
Translate this page into:
Factors Influencing Institutional-Based Pediatric Rehabilitation Services among Caregivers of Children with Developmental Delay in Southwestern Rajasthan
Address for correspondence: Dr. Kriti Mishra, B-503, Sumadhur 2 Apartment, Behind Azaad Society, Ambawadi, Ahmedabad - 380 015, Gujarat, India. E-mail: kritimishra1@yahoo.co.in
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Context:
A limited number of caregivers of children with developmental delay access rehabilitation facilities in India. The study explored utilization of rehabilitation services at a tertiary care setup in southwestern Rajasthan and various factors influencing it.
Aims:
The aim of this study is to explore rehabilitation service utilization among children with developmental delay at a tertiary care setup and to ascertain factors that influence this pattern.
Settings:
This study was conducted at the department of physical medicine and rehabilitation at tertiary care setup.
Design:
This was an observational study.
Subjects and Methods:
Children with developmental delay who were advised institutional-based rehabilitation were identified over span of 1 year. Those who failed to return for rehabilitation after the first visit were interviewed telephonically. The interview had semi-structured open-ended questions about their reasons for inability to avail services.
Statistical Analysis:
SPSS statistics 22 was used for descriptive analysis and correlation of variables.
Results:
Of 230 children with developmental delay visiting department in 1-year duration, 48 took regular rehabilitation. Parents of 129 children with complete records were asked regarding discontinuation. Factors cited by majority were long distance from institute and service at hospital. Other reasons for discontinuation were related to belief system, family issues, time issues, socioeconomic factors, etc. Socioeconomic status was significantly associated with parental education (C = 0.488, P = 0.000) and financial issues. Location of family had significant association with long distance (C = 0.315, P = 0.000), parental education (C = 0.251, P = 0.003), and belief system (C = 0.265, P = 0.002).
Conclusions:
Distance from institute and quality of hospital service determined rehabilitation service use at a tertiary institute. Other factors such as socioeconomic status, family support, and social belief system must also be addressed while delivering institutional rehabilitation to children.
Keywords
Developmental delay
factor analysis
pediatric rehabilitation service

INTRODUCTION
It is estimated that 40–90 million children in India are differently abled, i.e., one in every tenth child has a physical, mental, or sensory disability.[1] Of these, developmental delay/disabilities form a major bulk with a global prevalence of 5%–15% among the pediatric population.[2] Developmental delay is defined as a condition when a child does not reach important developmental milestones within an expected period of time in 1 domain or more, i.e., gross/fine motor, language, and social domain.[2]
Institutional rehabilitative interventions are known to improve the physical and cognitive deficits and thereby enhance the functional outcome and level of independence in these children. The rehabilitation in these children is an ongoing process.[345] In spite of essential role of rehabilitation, only 2% of these people have accessibility to rehabilitation services in developing countries.[6] Hence, a systematic research regarding rehabilitation service utilization and barriers and facilitators for its usage is needed.
Only a few studies have explored these factors and lesser of them have determined what led to discontinuation of these services. Therefore, this study aimed to ascertain the factors that influenced caregiver's decision regarding continuation of institutional-based rehabilitation services for children with developmental disabilities.
SUBJECTS AND METHODS
The study was a descriptive analysis of data obtained from an ongoing study at a tertiary care setup concerning functional outcomes of children with developmental delay. Patients included were children between 0 and 18 years with no preference for sex and diagnosed as developmental delay. The data were obtained for 1-year duration. The rehabilitation service at the institute comprised of goal-directed therapy broadly consisting of consultancy, goal planning and therapy implementation by multidisciplinary rehabilitation team with recording of functional improvement during subsequent visits. Those caregivers who failed to report on regular basis/as advised by the rehab physician or therapist were contacted telephonically, and after obtaining informed consent, they were interviewed. The interview consisted of semi-structured and open-ended questions about reasons for not availing the service. A correlation analysis was done between factors as mentioned by the caregivers and their socioeconomic status, type of family, rural/urban background, and distance from the institute. Data analysis was done on IBM SPSS Statistics for Windows Version 22.0, Armonk, NY, IBM Corp. Released 2013. Frequency distribution was calculated for sociodemographic profile, and contingency coefficients were used to estimate relationship between reasons cited and demographic variables.
RESULTS
Total data set was of 230, out of which 48 children were reporting regularly for therapy. There was incomplete information for 53 children. Hence, the data set used for statistical analysis was of 129. Out of 129, there were 41 females and 88 males. Children from 11 months to 17 years reported for rehab and 1–1800 km distance range. Sixty-six families belonged to rural areas and 63 from urban areas. Maximum families belonged to middle class family (MCF) (n = 64) followed by lower MCF (n = 51). There were 10 families from upper MCF and 4 from lower class family (LCF). Eighty-six families were joint families. Forty-three were nuclear families.
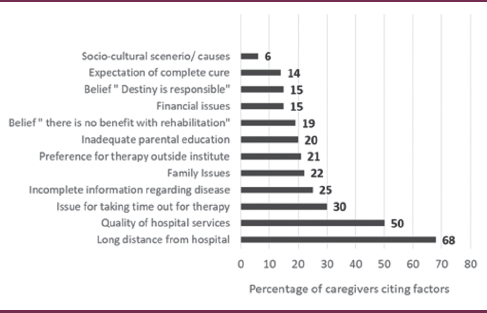
Eighty-eight families considered long distance responsible for one-time consultancy. Hospital services were considered as a factor by 64 families while 65 families did not consider it as a contributing factor. One hundred and two families did not prefer taking therapy outside and continued on home program as advised in the institute. Thirty-two families said that incomplete information about their child's health problem contributed to their decision of not taking regular therapy at hospital. Twenty-nine families had various family issues and 8 families stated sociocultural causes for not bringing their child for regular therapy. Twenty-six families were facing low parent education issue while 20 families reported monetary issues as a major contributor for discontinuation of therapy at hospital. Thirty-nine families had time-related issues. Nineteen families believed that there was no hope for their child since it is their destiny while 24 families believed that there was no benefit from therapy. Eighteen families expected complete cure, which was not achieved with rehabilitation. Further details are elaborated in Tables 1 and 2.

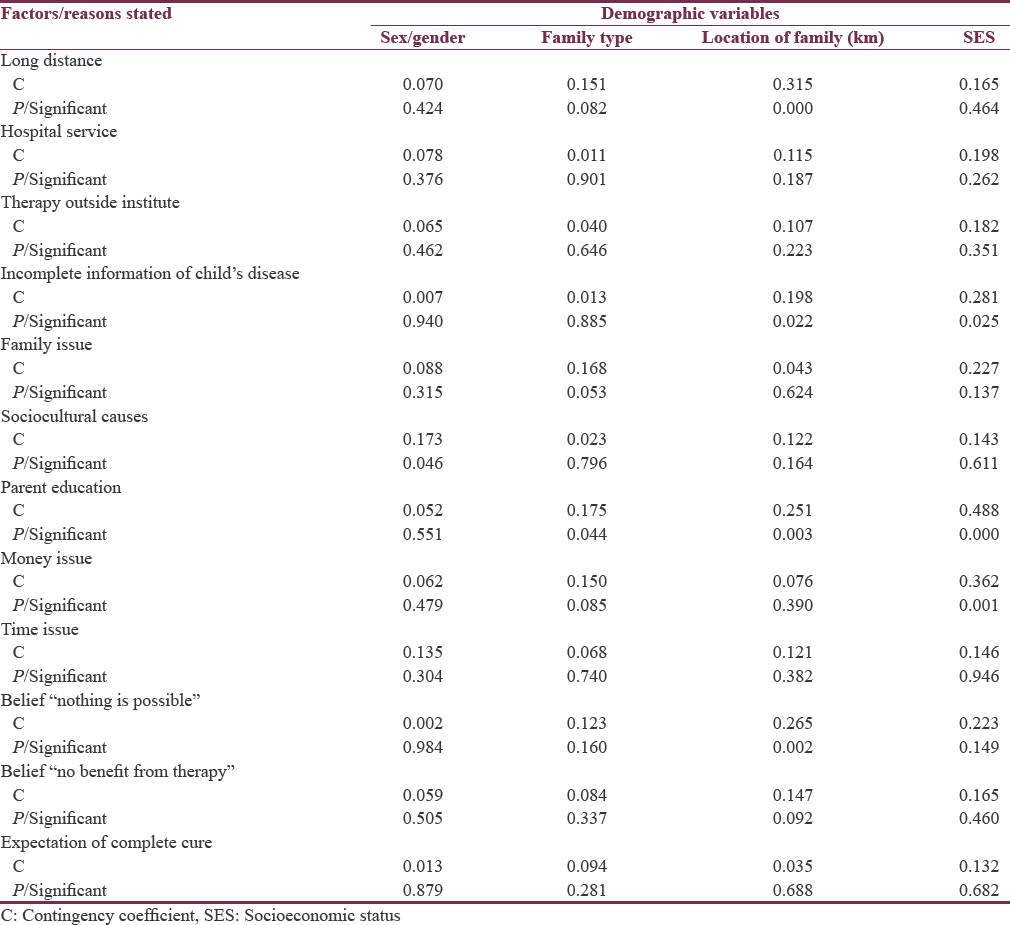
Data were not normally distributed (Shapiro-Wilk = 0.768, Sig. = 0.000). Association of twelve factors obtained with variables of sex, family type, socioeconomic status, and location (in kilometers) was calculated using contingency coefficients. Location of family showed significant association with factor of “long distance from institute” (C = 0.315, P = 0.000), inadequate parental education (C = 0.251, P = 0.003), and belief of “nothing is possible since it is child's destiny” (C = 0.265, P =0.002). A significant association was found between socioeconomic level and factors of inadequate parental education (C = 0.488, P = 0.000) and financial issues. Sex and type of family did not show any significant associations with any of the factors/reasons stated. Table 3 specifies further details.
DISCUSSION
An institutional-based rehabilitation setup caters to a wide spectrum of pediatric patients. Rehabilitative services for disabled children must address felt needs of the child and caregivers, and this requires multidisciplinary periodic assessments and interventions.[7] Thus, recurrent accessibility of rehabilitative services is essential. This, in turn, depends on multiple factors, namely, availability of service, physical accessibility to the institution, and affordability and acceptability of services by the local community.[8]
This study aimed to explore factors associated with nonutilization of rehabilitation services and perhaps one of the first studies to observe these factors in southwestern Rajasthan. Its uniqueness lies in the fact that unlike the previous studies done, the caregivers interviewed in the present study had an exposure of institutional rehabilitative service, and so, factors studied were reasons given by caregivers for not complying with rehabilitation at the institute.
Long distance was cited as the most common cause for not availing the service. Distance was noted to be a perception, i.e., caregivers who were residing as near as 4–5 km to the institute found distance far enough to avail the service. Hence, concept of “long distance” can be a prominent limitation in availing rehabilitation. This study also favors the findings of previous studies which suggested that the physical access to health service is a major hurdle for disabled people with disabilities to reach and utilize these services.[69]
Quality of health service is determined by structural elements (e.g., frequency, intensity, workforce, and facilities), processes of care (e.g., respectful and supportive care and treatment choices), and outcomes (e.g., functional gains and satisfaction with service).[710] Hence, the method of service delivery becomes essential. This became evident in the study as hospital service delivery method was the second most important factor for nonutilization. Nearly 50% of caregivers considered waiting process for services and communication gap from hospital staff as a major contributing factor. Moreover, deficiency of lodging in and near the hospital made it worse. Difficulty in comprehending information given at the institute regarding the condition also added to the nonutilization in 24%. This is similar to study by Laskar et al. where nonutility of government specialty rehabilitative services was due to long hours in queue (57%), ill-treatment by staff, especially those relying on aids and appliances, (45%) and complicated paperwork (36%).[11]
The present study showed that 81% caregivers understood importance of rehabilitation. Only 19% of families did not feel any benefit from therapy; 14% expected complete cure with no role of rehabilitation in cure, and only 15% believed destiny to be responsible for child's condition and hence no hope of change. Thus, majority of caregivers were aware of significance of rehabilitation for their child. This is in contrast to study by Borker et al. where poor utilization among disabled people of rural Goa was primarily attributed to lack of knowledge regarding rehabilitation in 77.9%.[8] An exposure to rehabilitation during their one-time hospital consultancy was probably responsible for better awareness among caregivers in the current study. It was noted that only 6% of these children were taking therapy outside and rest were continuing the same home program as explained to them at the institute. Some of the caregivers even mentioned improvement in child's physical abilities with the same home program.
Family or social issues such as death in family, elderly parents, other responsibilities of household, and job transfer (as mentioned by caregivers) affected utilization in 22% and 6% of families, respectively. This is in concordance with previous study by Borker et al. who found only 9% stating family issues as a cause for nonutilization.[8]
The current study also showed that 20% of parents had low education levels and hence had a poor understanding of the system, condition, and rehabilitative intervention. Padmamohan et al. also found poor education level of father as a determinant for service utilization in disabled rural children.[12] Patel and Ladusingh stated that treatment-seeking behavior of disabled persons would depend on socioeconomic factors, on cultural factors, area of residence, literacy status, gender, etc.[13] In the present study, though these factors have been mentioned, they only form a small percentage for discontinuation of rehabilitation.
Monetary concerns were mentioned as a cause by 15% in the current study. As this was a government institute, the facilities available were affordable. However, indirect expenses such as loss of daily wages/loss of daily business turnover/travel cost to the institute were high for a few of them. Nearly 30% had time-related issues due to family/work-related engagements and long waiting duration at the hospital. This is similar to study by Padhyegurjar and Padhyegurjar where lack of time, unaffordability, and belief of no requirement of rehabilitation formed a few reasons.[9] However, the percentage noted was as low as 2%–3% for these reasons and lack of knowledge formed the bulk. Furthermore, Borker et al. mentioned affordability followed by poor transport facility for nonutilization of service.[8] A recent study in Uttar Pradesh reported financial problem, lack of awareness, family negligence, and transportation problem as major barriers for neurological rehabilitation.[6] Although the current study did report these factors, but the lesser numbers suggest limited role played by these factors in the given region.
It has been found that in developing countries like India, socioeconomic status is closely linked to the type of service being availed. Middle classes generally preferred medical teaching institutes, lower classes availed from government setup, and high classes from private hospitals/clinics.[1415] A similar trend was seen in this study where the bulk of patients were from middle class or lower middle class, since this being a teaching institute.
An interesting finding was that though monetary issue was cited by limited caregivers, association estimation showed that socioeconomic status did become one of the determining factors for availing rehabilitation if parents had inadequate education and financial issues. Parents did prefer to avail services nearer to their homes or continue on the same home program as given at the institute. Time factor became an important contributor for them and the time spent in bringing their child for therapy was thought to be better utilized in their daily earnings/living. Since majority were from lower middle class, inadequate parental education and monetary issues were an obvious correlation. Both of these classes had lesser resources to share responsibility of family. Moreover, people with higher background and better education levels were more focused on acquiring this knowledge not just in the institute but also through other sources. Agrawal et al. similarly observed that better socioeconomic status is closely associated with greater utilization of health-care services among older persons as well.[16]
Another finding of the study was strong association of location with parental education, concept of long distance, and belief of no hope with blame on destiny for child's condition. The farther the family stayed from institute (more in suburban/villages), more was the ignorance, worse was parental education level leading to belief on destiny and no hope for child's condition.
It was noted that gender did not show a significant correlation with any of the factors cited suggesting that parents of children with disability irrespective of gender tend to avail rehab services if other factors are nullified. Previous study by Majnemer et al. have shown that gender did not emerge as strong correlate with receipt of these services.[7]
The present study had an equal number of rehab nonutilizers in rural and urban areas suggesting that these factors studied here play a role in both villages and cities alike.
It was found that majority were in residing in joint family highlighting significance of family members in the decision to seek service. However, family type did not show any strong association with any of the factors.
CONCLUSIONS
This study exposed the practical problems faced by parents with disabled children while accessing a tertiary care institute, suggesting a caregiver perspective. This was an attempt on the part of service providers to take a step beyond their regular duties of providing treatment and assessing what could be the possible backlogs of the current practice scenario so that the gap between the provider and receiver is bridged. Quantification of problem in actual settings and addressing them can help create a friendly environment and encourage caregivers to utilize services frequently. This would also lead to formulation of rehabilitation protocols with a practical utility for these children, than a theoretical application of rehabilitation goals. This would, in turn, help in improving the acceptability, accessibility, and utility of institutional-based rehabilitation in a given community, since a rehabilitation program formulated keeping these factors into consideration, could be more realistic and acceptable for caregivers. Studies focusing on written feedbacks from patients visiting outpatient department the first time or those coming to hospital on regular basis can further strengthen findings of the present study and may influence the decisions of policymakers and health-care staff for a better patient service delivery model.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We thank caregivers and parents of children with developmental delay who had visited our department earlier and agreed to give their valuable time and contributed by participating in the study for a telephonic interview.
REFERENCES
- Discrimination against differently abled children among rural communities in India: Need for action. J Nat Sci Biol Med. 2015;6:7-11.
- [Google Scholar]
- Practice parameter: Evaluation of the child with global developmental delay: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2003;60:367-80.
- [Google Scholar]
- Youth and young adults with cerebral palsy: Their use of physician and hospital services. Arch Phys Med Rehabil. 2007;88:696-702.
- [Google Scholar]
- Use of health care among adults with chronic and complex physical disabilities of childhood. Disabil Rehabil. 2005;27:1455-60.
- [Google Scholar]
- Awareness and utilization of rehabilitation services among physically disabled people of rural population of a district of Uttar Pradesh, India. Int J Med Sci Public Health. 2014;3:1157-60.
- [Google Scholar]
- Rehabilitation service utilization in children and youth with cerebral palsy. Child Care Health Dev. 2014;40:275-82.
- [Google Scholar]
- Study of knowledge, accessibility and utilization of the existing rehabilitation services by disabled in a rural Goan community. Ann Trop Med Public Health. 2012;5:581-6.
- [Google Scholar]
- Factors affecting treatment seeking behaviour of individuals with locomotor disabilities. Natl J Med Res. 2012;2:145-8.
- [Google Scholar]
- Psychosocial effect and economic burden on parents of children with locomotor disability. Indian J Pediatr. 2010;77:529-33.
- [Google Scholar]
- Utilization of rehabilitation services by rural households with disabled preschool children. Indian Pediatr. 2009;46:S79-82.
- [Google Scholar]
- Age Pattern of Onset of Disability and Treatment Seeking Behaviour of Disabled Persons in India. 2012. Available from: http://www.iussp2009.princeton.edu/download.aspx?submissionId=91173
- [Google Scholar]
- Factors influencing utilization of physiotherapy service among children with cerebral palsy in Jalandhar district of Punjab. J Neurosci Rural Pract. 2017;8:209-15.
- [Google Scholar]
- A study on the awareness, beliefs, and service utilization among families of children with cerebral palsy in Jalandhar District of Punjab. CHRISMED J Health Res. 2014;1:170-5.
- [Google Scholar]
- Aging, disability and health care services among older persons in India. Middle East J Age Ageing. 2009;6:21-8.
- [Google Scholar]




