
Translate this page into:
Is Thalamic Lesion a Contributing Factor for Inappropriate Sexual Behavior in Older Adults with Cognitive Impairment?
 , Namrata Jagtap2, Krishna Prasad Muliyala3, P. T. Sivakumar2, Preeti Sinha2, Sandhya Mangalore4, Mathew Varghese2
, Namrata Jagtap2, Krishna Prasad Muliyala3, P. T. Sivakumar2, Preeti Sinha2, Sandhya Mangalore4, Mathew Varghese2
Krishna Prasad Muliyala, MBBS, MD Department of Psychiatry, National Institute of Mental Health and Neurosciences Bengaluru 560029 India krishnadoc2004@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Thalamus is a group of nuclei located deep inside the brain, well known for its sensory and cognitive functions. However, its role in the reward and behavior regulation is less explored. In this case series, we have presented four cases with inappropriate sexual behaviors (ISB) that are temporally related to thalamic infarction. We have discussed about the limbic part of thalamus and its extensive connections with other regions in regulating sexual behaviors. Although in all the four cases described there was underlying cognitive impairment that can itself increase the risk of ISB, there was potential contributing role of thalamic lesions.
Keywords
thalamus
older adults
inappropriate sexual behaviors
cognitive impairment

Introduction
Sexual behavior in humans is a complicated process subserved by both central and peripheral nervous systems. Appropriate sexual behaviors are a result of precise balance of reward system and inhibitory processes. Any disturbance in this balance will result in either decreased or increased regulation of sexual behavior. Central nervous system structures mediating sexual behaviors are primarily components of limbic system such as hypothalamus, amygdala, insula, and cingulate cortex. Cortical structure that is involved in regulating the sexual behavior is the prefrontal cortex (PFC), specifically the orbitofrontal cortex (OFC).1 Hypersexual behaviors involving lesions in these structures have been reported secondary to infarcts, traumatic brain injury, and postsurgical interventions.2
Thalamus, a paired gray matter subcortical structure, is made up of a series of nuclei that are responsible for receiving different sensory signals and plays an important role in episodic memory and learning. Although thalamus is important for the reward pathway, as a part of limbic system, its role in sexual behaviors is less explored. A few case studies that explored the role of thalamus in sexual behaviors have reported lesions of ventral thalamus and paramedian nucleus to be implicated in inappropriate sexual behaviors (ISB).3 4 Recent studies have also emphasized the importance of thalamus in regulating PFC and thus controlling sexual behavior.5
In this article, we have presented four cases presenting with inappropriate sexual behaviors following thalamic infarct (Table 1). We have reviewed the available literature on role of thalamus in sexual behavior.
|
Sl. no |
Author, year |
Age, sex |
Sexual misbehavior |
Other features |
Imaging finding |
Functioning |
Major neurocognitive disorder |
|---|---|---|---|---|---|---|---|
|
1 |
Muller et al,7 1999 |
NA |
Hypersexuality |
Hyperphagia, hypersomnia, amnesia, impaired attention |
MRI-bilateral thalamic infarcts PET-hypometabolism in ventral thalami and frontotemporal cortex |
Impaired |
NA |
|
2 |
Spinella4 2004 |
66 years/M |
Inappropriate sexual behavior and scatological remarks |
Witzelsucht, blunted affect, confabulation, amnesia, hypersomnia, utilization behavior |
Thalamic infarct following aneurysm bleed |
Impaired |
NA |
|
3 |
Mutarelli et al,3 2006 |
63 years/M |
Hypersexuality and disinhibition |
Anterograde amnesia, irritability and hypersomnia |
Bilateral thalamic paramedian nucleus infarct. SPECT-bilateral hypoperfusion |
Impaired |
NA |
|
4 |
Case A |
72 years/M |
Inappropriate sexual behavior |
Apathy, executive dysfunction, impaired episodic memory, paranoid ideation |
Subacute infarct in right thalamus |
Impairment in complex and basic activities of daily living |
Mixed dementia (AD+ VaD) |
|
5 |
Case B |
62 years/M |
Inappropriate sexual behavior |
Executive dysfunction, impaired episodic memory, agitation/aggression |
B/L thalamic infarct |
Impairment in complex activities with preserved basic activities |
Vascular dementia |
|
6 |
Case C |
63 years/F |
Inappropriate touching |
Executive dysfunction, unprovoked aggression, impulsive behaviors, dietary changes |
Right thalamic infarct |
Difficulty in complex activities |
Vascular dementia |
|
7 |
Case D |
93 years/M |
Inappropriate sexual behavior |
Impaired attention and episodic memory |
Left thalamic infarct |
Difficulty in complex activities |
Mild cognitive impairment |
Abbreviations: NA, not available; PET, positron emission tomography; SPECT, single-photon emission computed tomography.
Case Report
Case A
A 72-year-old gentleman, right-handed, hypertensive, on regular medication for the last 3 years, presented with history of abrupt onset confusion and urinary incontinence 1.5 years ago lasting for a week. Subsequently, he was noted to have persistent cognitive deficits involving attention, executive dysfunction, and episodic memory. He was brought to our facility with an acute worsening of cognition for the last 2 months that was associated with increased libido and sexual disinhibition. His wife reported of drastic change in his sexual behavior with frequent demands of physical intimacy multiple times in a day and in inappropriate situations. He would become aggressive toward her when his needs were not met. On magnetic resonance imaging (MRI) brain, there was small vessel disease, diffuse atrophy, and subacute infarct in the right thalamic nucleus (Supplementary Fig S1, available in the online version only). Patient was diagnosed as Alzheimer's dementia with mixed etiology. During the in-patient care, assessment of ISB thar included previous sexual history and analysis of ISB behavior was done. In addition, there was an assessment about his physical and emotional needs in relation to ISB. Following the assessment, nonpharmacological approaches including strategies to improve communication, ensuring privacy, and engagement in other pleasurable activities were provided to patient. These resulted in a partial response in ISB. He was also started on tab. donepezil 10 mg OD for cognitive symptoms and tab. quetiapine 100 mg/day for intermittent physical aggression that also helped in decreasing ISB.
Case B
A 62-year-old married gentleman, right-handed, premorbidly well-adjusted, with a history of hypertension for the last 13 years, ischemic heart disease for the last 11 years, diabetes mellitus for the last 6 years, was brought to our facility. He had insidious onset and progressive cognitive decline for the last 2 years. The cognitive decline predominantly involved executive function and recent episodic memory which progressed to involve visuospatial impairment. He also had one episode of transient ischemic attack 3 years ago. Since 2 years, more so in the last 1 year, there was increased sexual desire with repeated demands on wife for sexual intimacy and he was procuring sildenafil to improve erectile function. On Hindi Mental Status Examination,6 he scored 21.1 During the evaluation, MRI brain was done and it revealed bilateral thalamic infarcts along with extensive small vessel disease of brain (Supplementary Fig S1, available in the online version only). He was diagnosed with vascular dementia. Psychosexual assessment of the couple was done. It was found apart from ISB, there were misconceptions about sex in the couple such as “physical intimacy in old age is inappropriate” and sexual interest declines naturally in late life. These misconceptions were clarified and communication improved on sexual needs in the couple. The patient was prescribed donepezil 10 mg OD for cognitive symptoms, besides metoprolol 50 mg OD, aspirin 75 mg OD, atorvastatin 10 mg OD, and metformin 1,000 mg twice daily, and vildagliptin 50 mg twice daily.
Case C
A 63-year-old female, married and retired employee, known case of diabetes and hypertension, was brought with a history of cerebrovascular stroke with left hemiparesis 7 years ago. She was able to work without any difficulty till she retired 3 years ago. Patient had another lacunar stroke 2 years ago. After the recent stroke 10 months ago, the patient presented with slurred speech and giddiness that improved after 1 month. Since 6 months, there was a change in her behavior characterized by loss of inhibition in terms of touching private parts of husband and close family members, repeatedly expressing the desire for physical intimacy with husband. These behaviors were not in keeping with her social norms and culture. In addition, there were mistakes while cooking, difficulties in making transactions at bank, impulsively snatching objects, craving for sweets, and unprovoked physical aggression. On evaluation, there was left facial weakness. Her investigations were unremarkable except for hyperglycemia. Her MRI brain revealed a chronic infarct in the right globus pallidus and left thalamus in the background of small vessel changes (Supplementary Fig S1, available in the online version only). Patient was diagnosed with vascular dementia. Psychosexual assessment of the couple was done and misconceptions were clarified; couple was provided psychoeducation about the ISB. Couple was encouraged in doing activities together (board games, evening walk, sharing emotions about each other). Patient was started on escitalopram 5 mg OD, aspirin 75 mg OD, atorvastatin 20 mg OD, amlodipine 5 mg OD, metformin 500 mg twice daily, glimepiride 1 mg twice daily.
Case D
A 93-year-old gentleman, with a history of hypertension, diabetes mellitus, and hypothyroidism, was brought by his son to our outpatient department for a subacute onset change in his personality and ISB of 4 months duration. Patient was found making inappropriate sexual gestures and advances toward house maids. He had attention and mild episodic memory deficits and episodes of intermittent irritability when confronted about his problematic behaviors. On clarification, there was an episode of transient ischemic attack 6 months ago. The computed tomography brain of patient revealed infarct in the left thalamus (Supplementary Fig S1, available in the online version only). The hypersexual behavior was managed with interventions including environmental modification, distraction techniques, and involvement in other activities. Patient was diagnosed with mild vascular cognitive impairment.
Discussion
The four cases that we have described were older adults, who presented with different types of ISB. The diagnosis was vascular dementia in two patients, one had mixed dementia (AD + VaD) and another had mild cognitive impairment. In addition, all patients had impairment in executive functions. There were three case studies that have reported on thalamic infarct and ISB (Table 1). In the case reported by Müller et al, there was involvement of ventral thalamus that presented as Klüver-Bucy syndrome.7 In the other two cases reported by Mutarelli et al, and Spinella, hypersomnia apart from ISB was reported that was not observed in our patients. In the Mutarelli et al's case, there was bilateral infarct in the paramedian thalamus and in another case by Spinella, there was infarct of the paramedian thalamus secondary to aneurysmal bleed.3 4 In the four cases we presented, three had left thalamic infarct and one had bilateral thalamic infarcts. We have conceptualized the role of thalamus in sexual behavior from the neuroanatomical and lesion-based studies on animal and nonhuman primates. Thalamus is a densely packed aggregation of multiple nuclei. Neuroanatomically thalamus is broadly divided by internal medullary lamina into medial and lateral group of nuclei. Positioned in the anterior and posterior part of thalamus are anterior nucleus and pulvinar nuclei, respectively. In addition, there are intralaminar and reticular nuclei. Closely associated with thalamus are medial and lateral geniculate nuclei. Among these thalamic nuclei, dorsomedial nuclei (DMN) are implicated in behavioral regulation and cognitive functions.
The DMN is the largest of the nuclear structures in the medial thalamus. The vascular supply to DMN is through paramedian branches of the basilar root of posterior cerebral artery. Phylogenetically DMN is most developed in primates, especially in humans. The development of DMN parallels that of prefrontal, association and cingulate cortices in humans. There are four subdivisions of DMN: a magnocellular (mc) subdivision, parvocellular (pc) subdivision, densocellular (dc), and pars multiforms (mf) which form specific connections with cortical and subcortical structures.8
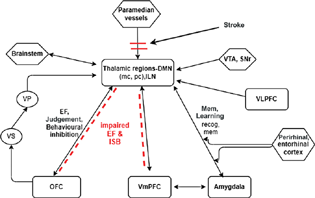
The major outputs of the DMN are to the medial and lateral PFC and OFC. The mc-PFC projections are almost exclusively reciprocal between the mc and the OFC and ventromedial PFC, but there is also a nonreciprocal input from ventrolateral PFC and medial PFC. This cortical–subcortical circuit is involved in attention, executive functions (planning, coordination, strategies, judgement), behavioral inhibition, and initiative. There are also reciprocal connections between the amygdala, hippocampal regions, and DMN.8 9 These circuits are involved in episodic memory, new learning, and recognition memory as shown in Fig. 1.
-
Fig. 1 Connection of the thalamus with prefrontal cortex: limbic, basal ganglia, and brain stem. DMN, dorsomedial nucleus; EF, executive function; ISB, inappropriate sexual behaviors; mc, magnocellular subdivision; OFC, orbital frontal; pc, parvocellular; SNr, substantia nigra; VLPFC, ventrolateral prefrontal cortex; VmPFC, ventromedial prefrontal cortex; VP, ventral pallidum; VS, ventral striatum; VTA, ventral tegmental area. Dotted line: circuit disruption.
Fig. 1 Connection of the thalamus with prefrontal cortex: limbic, basal ganglia, and brain stem. DMN, dorsomedial nucleus; EF, executive function; ISB, inappropriate sexual behaviors; mc, magnocellular subdivision; OFC, orbital frontal; pc, parvocellular; SNr, substantia nigra; VLPFC, ventrolateral prefrontal cortex; VmPFC, ventromedial prefrontal cortex; VP, ventral pallidum; VS, ventral striatum; VTA, ventral tegmental area. Dotted line: circuit disruption.
Given the extent of dense reciprocal connections between the DMN and PFC, any insult to thalamus will disrupt these corticosubcortial circuits. There is evidence from the perfusion imaging studies wherein it has been found that in patients with thalamic infarcts there was reduced perfusion in the bilateral PFC.3 Thus, a lesion in the DMN regions will decrease the input to the OFC, thereby reducing the behavioral inhibition and thus presenting as ISB.
The common constellation of symptoms in lesions of DMN includes cognitive symptoms: executive function impairment, episodic memory deficits, and new learning impairment. Behavioral manifestations include sexual misbehaviors, apathy, and confabulation.10 Other less common symptoms are hypersomnia, hyperphagia, preservation, hypophonia, and bilateral upper gaze palsy.10 In all the four cases we have described here, there was no change in sexual preference or any history suggestive of paraphilia. However, an increase in desire and inappropriate expression of sexual behavior that are suggestive of PFC dysfunction secondary to DMN lesion were observed. In the cases we have presented, the contribution of cognitive impairment to ISB cannot be ruled out.
In terms of management, the first step involves education of the caregivers/family members that helps in decreasing their apprehension, stigma, and improving communication. Other nonpharmacological interventions include promoting emotional intimacy between the couple, ensuring privacy through environmental modification, education of family members, distraction techniques, and involvement in activities. The pharmacological treatment needs to be considered in cases with severe ISB. Selective serotonin reuptake inhibitors, mood stabilizers, antipsychotics, and hormonal agents have been tried as treatment for ISB with variable response.11 As there are no randomized controlled studies in this field, treatment needs to be individualized depending on the patient profile and severity.
In older adults presenting with ISB, a thalamic lesion should be considered in the differential diagnosis. In addition to detailed history and clinical examination, neuroimaging should also be considered in these cases. This will help in avoiding inappropriate use of antipsychotics.
Conclusion
Thalamus plays a pivotal role in both cognitive processing and regulation of behaviors. There is a possibility that patients with thalamic infarcts presenting with behavioral manifestations could be erroneously diagnosed with primary psychiatric illness. Clinicians working with older adults need to consider thalamic lesions in their differential diagnosis in patients presenting with ISB and other frontal lobe features. There is merit in considering neuroimaging in these patients' investigative workups.
Conflict of Interest
None declared.
Funding None.
References
- Neuroanatomy and function of human sexual behavior: a neglected or unknown issue? Brain Behav. 2019;9(12):e01389.
- [Google Scholar]
- Neurological control of human sexual behaviour: insights from lesion studies. J Neurol Neurosurg Psychiatry. 2007;78(10):1042-1049.
- [Google Scholar]
- Hypersexuality following bilateral thalamic infarction: case report. Arq Neuropsiquiatr. 2006;64(1):146-148.
- [Google Scholar]
- Hypersexuality and dysexecutive syndrome after a thalamic infarct. Int J Neurosci. 2004;114(12):1581-1590.
- [Google Scholar]
- Thalamic circuits for independent control of prefrontal signal and noise. Nature. 2021;600:100-104. (7887):
- [Google Scholar]
- A Hindi version of the MMSE: the development of a cognitive screening instrument for a largely illiterate rural elderly population in India. Int J Geriatr Psychiatry. 1995;10(5):367-377.
- [Google Scholar]
- Persistent Klüver-Bucy syndrome after bilateral thalamic infarction. Neuropsychiatry Neuropsychol Behav Neurol. 1999;12(2):136-139.
- [Google Scholar]
- The anatomical and functional heterogeneity of the mediodorsal thalamus. Brain Sci. 2020;10(9):624.
- [Google Scholar]
- Treatment of inappropriate sexual behavior in dementia. Curr Treat Options Neurol. 2016;18(9):41.
- [Google Scholar]




