
- [Google Scholar]
- Quality of life of mothers of children with cerebral palsy and their age matched controls. 2014. Afr J Neurol Sci. 33:3. Available from: http://www.ajns.paans.org/article.php3?id_article=460
- [Google Scholar]




