
Translate this page into:
Pre-hospital care among victims of road traffic accident in a rural area of Tamil Nadu: A cross-sectional descriptive study
Address for correspondence: Dr. Saurabh R. Shrivastava, Department of Community Medicine, 3rd Floor, Shri Sathya Sai Medical College and Research Institute, Ammapettai Village, Thiruporur-Guduvancherry Main Road, Sembakkam, Kancheepuram - 603 108, Tamil Nadu, India. E-mail: drshrishri2008@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
The World Health Organization has estimated that globally almost 1.24 million people die annually on the world's roads. The aim of the study was to assess the attributes of pre-hospital care in road traffic accidents (RTAs) victim brought to the health care establishment and to evaluate the pre-hospital trauma care provided in the rural areas of Kancheepuram district of Tamil Nadu.
Materials and Methods:
A cross-sectional descriptive study of 3 months duration (June 2014 to August 2014) was conducted in the Shri Sathya Sai Medical College and Research Institute, Kancheepuram. The method of sampling was universal sampling and all RTA victims satisfying the inclusion criteria were included in the study. During the entire study duration, total 200 RTA victims were included. A pre-tested semi-structured questionnaire was used to elicit the desired information after the victims of RTAs are stabilized. Ethical clearance was obtained from the Institutional Ethics Committee prior to the start of the study. Written informed consent was obtained from the study participants (patient/guardian of children) before obtaining any information from them. Data entry and statistical analysis were done using SPSS version 18. Frequency distributions and percentages were computed for all the variables.
Results:
Majority of the RTA victims 158 (79%) were from the age-group of 15-45 years. Most of the accidents were reported in night time [77 (38.5%)], on week-ends [113 (56.5%)], and involved two-wheelers [153 (76.5%)]. Almost 66 (33%) of the victims were not aware of the existence of emergency ambulance services. Also, only 15 (7.5%) victims were brought to the hospital in the emergency ambulance, of which only 3 victims were accompanied by a doctor.
Conclusion:
To conclude, the study indicates that a significant proportion of people were unaware about the emergency trauma ambulance services and the existing pre-hospital care services lack in multiple dimensions in a rural area of South India.
Keywords
Pre-hospital care
road traffic accidents
rural
South India

Introduction
The World Health Organization has estimated that globally almost 1.24 million people die annually and 20 to 50 million people are exposed to non-fatal injuries on the world's roads.[1] In-fact, young adult (15-44 years) contributes almost 60% of global road traffic deaths.[1] Since developing countries contribute a major share of the global burden of road traffic accidents (RTAs), cost of dealing with the aftermaths of RTAs (namely management of immediate complications; disability prevention; and long-term rehabilitation services) adds enormously to the already overburdened health care delivery system.[12]
Realizing the global public health concern, United Nation has declared the current decade 2011–2020 as the Decade of action for road safety, with a goal of first balancing and then minimizing the anticipated magnitude of RTA-associated mortality.[2] A wide range of socio-demographic parameters such as male gender;[3] young age;[3] risk taking behavior;[4] alcohol/psychoactive substances intake;[15] non-use of personal protective equipments;[14] non-compliance with the traffic rules;[14] and delay in provision of prompt medical care to the victims of RTAs;[16] have been identified as potential risk factors in the causation or amplification of the consequences of accidents.
Further, in low-resource communities and remote areas (rural/tribal) with long pre-hospital transport times, most trauma deaths have been reported even before the victims reach the hospital.[789] In-fact, efficient post-crash response has been acknowledged as one of the five pillars (others being: Road safety management; safer roads and mobility; safer vehicles; safer road users) by the United Nation to bring about a significant reduction in the incidence of RTAs.[24] Also, in a non-randomized cohort study done in Iraq, it was observed that efficient pre-hospital trauma system played a critical role in reducing RTA-associated deaths.[10] These facts have seriously necessitated the need for availability and accessibility of good quality pre-hospital care in all areas of the country to minimize the RTA-related morbidity, mortality and disability.[11]
Although over the years trauma institutes and emergency ambulance services have been established in the country, but most of them again remain confined to the urban pockets with minimal efforts from the policy makers pertaining to both strengthening of the emergency response system and creating awareness among the people living in rural areas.[1213] Even findings of studies have shown that factors pertaining to administration and organization, staff qualifications and competencies, availability and distribution of resources, communication and transportation, poor cooperation and coordination, awareness among people, and infrastructure support, either hinder or facilitate an effective pre-hospital trauma care process.[141516] In addition, there is a dearth of studies done with an aim to assess the effectiveness of pre-hospital care in rural area, South India. Thus, the current study has been planned to assess the attributes of pre-hospital care in RTAs victim brought to the medical college and to evaluate pre-hospital trauma care provided in the rural areas of Kancheepuram district of Tamil Nadu.
Materials and Methods
A cross-sectional descriptive study of 3 months duration (June 2014 to August 2014) was conducted in the Shri Sathya Sai Medical College and Research Institute, Kancheepuram district, Tamil Nadu—the hospital, Urban Health Training Centre (UHTC) and Rural Health Training Centre (RHTC). Tamil Nadu state lies in the southernmost part of the India and is surrounded by the union territory of Puducherry, Bay of Bengal, and the states of Kerala, Karnataka, and Andhra Pradesh. In India, Tamil Nadu is the 11th largest state by area, 6th most populous state, 3rd most developed state, and ranks second as far as employment percentage is concerned.[1718] In Tamil Nadu alone in the last 10 years (2005-June 2014), almost 11.9 million new vehicles (transport and non-transport) have been registered, of which ambulances (4489/11934025) constitutes only 0.03%.[19]
The method of sampling was universal sampling and all RTA victims were included in the study. During the entire study duration, total 200 RTA victims were included in the study.
Inclusion criteria
All victims of RTAs during the study period were included in the study after obtaining their informed consent (for children, informed consent from the guardian/parents will be obtained).
Exclusion criteria
Those patients who refused to give their informed consent (one subject) or died (three subjects) before the interview were excluded from the study. In addition, unconscious patients and patients who were hemodynamically unstable were also excluded.
Data collection instrument
A semi-structured questionnaire was used to elicit the desired information. The questionnaire was pre-tested on 10 individuals and based on the obtained responses, the questionnaire was modified. These five subjects were not part of the final study analysis and the modified questionnaire was employed to collect the desired data.
Study variables
The patients’ socio-demographic parameters, place of the accident, the time of accident (day/night), damaged organs, the type of vehicle involved in an accident, pre-hospital care status, pre-hospital time (response time and transport time), and outcome of RTAs.
Methodology
Once the victims of RTAs are stabilized, all the study participants/guardians (in case of children) were interviewed face to face with the help of the pre-tested semi-structured questionnaire after obtaining their written informed consent. Medical officers of the RHTC and UHTC were explained about the purpose of the study and oriented regarding the different aspects of the questionnaire to enable them to collect the data from their respective centers.
Operational definitions
Pre-hospital time interval is the sum of response time (time interval between the occurrences of the RTAs to arrival of the first responding vehicle on the scene) and transport time (time required for reaching the hospital from the site of the accident). B G Prasad's socio-economic status classification was used to categorize the study participants in different socio-economic class.[20] National classification of occupation was used to categorize the workers into skilled, semi-skilled and unskilled type of occupation.[21]
Ethical considerations
Ethical clearance was obtained from the Institutional Ethics Committee prior to the start of the study. Written informed consent was obtained from the study participants (patient/guardian of children) before obtaining any information from them. Utmost care was taken to maintain privacy and confidentiality. The victims were ensured that findings of the study will not have any implications on their career.
Statistical analysis
Data entry and statistical analysis were done using SPSS version 18. Frequency distributions and percentages were computed for all the variables.
Results
Table 1 reflects the distribution of study participants according to their socio-demographic parameters. Majority of the subjects 158 (79%) were from the age-group of 15-45 years. Most of the victims were the driver/pillion rider (177/200), while the rest of them were passengers in the four-wheeler/pedestrians (23/200). Out of the 12 subjects who were below 15 years, 10 were travelling in either four-wheeler or motorcycle, while the remaining two got injured while crossing the road. Most of the study participants were males (145/200), educated (181/200), and employed in semi-skilled (127/200) type (namely agriculture, shop, clerk, etc.) of work.

Table 2 demonstrates the multiple attributes of the reported RTAs. Most of the RTAs were reported on Saturday and Sunday (113/200), especially in rural areas (184/200), with most of them being reported in night time as compared to rest of the day. In addition, most of the victims (driver/pillion rider) injured in accidents were travelling on two-wheelers (namely motorcycle, scooter, etc.) than those on four-wheelers. In most of the RTAs, injuries were not restricted to a single body part, with maximum injuries being in upper and lower extremities. However, only 7 (20.6%) and 33 (21.6%) of the victims were using personal protective measures in four-wheelers and two-wheelers at the time of their accident, respectively. Another 70 (37.4%) injured victims were either using mobile phones or had consumed alcohol at the time of their accident. Also, only 124 (66.3%) victims had a valid license while remaining 33.7% were either not having license at all or the license had expired.
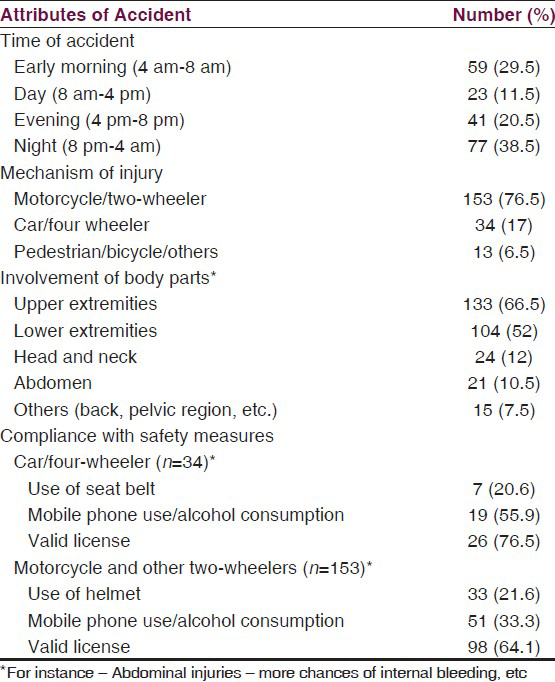
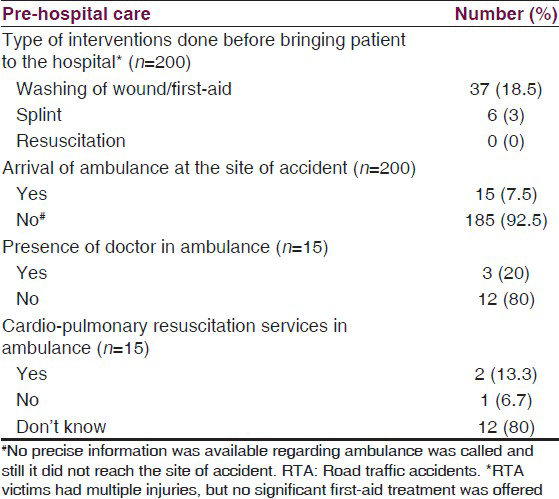
Table 3 demonstrates some of the parameters of pre-hospital care. Only 134 (67%) of the victims were aware of the existence of emergency ambulance services while the rest of them have never heard of the same. Awareness about emergency services in the present study meant that one phone number is available which can be contacted for emergency medical attention at the time of RTAs. Although no precise information was available regarding who called for the ambulance, but most of them was initiated by bystanders or by the victims themselves. Only 15 (7.5%) of the victims were brought to the hospital in the emergency ambulance, while for remaining 185 (92.5%) cases the ambulance either did not reach or was not called for due to the poor awareness among victims/bystanders, or brought to the hospital by other modes of transport. The ambulance took almost 35 ± 15 minutes to reach the site of accident and another 20 ± 10 minutes to reach the hospital from the site of accident. Furthermore, in almost 12 (80%) of the ambulances, no attending doctor was present. No data was available about the functional status of the cardio-pulmonary resuscitation equipment or the competence of the doctor present in the ambulance in carrying out resuscitation activities. Out of the 200 victims of RTA who reached the health care setting, 138 (69%) were managed on an out-patient basis while remaining 62 (31%) were appropriately managed based on their injuries or clinical condition/referred to higher centers for radiological investigations and further management.
Discussion
The current descriptive study has been undertaken to assess the status of the emergency trauma system in a rural area. It is one of the very few studies conducted in the rural pockets of South India and thus findings of the study can be an eye-opener for the program managers.
The present study showed that almost 158 (79%) of the study participants were from the age-group of 15-45 years. Similar sorts of age-group preponderance have been obtained in multiple other cross-sectional studies across diverse settings.[2223] The people from young age-group were involved in most of the settings as they generally have a risk taking behavior and does not abide with traffic regulations in a consistent manner. However, in contrast to most of the other studies, the study revealed that elderly people were the victims of RTAs.[24] This could be because of the rash driving by the vehicle users or because of the delayed reflexes in the old-age or absence of a companion to guide them while they were using the roads. In-fact, both of these extreme age limits indirectly indicate that not only our society but even the public health professionals is lacking in their efforts to protect and nurture them efficiently.
Also, our study revealed that the male: female ratio among the RTA victims was 2.6:1. In-fact, virtually all the epidemiological studies which have been conducted with an objective to assess the determinants of RTAs have shown that males are more commonly involved in RTAs than the females.[222425] This is primarily because of their risk-taking and fearless nature, peer pressure to drive their vehicles beyond the recommended speed limits as compared to the females who usually abide with traffic regulations. This is not a very new finding, but observing the same trend across different settings is of major concern and reflects the minimum reach of both teachers and the concerned health ministry to reach the most vulnerable section of the society.
The present study depicted that a major proportion (56.5%) of RTAs were reported on weekends. Some of the other studies also concluded that RTAs were more common during weekends.[2627] However, in another study to evaluate the effectiveness for emergency dispatch of ambulances, the RTAs were more common in the weekdays.[28] This has been generally attributed to the kind of lifestyle which people adopt in the modern society, where they usually work for 5–6 days a week and weekend is the time to relieve their job-related stress which they might do by consuming alcohol/rash driving, etc.
The current study and other epidemiological studies have revealed that a major proportion of RTAs was seen in night time.[2226] Although different explanations, like absence of traffic police, no traffic signals in night time, less traffic and thus people drive beyond the recommended speed limits, have been cited but other than that complete absence/insufficient lights on the roads, especially in rural areas, as observed in present study is a valid explanation which interferes with the vision and augments the chances of human errors.
It was even observed that two-wheelers (namely motorcycle, scooty, etc.) were more commonly involved in accidents than four-wheelers. Again this finding has been supported by different studies and it essentially indicates the unstable nature of the two-wheelers and reinforces the need that motorcyclist should be over-cautious while driving.[23242627] As evidenced in different studies, even the current study showed that injuries were involving two or more body parts in most of the victims.[682426]
Our study even depicted that only 21.4% (40/187) of the vehicle users were using either helmet or had fastened their seat-belt at the time of their accident. Another study revealed that only 3.1% of the motorcyclist were wearing a helmet at the time of accident.[29] This is one of the most shocking findings as most of the people are aware of the consequences of head injury, but still they are not wearing the same.[30] However, these results can be biased as it does not suggest any details about use of safety measures among people who were killed at the time of accident. In other words, it reflects ignorance from the people and failure of the public health system to motivate people to use personal protective equipments. At the same time, it provides an opportunity for health professionals/outreach workers to grab this opportunity and work in a strategic manner to bridge this knowledge-application gap.[2931] Similar explanation stands true for those commuters who were using either mobile phones or had consumed alcohol while driving their vehicles.[15] Both of them generally interfere with the judgment and skills which are the key component while driving a vehicle and thus definitely aggravates the incidence of RTAs.[1526]
Another finding which questioned the reach of public health services/message was that almost one-fourth of the victims were not aware of the existence of emergency ambulance services. In another study done in Karnataka, almost 72% of the study participants were aware regarding the emergency ambulance services.[13] In-fact, only 15 (7.5%) of the victims were brought to the health care settings in the emergency ambulance, while for remaining cases the ambulance either did not reach or was not called for due to poor awareness among victims/bystanders. However, these results do not reveal the exact picture as some of the victims who died at the time of accident have not been brought to the hospital and thus were not part of the study. Findings of studies have revealed that in most of the low and middle income nations, the pre-hospital trauma care does not match the expected standards and thus a very few percentage of victims receive treatment at the crash scene and even fewer receive safe transport to the hospital by an ambulance.[113233] This is a serious concern, especially in rural areas, which generally lack adequate health care establishments and transport services 24 × 7. However, it will not be right to make any comment regarding the quality/effectiveness of the emergency ambulance services as no precise information was obtained (namely the call has been made but the ambulance did not reach). Nevertheless, this should not be considered as an excuse for 33% of the victims who were unaware about the same. This calls for a strong campaign involving all stakeholders and should ensure affective community participation to warrant long lasting results and reduce RTA-associated morbidity/mortality.
Furthermore, only three (20%) of the ambulances had an attending doctor and it again reflects the shortness of the health care professionals in the health sector. Even other studies have documented that injured people are often accompanied by untrained persons like driver or relatives only.[3132] At the site of the accident in the present study, very few patients 40 (20%) were given any kind of first-aid treatment. In contrast, other studies have shown a wide range of interventions that should be done as a part of pre-hospital care to improve the outcomes.[3435]
Finally, in our study the ambulance took almost 35 ± 15 minutes to reach the site of accident and another 20 ± 10 minutes to reach the hospital from the site of accident. This was almost comparable to other studies which have assessed the pre-hospital time interval in a RTA.[141529]
The strength of the study is that it was one of the first studies conducted in a rural area of South India to assess the effectiveness of pre-hospital emergency trauma system. In addition, due attention has been paid to cover all the involved variables. However, the present study had its limitation that it was a single institution-based study and thus findings of the study cannot be generalized to the entire South India. In addition, as the study was conducted only among the survivors, thus precise assessment of all the attributes of RTAs could not be achieved.
Conclusion
The cross-sectional descriptive study indicates that a significant proportion of people were unaware about the emergency trauma ambulance services and the existing pre-hospital care services lack in multiple dimensions in a rural area of South India. The findings of the study identify the crucial area that is lagging and provide adequate evidence for the program managers to formulate a comprehensive strategy to bridge the existing gap and thus reduce the morbidity and mortality associated with road traffic accidents.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 10 Facts on Global Road Safety. 2013. Available from: http://www.who.int/features/factfiles/roadsafety/en/index.html#
- [Google Scholar]
- Global Plan for the Decade of Action for Road Safety 2011-2020. 2010. Available from: http://www.who.int/roadsafety/decade_of_action/plan/en/
- [Google Scholar]
- Analysis of fatal road traffic accidents in a coastal township of South India. J Forensic Leg Med. 2012;19:448-51.
- [Google Scholar]
- Global status report on road safety. In: Supporting a decade of action, 2013. Geneva: WHO Press; 2013. p. :4-10.
- [Google Scholar]
- Alcohol, psychoactive substances and non-fatal road traffic accidents--a case-control study. BMC Public Health. 2012;12:734.
- [Google Scholar]
- The probability of death in road traffic accidents. How important is a quick medical response? Accid Anal Prev. 2010;42:1048-56.
- [Google Scholar]
- Strengthening care for injured persons in less developed countries: A case study of Ghana and Mexico. Inj Control Saf Promot. 2003;10:45-51.
- [Google Scholar]
- Road-traffic-related mortality in Iran: A descriptive study. Public Health. 2004;118:110-3.
- [Google Scholar]
- Epidemiology of deaths from injuries in the Islamic Republic of Iran. East Mediterr Health J. 2006;12:382-90.
- [Google Scholar]
- Prehospital trauma system reduces mortality in severe trauma: A controlled study of road traffic casualties in Iraq. Prehosp Disaster Med. 2012;27:36-41.
- [Google Scholar]
- Preventing death and disability through the timely provision of prehospital trauma care. Bull World Health Organ. 2006;84:507.
- [Google Scholar]
- Impact of emergency medical support services on public health delivery system in Goa. BMC Proceedings. 2012;6(Suppl 1):14.
- [Google Scholar]
- A study on awareness of 108 ambulance services at district hospital in Hassan, Karnataka, South India: A tertiary care hospital attached to Hassan Institute of Medical Sciences (HIMS) Int J Biol Med Res. 2013;4:2864-6.
- [Google Scholar]
- Barriers and facilitators to provide effective pre-hospital trauma care for road traffic injury victims in Iran: A grounded theory approach. BMC Emerg Med. 2010;10:20.
- [Google Scholar]
- Emergency Medical Service (EMS) systems in developed and developing countries. Injury. 2007;38:1001-13.
- [Google Scholar]
- Post-crash management of road traffic injury victims in Iran. Stakeholders’ views on current barriers and potential facilitators. BMC Emerg Med. 2009;9:8.
- [Google Scholar]
- Ministry of Home Affairs, India. Census of India 2011. 2011. New Delhi: Office of the Registrar General and Census Commissioner; Available from: http://censusindia.gov.in/2011-prov-results/prov_results_paper1_india.html
- [Google Scholar]
- NDTV. Rajan report: Odisha, Bihar least developed; Goa, Kerala on top. 2013. Available from: http://profit.ndtv.com/news/economy/article-rajan-report-odisha-bihar-least-developed-goa-kerala-on-top-327723
- [Google Scholar]
- State Transport Authority, Government of Tamil Nadu. Newly registered vehicle. 2014. Available from: http://www.tn.gov.in/sta/regtrans.PDF
- [Google Scholar]
- Revision of Prasad's social classification and provision of an online tool for real-time updating. South Asian J Cancer. 2013;2:157.
- [Google Scholar]
- National Classification of Occupations. 2004. Available from: http://www.nsdcindia.org/pdf/nco2004-code-structure.pdf
- [Google Scholar]
- An epidemiological study on the road traffic accidents from hills of north India. Burn Trauma. 2014;2:71-5.
- [Google Scholar]
- Injury characteristics and outcome of road traffic crash victims at bugando medical centre in Northwestern Tanzania. J Trauma Manag Outcomes. 2012;6:1.
- [Google Scholar]
- Motor vehicle trauma: Analysis of injury profiles by road-user category. Emerg Med J. 2006;23:27-31.
- [Google Scholar]
- Building national estimates of the burden of road traffic injuries in developing countries from all available data sources: Iran. Inj Prev. 2009;15:150-6.
- [Google Scholar]
- Epidemiological study of road traffic accident cases from Western Nepal. Indian J Community Med. 2010;35:115-21.
- [Google Scholar]
- Road traffic collisions in Bursa, Turkey, during 2003, 2004 and 2005. Injury. 2008;39:547-53.
- [Google Scholar]
- Evaluating the effectiveness of telephone triage for priority emergency ambulance dispatch. J Clin Diagn Res. 2009;3:1726-30.
- [Google Scholar]
- Pre-hospital trauma care in road traffic accidents in Kashan, Iran. Arch Trauma Res. 2013;1:166-71.
- [Google Scholar]
- The impact of mandatory helmet law on the outcome of maxilla-facial trauma: A comparative study in Kerala. J Maxillofac Oral Surg. 2014;13:176-83.
- [Google Scholar]
- The problem of the pillion rider: India's helmet law and New Delhi's exemption. J Surg Res. 2014;188:64-8.
- [Google Scholar]
- Emergency medical systems in low- and middle-income countries: Recommendations for action. Bull World Health Organ. 2005;83:626-31.
- [Google Scholar]
- Evaluation of gasometric parameters in trauma patients during mobile prehospital care. Rev Col Bras Cir. 2013;40:293-9.
- [Google Scholar]
- An observational study of paediatric pre-hospital intubation and anaesthesia in 1933 children attended by a physician-led, pre-hospital trauma service. Resuscitation. 2014;85:189-95.
- [Google Scholar]




