
Translate this page into:
Main Neurosurgical Pathologies in Benin Republic
Address for correspondence: Dr Hugues Jean-Thierry Gandaho, Department of Health Sciences, University of Abomey-Calavi, 03 BP 3657 Cotonou, Benin Republic. E-mail: jeampyg@hotmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Benin republic is a very low-income French-speaking country in West Africa The development of Neurosurgery in the Republic of Benin took off with the arrival of the first Beninese neurosurgeons in the year 2003.
Aims:
This study aims to evaluate patients’ attendance in a public neurosurgical center, and appreciate populations’ affordability to a new specialty.
Settings and Design:
In the year 2004, the Benin Armed Forces established the first Department of Neurosurgery in the Nation's Military Teaching Hospital. From the public authorities, that was a proof of motivation to develop this specialty in the Benin Republic.
Materials and Methods:
A retrospective cross-sectional survey (September 2003 to December 2009) of the total neurosurgical patient population managed in a public pioneer hospital in a developing country.
Statistical Analysis Used:
Data were captured and analyzed with the SPSS software (SPSS Inc., Chicago, IL, USA) and presented in descriptive statistics such as frequencies and proportions.
Results:
2908 new patients, civilians, and militaries were registered. The surgical treatment was offered adult (86%) as well as pediatric (14%) patients. Spinal degenerative diseases (52.1%) were the most common pathology; neurotraumatology emergency cases (8.4%) appeared low in representation. Three-quarters of patients experienced financial difficulties to procure the required radiologic investigations and although 609 (20.94%) benefited from surgery, most patients could not pay for the surgical operations as well as the perioperative care.
Conclusions:
In spite of the great constraints of this country's privately-funded health-care delivery system on the affordability of neurosurgical treatment for the average Beninese, this study demonstrates a globally increasing attendance of the department.
Keywords
Benin Republic
disease burdens
low-resource neurosurgical practice
neurosurgery
socioeconomics

INTRODUCTION
Neurosurgery is the specialty that deals with surgical care of the pathologies of the nervous system. Its development remains dependent on the experimental physiology of the nervous system and was marked by the works of famous pioneer neurologists like Sir William Richard Gowers, and his protégé, Sir Victor Horsley. The latter was the first to operate successfully, in 1887, on a medullary tumor in the National Hospital of London,[1] Benin Republic is a small French-speaking country of about 10 million people in West Africa. The development of Neurosurgery in Benin is a very recent event and is marked by the arrival in the country of the first 2 Beninese neurosurgeons, both trained abroad, in the year 2003. From 2003 to 2009, these two pioneers have been dealing with that specialty in Cotonou. The country's Military hospital inaugurated the nation’s first formal Neurosurgical Department, and to date remains the far leader in technical equipment acquisition as well as the volume of operative neurosurgical activities. It is thus in most vantage position to give a global view of the main neurosurgical pathologies and the challenges of treating them in Benin Republic's health system, a privately-funded, fee-for-service one as in most low-middle income countries of the world.
The previous works in Benin of Avode et al.[2] and Central African Republic with Mbelesso and Tatangba-Bakozo[3] reported the main clinical symptoms in neurology and underlined the diagnostic difficulties related to the absence of individualization of the departments or to the lack of access to diagnostic explorations.
These socioeconomic realities handicap daily care of the neurological pathologies, more particularly so in the setting of a Neurosurgical Department.
That is why, after a decade of regular practice in the Department of Neurosurgery of the Military Hospital in Cotonou (HIA), we aim to report the epidemiological characteristics of the main neurosurgical pathologies in this country, and to highlight the challenges to the optimal accessibility of the population of Benin to this inherently expensive type of surgical care.
MATERIALS AND METHODS
The study was a retrospective cross-sectional survey of the neurosurgical patient population managed by the principal author in the Department of Neurosurgery of the Military Hospital in Cotonou (HIA). This tertiary care hospital, being a Military hospital in Benin Republic has an inpatient capacity of only 15 beds. The military infrastructure could as yet not provide services related to emergency department needed for emergency surgical care, or neuroresuscitation. It could not accept pediatrics hospitalization yet either. There is no facility for emergency imaging or vascular explorations. Twenty-four-hour on-call clinical evaluation for neurosurgical emergencies are as yet a luxury. Finally, the geographical and financial access for the patient population remains dependent on the privately funded, point-of-service payment for health care, the health-financing model for all the other infirmities in the country.
The present study is a retrospective descriptive analysis of patients’ files available in the department following hospitalization, consultations, and operative military neurosurgical campaigns between September 23, 2003, and December 31, 2009.
The recruitment was exhaustive. The main variables of the study were the patients’ sociodemographic characteristics including the age and the sex as well as the nature of the neurosurgical pathologies.
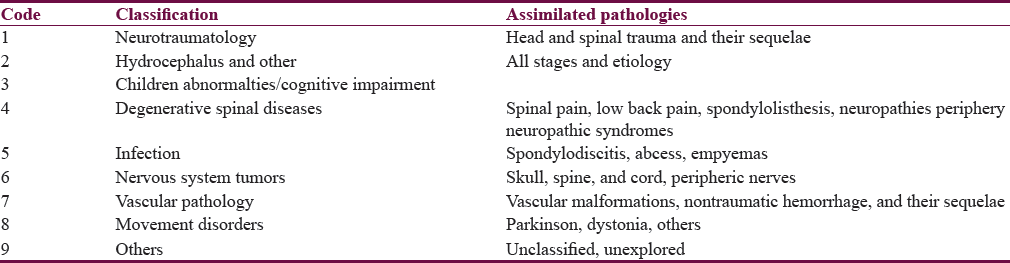
To facilitate the data analysis, the main identified neurosurgical pathologies had been coded and grouped in nine categories of clinical picture [Table 1]. Incomplete files or cases whose clinical evaluations were not conclusive were excluded from the study. Examples of cases with inconclusive clinical evaluation were cases that following their initial presentation in the outpatient department could not procure the proposed diagnostic neuroimaging and usually failed to present for follow-up evaluation. Data were captured in an electronic spreadsheet and analyzed with the software SPSS version 21 (SPSS Inc., Chicago, IL, USA). It is presented in descriptive statistics such as frequencies and proportions.
RESULTS
During the period of study, 2908 cases, adults, and children were reviewed. There was a slight male preponderance, with a ratio of 1.12. Age and sex distributions, followed by yearly incidences, are summarized in Figures 1 and 2. Figure 2 shows attendance in our Department of Neurosurgery quickly increasing, apart from some occasional dips, from the last quarter of 2003 onward.
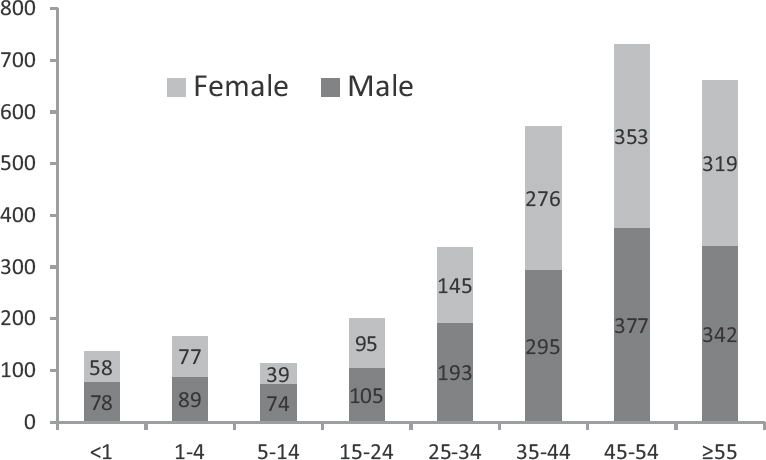
- Main neurosurgical pathologies in Benin Republic, age, and sex distribution
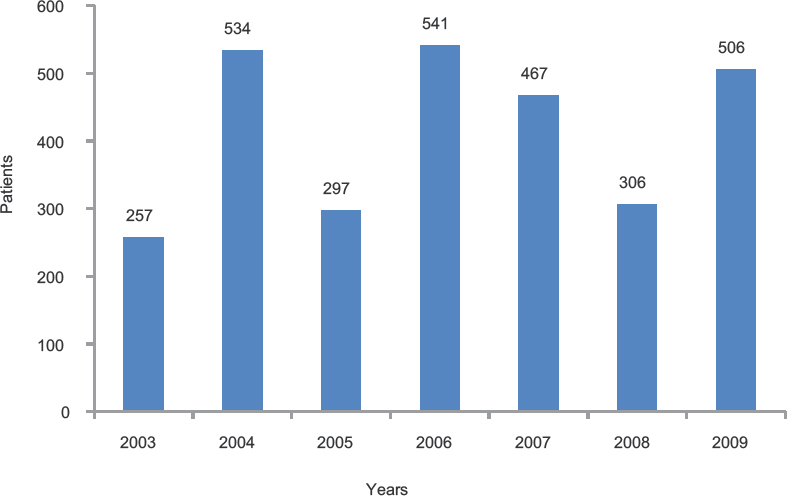
- Neurosurgical pathologies encountered in Benin Republic, yearly case distribution
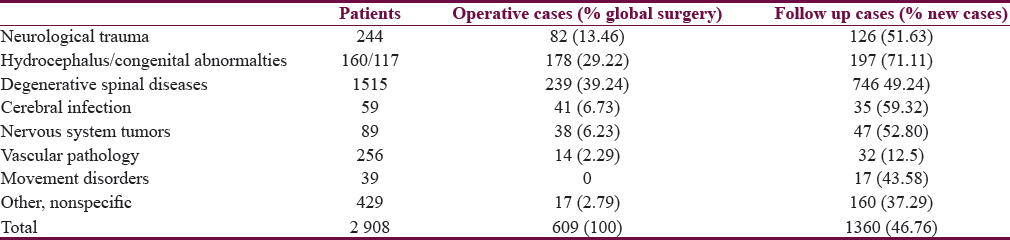
In Table 1, the main groupings of the clinical presentation of the neurosurgical pathologies in this study subjects are shown. They include neurotrauma, congenital anomalies of the central nervous system (CNS), spinal degenerative diseases, and so on. The proportional distribution of these diagnoses in this patient cohort shows that the degenerative spinal diseases were the dominating reason for consultation, with up to 52% of attendances.
Figure 3 illustrates the distribution of the neurosurgical disease presentations according to the patients’ age groupings. In the children's population, hydrocephalus and neural tube abnormalities were the most usually observed pathologies accounting, respectively for 50.8% and 34.6% in terms of frequency in those <1 year of age, and 25.9% and 27.1% in the age group 5–14 years. For patients aged over 15 years old, hydrocephalus was still observed in 11.5% of cases.
- Main neurosurgical pathologies in the Benin Republic, proportion of patients with respect to age groups
Degenerative spinal diseases represent 49.4% of the demand for neurosurgical care among subjects aged 25–34 years old, and more than 60% for patients older than 35 years.
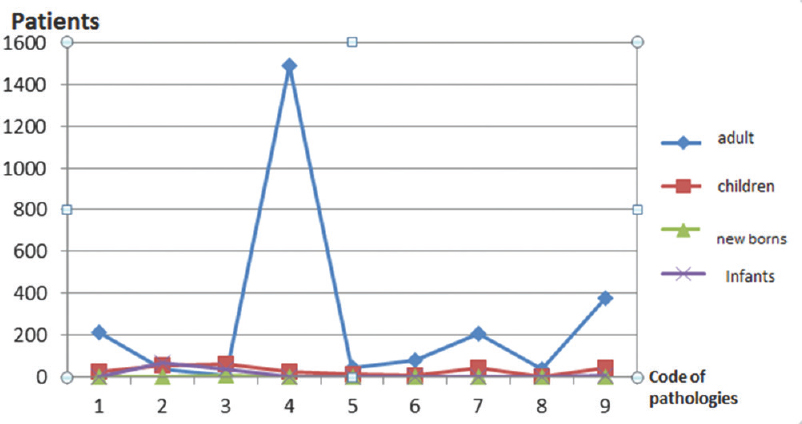
By considering the most common pathologies in the department during the last 3 years of the study, there was an increasing attendance for degenerative spinal diseases, hydrocephalus, congenital abnormalities, and trauma cases. On the other hand, the vascular pathologies show nonlinear course [Figure 4].
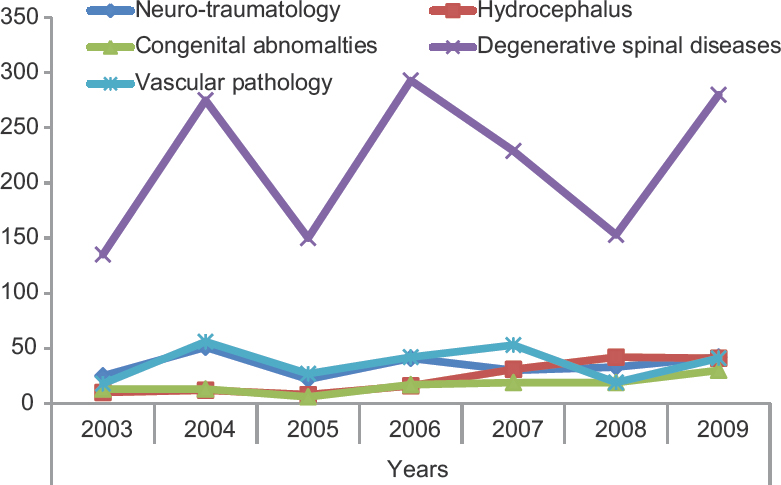
- Main neurosurgical pathologies in the Benin Republic, yearly trends of the clinical diagnosis over the study period
Regarding clinical evaluations for patients presenting in emergencies, 244 patients had information available regarding the status of the requested radiological evaluations. None of them could afford magnetic resonance imaging (MRI) evaluation whereas, respectively, 174 (71.33%) and 70 (28.68%) had access to plain X-ray and computed tomography (CT) scans.
Of the total number of new cases (n = 2908), 1360 received only clinical treatment/symptom control while 609 benefited from surgical procedures. Clinical follow-up could be performed in 46.76% of new cases. The rates seem higher regarding pediatric cases, (71.11%); but remain very low when considering vascular disorders (1.5%). Definitely, certain conditions (spine, pediatric neurosurgery) benefited from more surgical procedures than others (tumoral or vascular) [Table 2].
DISCUSSION
In this study, 2908 neurosurgical conditions were documented over a 6-year period in a new, pioneering neurosurgical service from the Republic of Benin, West Africa. This brings an annual average attendance of 484 patients. In 1997, and from the same country, Avode et al.[2] reported in Cotonou, an average annual distribution of neurological diseases of 275 cases; this was approximately 13% of the hospitalizations of the Department of Internal Medicine of the University Hospital. 5 years later, Mbelesso and Tatangba-Bakozo[3] published in Bangui, another West African country, a similar attendance of 250 neurological patients, which represented 48% of all inpatients in their specialized department.
In Côte d’Ivoire, there were several well-equipped Departments of Neurology. Aka Anghui Diarra et al.[4] reported their own experience of 1000 yearly cases; 19.3% were pupils and students. On the contrary, in a reference center of neurosurgery in Newcastle, England, serving a population close to that of Cotonou, Mukerji et al.[5] reported an annual average of 2801 admissions, that is >5 times the attendance noticed in the present study. This underlines well the low density of neurosurgeons in our country, an African fact already reported by El Khamlichi:[6] 1 neurosurgeon for 7 million inhabitants in sub-Saharan countries.
Degenerative spinal diseases (n = 1515, 52.1%) were the most common pathologies seen in this study. This was similar to a study in the year 2000 in Lomé, Togo, a neighboring country by Mijiyawa et al.,[7] through a series of 9065 patients of whom 35.34% suffered from low back pain.
Due to the suboptimal level of availability and functionality of important medical equipment in most developing countries, Adeleye et al.[8] reported in 2012 that some neurosurgical pathologies are underinvestigated and hence underdiagnosed. This is particularly true for vascular lesions in the present study. Supporting this idea, Hurtado et al.[9] reported that spinal surgery (40.1%) was more practiced than craniotomies for tumor removal (24.1%). Park[10] also noted the difficulty of obtaining essential MRI diagnostics for spinal lesions; hence, on the continuing need for cheaper procedures such as myelography in 16 developing countries.
Pediatrics considerations
Pediatric neurosurgical pathologies were about 16.36% of the total attendance in this department, whereas Aka et al.[4] reported 11% in Abidjan. In this study population, hydrocephalus was the most frequent pathologies with 39.11% of pediatric neurosurgical cases. In two units of neonatology, Lalya[11] reported in 2006 that 9.1% of children will develop hydrocephalus after meningitis. From a prospective survey on 36 children treated for meningitis in the same units conducted about 10 years later, Yekpe[12] reported in 2013, 22 (61.11%) various infectious complications, most frequently hydrocephalus (n = 11; 50%), brain abscess (n = 6; 27.27%), and empyema (n = 3; 13.63%). Delayed presentation leading to delayed diagnosis, as well as the absence of quick screening investigation like simple ultrasound scanning in these low-resource practice units, leads to further delayed diagnosis of intracranial complications of meningitis in the pediatric age group. Children on treatment for meningitis should benefit from a closer ultrasound screening to rule out possible hydrocephalus or other infectious complications for accurate and appropriate therapeutic response, to achieve a better cognitive development after meningitis.
Neurological abnormalities account for 28.6% of pediatric cases in the unit. One possible reason for this lower incidence is that the women populations have low accessibility for antenatal diagnosis in this region of the world. Djientcheu[13] in Cameroon reported that antenatal ultrasound was performed in only 32.8% of cases, whereas Munyi[14] in Kenya had reported delayed diagnosis up to 3 years of age for some children's abnormalities.
There was a gradual yearly increment of the frequency of neurosurgical pathologies in the children population presenting in this study period: 31 (12.0%) in 2003, 63 (11.72%) in 2005, and then 83 (17.77%) in 2007. This suggests a progressive improvement in the awareness of the local populations to the neurosurgery services rendered by our department. In the particular aspect of pediatric neurosurgical pathologies, much efforts are still needed to enforce knowledge among local communities and increase their adhesion to modern medical care related to children neurosurgical pathologies.
Other pathologies weakly represented
Vascular pathology had relatively low frequency (8.6%) and present the lowest rate in surgical activity (2.3%). As underlined by Aguemon,[15] CT scan was performed only in 5% of the patients admitted in coma. In emergency situations, there is no angiography and the few-slides-only CT machine available in our country does not allow the feasibility of vascular reconstructions. These various handicaps explain the poor prognosis and other statistical gaps of vascular pathologies in our experience. Thus, while reporting on vascular problems in Benin, Avode et al.[2] in an era before the availability of the first CT scan machine in our country, established an overall mortality of 48.3%. This is much higher mortality burden from this disease when compared with the lower burden, 19% reported by Aka et al.[4] in Côte d’Ivoire.
Regarding neurotraumatology cases, about 244 admissions representing only 8.4% were recorded. Preacely[16] in a paper from Nigeria reported that road accidents (9%) achieved the second position of the five first causes of death after HIV/AIDS which accounted for 21%. The mortality was 8.85% that represents 41.32% of the global mortality of the hospital during the same period. In another study with similar duration to ours, Kudebong[17] reported in Ghana that commercial motorcycles constituted 98% of registered vehicles in a city in the northeast of Ghana and that they had caused 410 traffic accidents, that is twice the figures we mentioned in our study.
Several reasons could be adduced for the low rate of traumatic lesions among our neurosurgical patient populations. One of them is the poor state of the prehospital trauma care, including inter-hospital transportation, in our country. Aguemon[15] in 2005 published that only 9% of trauma patients could benefit from a medical transportation to the hospital. In HIA, Cotonou Military Hospital, one should also take into account two major handicaps: The absence of a department of emergency care, and the high cost of CT scan (80,000 F local currency, i.e., 160 US dollars) that is approximately 2½ times the minimum salary in Benin population. These problems of accessibility have also been reported by Avode et al.[2] when dealing with nonvascular motor impairment and late-onset seizures in adult: Respectively, only 17.64% and 8.1% of patients could afford the CT scanning requested.
Analysis of the surgical activity
As seen in Table 2, spinal surgery (39.24%) and pediatric neurosurgery (22%) were the first two dominating conditions among 609 operated cases. It appears that affordability of the needed diagnostic investigations (radiological and others), the need of specific surgical equipment, the levels of technical skills of the surgical team, and the ability of public facilities in managing a new field of specialty, are key parameters that introduce bias in patients selection for surgery: Conditions such as vascular lesion and brain tumor that require multistage neuroradiology evaluation, long stay in intensive care unit, and complex surgical tools are weakly represented compared to those who could be managed through daily surgery and whose assessment are somewhat amenable to low-cost investigations such as plain X-ray or ultrasonography. Examples include spinal lesions, hydrocephalus, or craniospinal dysraphism. In a hospital in Catalonia in Spain, Hurtado[9] reported in 2003, a series of 6909 procedures dominated by spinal surgery (39.2%) and pediatric neurosurgery (24.3%); CNS tumors were weakly represented (7.1%). In another African country, Sakho[18] reported his own experience in Dakar (Senegal): 21 cases of tumors operated in 4 years, whereas Eyenga[19] in Cameroon reported as for him a rate of 6.3% related to tumoral surgery within the global surgical activity.
CONCLUSIONS
The present study points out numerous handicaps related to poverty and human resources management in our country, the Republic of Benin: poor state of the prehospital trauma care, absence of a department of emergency care, and quick screening, a globally low access to radiologic evaluation challenges and finally, delayed presentation leads to delayed diagnosis. In addition, certain pathologies such as neurotrauma and vascular diseases remain weakly represented.
These are key factors responsible for apparent poor attendance in our public neurosurgical unit; thus generating some bias on patient's selection for surgery. Despite all these, the study demonstrates a generally increasing neurosurgical activity in our young Neurosurgical Department.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The genesis of neurosurgery and the evolution of the neurosurgical operative environment: Part I – Prehistory to 2003. Neurosurgery. 2003;52:3-19.
- [Google Scholar]
- Main neurological diseases in National University Hospital, Cotonou-Benin. Le Béin Méd. 1997;6:14-7.
- [Google Scholar]
- Hospital incidence of major neurological diseases in Bangui (Central African Republic) Le Béin Méd. 2006;32:12-5.
- [Google Scholar]
- Outpatient neurological consultations in Abidjan- Cote d’Ivoire: four years’ experience. Le Béin Méd. 2007;37:21-4.
- [Google Scholar]
- Emergency neurosurgical referrals in the North East of England – Trends over four years 2008-2011. Br J Neurosurg. 2013;27:334-9.
- [Google Scholar]
- African neurosurgery: Current state and future prospects. Jpn J Neurosurg. 2004;13:292-3.
- [Google Scholar]
- Low back pain in hospital outpatients in Lomé (Togo) Joint Bone Spine. 2000;67:533-8.
- [Google Scholar]
- Skull base surgery in a large, resource-poor, developing country with few neurosurgeons: Prospects, challenges, and needs. World Neurosurg. 2012;78:35-43.
- [Google Scholar]
- And Grupo Anescat. Neurosurgical activity in Catalonia: Results of an anesthetic survey in 2003. Neurocirugí. 2007;18:492-5.
- [Google Scholar]
- Myelography as a stand-alone diagnostic procedure for degenerative spine disease in developing nations. World Neurosurg. 2010;73:285-8.
- [Google Scholar]
- Purulent meningitis in children at National University Hospital in Cotonou-Benin: Clinical and biological management and follow up. In: Le Bénin Méd. Vol 33. 2006. p. :29-31.
- [Google Scholar]
- Complications in meningitis and follow up by cranial ultrasound in neonates and infants in Cotonou-Benin. Le Béin Méd. 2012;51-52:11-6.
- [Google Scholar]
- Management of neural tube defects in a Sub-Saharan African country: The situation in Yaounde, Cameroon. J Neurol Sci. 2008;270:29-32.
- [Google Scholar]
- Encephalocele – A single institution African experience. East Afr Med J. 2009;86:51-4.
- [Google Scholar]
- Intensive care management of patients with severe head traumatism in Benin from 1998 to 2002. Ann Fr Anesth Reanim. 2005;24:36-9.
- [Google Scholar]
- Hospital-based mortality in Federal Capital Territory hospitals – Nigeria, 2005-2008. Pan Afr Med J. 2012;11:66.
- [Google Scholar]
- Economic burden of motorcycle accidents in Northern Ghana. Ghana Med J. 2011;45:135-42.
- [Google Scholar]
- Management of cranial meningiomas in a neurosurgical unit, in Dakar. Afr J Neurol Sci. 2005;24:45-54.
- [Google Scholar]
- Central nervous system tumours in Cameroon: Histopathology and demography. Sante. 2008;18:39-42.
- [Google Scholar]




