
Translate this page into:
Epidural steroid injection in patients with lumbosacral radiculopathy in Abuja, Nigeria
Address for correspondence: Dr. Ahidjo A Kawu, Department of Orthopaedics, Spine Unit, University of Abuja Teaching Hospital, Gwagwalada, PMB 228, Abuja FCT, Nigeria. E-mail: ahidjokawu@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objective:
This prospective-controlled observational study looked at well-matched patients with spinal pain and radicular symptoms, caused by lumbar intervertebral disc herniation to compare the short-term clinical outcome of transforaminal and interlaminar epidural steroid injection (ESI) in a resource challenged tertiary institution in Nigeria.
Materials and Methods:
49 patients with radicular symptoms who were matched for age, symptom duration, magnetic resonance imaging findings, and pre-injection revised Oswentry Disability Index (ODI) score and Visual Analogue Scale (VAS) were assigned into ESI technique. The ODI and VAS score were analyzed immediately after an injection and upon follow-up (average 178.5 days), also with the need for repeated injections and surgical interventions over a 1-year follow-up interval.
Result:
In the transforaminal group (25 patients), there was a statistically significant improvement in the ODI scores from before the injection (ODI mean 62.4) to immediately after the injection (ODI mean 24.4, P < 0.01), and upon follow-up (ODI mean 20.8, P < 0.01). 9 patients (18.4%) required 1 or 2 repeated injections, 3 (6.1%) patients underwent surgery and 2 (4%) patients lost to follow-up. In the interlaminar group (24 patients), there was a statistically significant improvement in the ODI scores from before the injection (ODI mean 60.7) to immediately after the injection (ODI mean 30.1, P < 0.01), but not upon follow-up (ODI mean 43.2, P = 0.09). 11 (22.4%) patients required 1 or 2 repeated injection, 4 (8%) patients underwent surgery and 3 (6.1%) patients were lost to follow-up. There is an average of 2 fold improvement of transforaminal ESI over interlaminar ESI in a 40 point scale of ODI score on follow-up, which was statistically significant (P < 0.01). The VAS showed similar pattern with the ODI scores in the study.
Conclusion:
Transforaminal ESI to treat symptomatic lumbar disc herniation resulted in better short-term pain improvement and fewer long-term surgical interventions compared to interlaminar ESI.
Keywords
Epidural injections
oswentry disability index
spinal pain

Introduction
Spinal pain is the most common of all chronic pain disorders.[1–5] There are factors that have been implicated in the genesis of back pain and disability that can be used to determine whether a pathological process seen on imaging studies is associated with symptoms experienced by a patient.[1–4] Certain of these factors are based on epidemiological studies while others are based on clinical findings and physiological tests.[4] The lifetime prevalence of spinal pain has been reported as 54% to 80%.[5–8] Annual prevalence of chronic low back pain ranges from 15% to 45%.[5–8]
Intervertebral disc herniation is a commonest cause of lumbosacral radiculopathy. Many interventions have been employed in the treatment of chronic low back pain from lumbosacral radiculopathy. These interventions have been non-surgical[9–13] and surgical. Though a large proportion of these patients recover with non-surgical treatment, 10% - 15% of patients will require surgical care.[14] There are not any interventions which have provided definite and long-term improvement in chronic low back pain, neither conservative nor surgical.[15–17] Epidural steroid injections (ESIs) have been used for decades for the treatment of spinal pain, particularly for radicular symptoms and radiculopathy.[18] The goal of this treatment is to reduce pain, improve functions and to reduce surgical intervention.[5918] Many studies[19–23] have demonstrated the efficacy and methods of ESI. These studies have not been conclusive on the overall benefit over long-term and its cost-effectiveness.
ESI is one of the established treatment options in the management of spinal pain in few centers in Nigeria with no outcome study in the literature. ESI is performed with an aid of a portable mobile X-ray in our institution because of the non-availability of a fluoroscopy machine. The hypothesis of this study is that ESI would improve radicular symptom and that transforaminal ESI provides better outcome compare to interlaminar ESI.
This prospective-controlled observational study looked at patients with spinal pain and with radicular symptoms, caused by lumbar intervertebral disc herniation to compare the short-term clinical outcome of transforaminal to interlaminar epidural steroid injection in a resource challenged tertiary institution in Nigeria.
Materials and Methods
This study prospectively looks at 49 patients with low back pain treated with ESI at the University of Abuja Teaching Hospital, Gwagwalada Nigeria, from 1st January 2009 to 1st June 2010. The following were the inclusion criteria of the patients for the study:
-
Patients with magnetic resonance imaging (MRI) films.
-
Low back pain with uni or bilateral radicular pain, caused by a lumbar intervertebral disc herniation of not more than 1-year duration.
-
Single level disc herniation on recent MRI corresponding to the patients clinical symptoms.
-
Failure to respond to non-invasive treatment.
The exclusion criteria were:
-
Known contraindications to ESI
-
Previous lumbar ESI
-
Previous lumbar spine surgery
-
Patients who decline to participate in the study.
These patients were examined and their image studies reviewed and assigned into 2 treatment group; transforaminal and interlaminar groups after an informed consent duly filled that described the study including the risks and benefits. Alternate patient was assigned into each treatment group. The patients were not blinded to the treatment protocol. At the time of the procedures, the author had no personal preference for either transforaminal or the interlaminar technique of ESI, and all injections using either technique were performed at or below the level of disc herniation.
A mobile X-ray was used for the procedures due to lack of fluoroscopy facility in our center at the time of this study. The transforaminal and interlaminar approach employed was as described by Schaufele et al.[18] For the transforaminal approach, a 25 or 22-gauge, 3½-inch or 5-inch spinal needle was used. The needle was placed in the superior and anterior aspect of the corresponding neuroforamen under frequent mobile X-ray guidance, using the described standard technique.[24] After the needle was determined radiographically to be in the appropriate position, a combination of 80 mg of methylprednisolone acetate with 4 ml of marcaine 0.5% was injected.
For the interlaminar epidural steroid injections, the modified traditional midline approach was used. A 18-gauge, 3½-inch or 5-inch Tuohy needle was advanced into the posterolateral epidural space of the affected leg with radicular symptoms, using the loss-of-resistance technique. After negative aspiration for cerebrospinal fluid, a combination of 80 mg of methylprednisolone acetate with 4 ml of marcaine 0.5% was injected in the epidural space.
Prior to the procedure, the patients were rated using the revised Oswentry Disability Index (ODI) and Visual Analogue Scale (VAS) by the resident doctor in the unit. This was also rated immediately after the procedure and at 6 months of review by independent personnel, not involved in the ESI procedure. Using the ODI (scale, 0 to 100), 10 to 20 points is considered moderate, < 10 is small while > 20 is considered substantial. The mean improvements of 5 to 10 points on a 100-point visual analogue pain scale is considered small or slight, 10 to 20 points is considered moderate and > 20 points is considered large or substantial.
Using statistical package for social science (SPSS) 17.0 (SPSS Inc. Chicago Illinois, USA), a paired, two tail t-test was used to determine a statistical difference for pre-injection, post-injection and follow-up between the interlaminar and transforaminal groups. A P-value of < 0.05 is significant.
Results
56 patients satisfied the inclusion criteria, 49 patients (87.5%) consented to the trial and 5 patients (10.2%) were lost to follow-up. The patients’ characteristics are as shown in Table 1. In the transforaminal group, there was a total of 25 (51.0%) patients with mean age 46.9 ± 10.7 (range 36 - 67 years) while in the interlaminar group, 24 (44.4%) patients with mean age was 48.3 ± 11.3 (range 33 - 69 years). There was no statistically significant difference in the mean age in either group (P = 0.10). The mean pre-injection duration of symptoms in transforaminal and interlaminar group was 7.8 months and 8.1 months, respectively, and there was no significant statistical difference in the duration of symptoms in either group. This shows that the patients in both groups were matched.
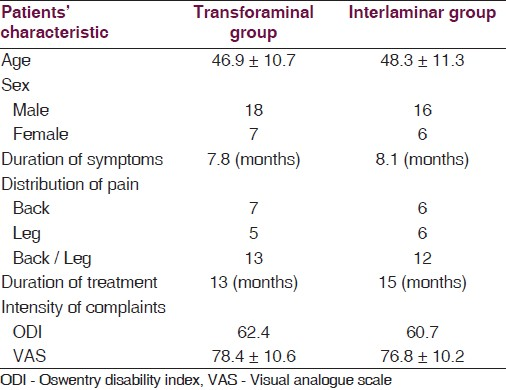
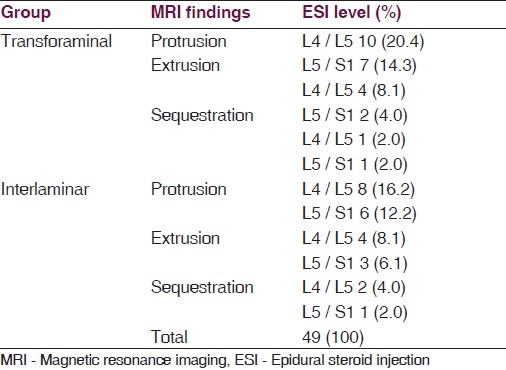
Table 2 shows the summary of MRI findings and the ESI levels of the subjects. The MRI reports were from different radiologists who were not directly involved in this study. There was no attempt to measure the size of herniation. The findings were similar between the 2 groups with disc protrusion predominating (65.3%). Majority (59.2%) of ESI were at the L4 / L5 level. Also, in terms of disease pathology and level of ESI, the patients in each group were well-matched.
The mean ODI and VAS scores at pre-injection, immediate post-injection and at 6 months were shown in Tables 3 and 4, respectively, for the 2 groups. The pre-injection ODI and VAS scores were similar in both the groups.
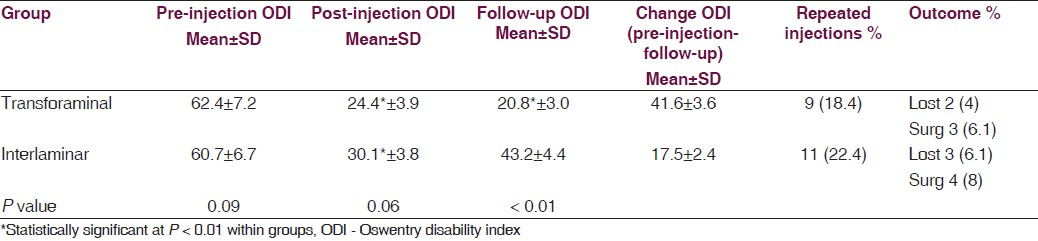

In the transforaminal group, there was an improvement in the ODI and VAS score from the pre-injection to the immediate post-injection state. This improvement was statistically significant (P < 0.01). Improvement in ODI and VAS scores were sustained upon follow-up, which was statistically significant (P < 0.01). In this group, 9 (18.4%) patients required 2 or more repeated injections, 2 (4%) patients were lost to follow-up, and 3 (6.1%) patients underwent surgery.
There was a statistically significant improvement in the ODI and VAS scores in the interlaminar group from the pre-injection to immediate post-injection review (P < 0.01). This improvement was sustained upon follow-up which was, however, not statistically significant. 3 (6.1%) of the patients in this group were lost to follow-up while 4 (8%) patient underwent surgery.
Unlike in the immediate post-injection review between the 2 groups where improvement did not show any significant difference, follow-up at 6 months improvement was statistically significant (P < 0.01). The transforaminal group showed an improvement in symptoms on ODI score over the interlaminar group at 6 months follow-up [Table 4]. The VAS score changes were better with transforaminal ESI compared to the interlaminar ESI. This also showed a significant difference at 6 months.
An average improvement noted in the transforaminal group and interlaminar group was 41.6 and 17.5 points of the ODI scores, respectively. This represents more than 2 folds improvement in the transforaminal group compared to the interlaminar group. 18 (72%) patients had an average improvement of 40 points or more on the ODI scale in the transforaminal group, compared to 6 (25%) patients in the interlaminar group. An average ODI improvement at 6 months follow-up was noted in 14 (56%) patients and 6 (25%) patients in the transforaminal and interlaminar group, respectively.
The VAS score showed more than 20 point change in both group of patients which, however, is a substantial improvement from pre-injection state.
Discussion
This study patterned, after the study done by Schaufele et al,[18] was to compare the short-term clinical outcome of transforaminal to interlaminar epidural steroid injection in a resource challenged country like Nigeria. The major drawback was that portable mobile X-ray was employed in this study against the current published guideline[1820] on the importance of fluoroscopic guidance. Nigeria is a developing country with peculiar socio-economic maladies where healthcare facilities are grossly inadequate and can only serve 5% - 10% of their potential patient load.[25]
There was no significant difference in the pre-injection age of the patients, symptom duration, MRI findings [Table 1], ODI and VAS scores and level of ESI [Table 1]; hence, the 2 groups of patients were well-matched.
Unlike in the findings by Schaufele et al,[18] this study showed that the transforaminal group on an average felt significantly better immediately after the procedure, compared to the interlaminar group. This group had significant improvement of ODI and VAS scores directly after an injection, which was largely maintained at follow-up. This author also agrees with others[1820] that the more targeted delivery of the injectate along the inflamed spinal nerve is the most likely explanation for these better outcomes [Table 4].
Schaufele el al[18] and Riew et al[21] noted that transforaminal ESI decreases the need for discectomies for lumbar disc herniations. This was also noted in this study where the surgery rate was 6.1%. This rate is lower than the rate, previously reported on (10% - 29%).[1821] This may be due to the well-matched patients in all the parameters for inclusion criteria.
Interestingly, the outcome measure employed in this study showed comparable findings to that in most of the studies[131519] reviewed. This supports the validity of this study. Schaufele et al[18] and Vad et al[20] reported 84% and 70% “success” in patients with lumbosacral radiculopathy who underwent transforaminal ESI, respectively. This supported the finding in this study that noted 72% success in the treatment, employing transforaminal ESI. In the interlaminar ESI, studies[1826] reviewed shows effective treatment between 42% - 56%. This is higher than that noted in our study. The only explanation may be the use of mobile X-ray without a concordant contrast studies use, affecting an appropriate localization of needle and reducing the quantity of injectate to the desire target.
Also, noted in this study was the high number of patients lost to follow-up (10.2%). This is the peculiarity of healthcare delivery system in the developing country like Nigeria, where patients move from one facility to the others without completing informed treatment options.
The study was limited as also documented by Schaufele et al[18] by the sample size, non-randomized control trial, short follow-up, and bias that may have been introduced by all the procedure being performed by the same physician.
This study addressed the short-term clinical outcome of transforaminal and interlaminar epidural steroid injection in a resource-challenged tertiary institution in Nigeria. Efforts should be made to promote the usefulness of this treatment option in the developing country like Nigeria where there are few specialists[27] that operate on the spine.
Source of Support: Nil
Conflict of Interest: None declared.
References
- The epidemiology of spinal disorders. In: Frymoyer JW, ed. The Adult Spine, Principles and Practice (2nd ed). Philadelphia: Lippincott-Raven; 1997. p. :32-78.
- [Google Scholar]
- The prevalence of low back pain among children and adolescents.A nationwide, cohort-based questionnaire survey in Finland. Spine. 1997;22:1132-6.
- [Google Scholar]
- An atlas of back pain. New York: The Parthenon Publishing Group; 2002. p. :8-93.
- Epidural steroids in the management of chronic spinal pain: A systematic review. Pain Physician. 2007;10:185-212.
- [Google Scholar]
- Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum. 1998;41:778-99.
- [Google Scholar]
- The Saskatchewan health and back pain survey: The prevalence of low back pain and related disability in Saskatchewan adults. Spine. 1998;23:1860-7.
- [Google Scholar]
- The prevalence of low back pain in the elderly. A systemic review of the literature. Spine. 1999;24:1813-9.
- [Google Scholar]
- Prognosis in sciatica: A clinical follow-up of surgical and non-surgical treatment. Acta Orthop Scand Suppl. 1970;12:129-36.
- [Google Scholar]
- Nonoperative treatment of herniated lumbar Intervertebral disc with radiculopathy: An outcome study. Spine. 1989;14:431-7.
- [Google Scholar]
- The natural history of lumbar Intervertebral disc extrusions treated nonoperatively. Spine. 1990;15:683-6.
- [Google Scholar]
- Lumbar disc herniation: A controlled prospective study with ten years of observation. Spine. 1983;8:131-40.
- [Google Scholar]
- The natural history of sciatica with associated disc pathology: A prospective study with clinical and independent radiologic follow-up. Spine. 1992;17:1205-12.
- [Google Scholar]
- Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain. Cochrane Database Syst Rev. 2005;3:CD003008.
- [Google Scholar]
- A Cochrane review of superficial heat or cold for low back pain. Spine. 2006;31:998-1006.
- [Google Scholar]
- Traction for low-back pain with or without sciatica. Cochrane Database Syst Rev. 2005;4:CD003010.
- [Google Scholar]
- Interlaminar versus transforaminal epidural injections for the treatment of symptomatic lumbar intervertebral disc herniations. Pain Physicians. 2006;9:361-6.
- [Google Scholar]
- A multicentre randomized controlled trial of epidural corticosteroid injections for sciatica: The WEST study. Rheumatology (Oxford). 2005;44:1399-406.
- [Google Scholar]
- Transforaminal epidural steroid injections in lumbosacral radiculopathy: A prospective randomized study. Spine. 2002;27:11-6.
- [Google Scholar]
- The effect of nerveroot injections on the need for operative treatment of lumbar radicular pain.A prospective, randomized, controlled, double-blind study. J Bone Joint Surg Am. 2000;82-A:1589-93.
- [Google Scholar]
- The efficacy of corticosteroids in periradicular infiltration for chronic radicular pain: A randomized, double-blind, controlled trial. Spine. 2005;30:857-62.
- [Google Scholar]
- Lumbar transforaminal injection of corticosteroids. In: Practice guidelines for spinal diagnostic and treatment procedures. San Francisco, Calif: International Spine Intervention Society; 2004. p. :163-18.
- [Google Scholar]
- No wealth, no health. Available from: http://www.thisdaylive.com/articles/no-health-no-wealth-1-/95993/
- [Google Scholar]
- Treatment of lumbar disc herniation: Epidural steroid injection compared with discectomy. A prospective, randomized study. J Bone Joint Surg Am. 2004;86-A:670-9.
- [Google Scholar]
- Spine surgery practice in Nigeria: Present perceptions and future trends. Nig J Ortho Trauma. 2010;9:8-9.
- [Google Scholar]




