
Translate this page into:
Endovascular Management of Intracranial Pial Arteriovenous Fistulas: Experience of Largest Series at a Single Center Over Six Years
Address for correspondence: Dr. Luis Rafael Moscote-Salazar, RED LATINO Latin American Trauma and Intensive Neuro-Care Organization, Bogota, Colombia. E-mail: mineurocirujano@aol.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Intracranial pial fistulas are an extremely uncommon type of vascular pathology consisting of one or multiple arterial connections to a single venous drainage channel without the presence of an intervening nidus. Due to its typical location and high-flow dynamics, its management is difficult and options include endovascular treatment and open surgical treatment. The arterial supply of these lesions is usually derived from pial or cortical vessels, and commonly such lesions are not localized in the dura mater.
Materials and Methods:
Authors report the experience of consecutive ten cases managed at the Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez” of México extending from 2007 to 2012 with endovascular technique, constituting one of the largest series in the Western literature.
Discussion:
Pial fistulas are associated with a poor natural history, and the selection of individualized therapeutic strategies can provide good outcomes.
Conclusion:
The neuroendovascular intervention is currently considered as safe, low cost, and effective management modality for such lesions.
Keywords
Endovascular management
intracranial
outcome
pial arteriovenous fistula

INTRODUCTION
Pial arteriovenous fistulas (AVFs) are extremely uncommon intracranial vascular lesions. The pial AVFs represent only 1.6%–4.7% of all neurovascular malformations.[1] In the past, pial AVF was once regarded as a type of arteriovenous malformation (AVM). However, current evidence suggests that pathological characteristics and clinical presentations and therapeutic options are different from those of AVM. These were previously categorized as AVFs; however, available evidences suggest that these are special entity which require different therapeutic approach for management. Authors present a case series, who were managed in the Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez” of México constituting the largest case series reported to date. Pial AVF may have single or multiple arterial connections to single venous drainage channel without any intervening nidus. Pial AVF differs from dural AVF in that the arterial supply is derived from pial or cortical arterial vessel and the location is not within the dural leaflets.[2] Due to high-flow dynamics, pial AVF is often associated with a venous varix.[2]
METHODS
A review of the clinical files of the National Institute of Neurology and Neurosurgery was the year 2007 until 2012 with a diagnosis of pial AVF. Medical records were carefully evaluated to determine the functional prognosis of the patients before treatment and in the late follow-up [Table 1].
CASE SERIES (CASE 5)
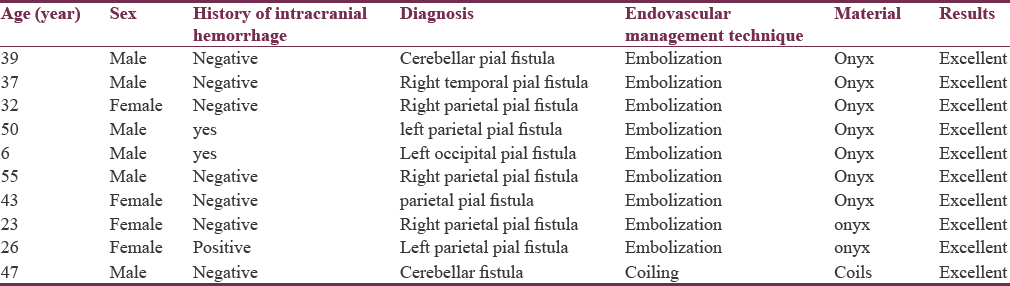
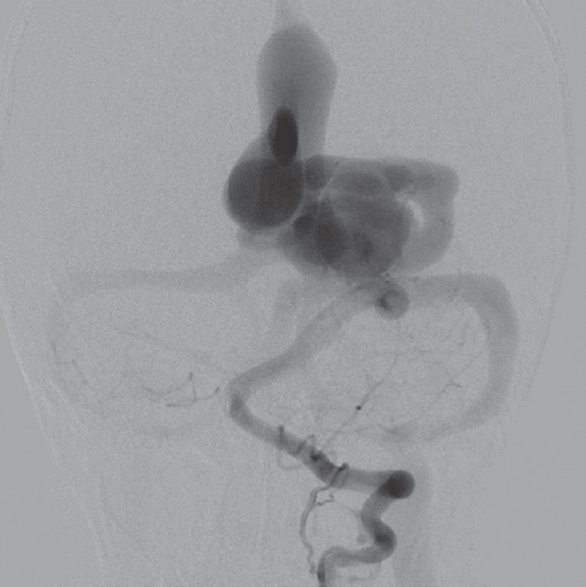
A 6-year-old male patient presented with a history of sudden loss of consciousness. The general examination and neurological examination were within normal limit at admission. A cranial computed scan was carried out to evaluate the causes of unconsciousness which revealed the presence of parietal hematoma; a cerebral angiography revealed evidence of an arteriovenous communication between posterior cerebral artery and distal anterior cerebral artery that drained to the sagittal sinus [Figure 1]. Based on angiography findings, the plan was decided to perform embolization with Onyx™ under general anesthesia, the posterior cerebral angiography showed the complete occlusion of the fistula [Figure 2a and b], and the postoperatory was satisfactory. At 12-month follow-up, the patient was asymptomatic.
- A cerebral angiography revealed evidence of an arteriovenous communication between posterior cerebral artery and distal anterior cerebral artery that drained to the sagittal sinus
- (a and b) A control cerebral angiography showed the complete occlusion of the fistula
DISCUSSION
The pial AVF is considered as rare cerebrovascular lesion and considered as variant of AVM for decades. However, newer studies showed that pial AVF is a distinct especial entity different from cerebral AVM, dural intracranial AVF, or other cerebral vascular lesions due to the different angiographic architecture, clinical course, and management options for pial AVF.[34]
The pathophysiological abnormality in pial AVF is related to high-flow nature of fistula. The communication between arterial feeder drains directly into a solitary draining vein without an intervening tangle of vessels called nidus and associated venous varices are related to the high turbulent flow from arteriovenous shunting.[56]
Due to lack of nidus, the existing higher pressure gradient, which can make such lesions more prone for rupture, leading to relatively worse prognosis.[7] It has been reported the case of a pial AVM with dural substitution associated with dural venous sinus thrombosis. The pial fistulas that occur in the 1st years of life may be associated with disease syndromes such Rendu-Osler-Weber and Klippel-Trenaunay-Weber syndromes. To our knowledge, this is the largest pial fistulas cases series reported.
Due to their rarity, the natural history of intracranial pial AVF is still not well understood. In case of untreated pial fistula, the conservatively managed pial AVF and associated high mortality: five (63%) of eight patients died due to acute or subsequent fatal bleeding, so pial AVF requires surgical or endovascular treatment.[8]
The pial fistulas may present as bleeding, seizures, neurological deficits, cardiac failure in neonates and infants, headache and symptoms of increased intracranial pressure in children and may also present as palpable masses, erosion in the skull, and macrocephaly. The pial fistulas can also present with hemorrhage, headache, high-output cardiac failure in neonates and infants, macrocephaly, and features of raised intracranial pressure.[19]
Management of pial AVF differs from that of AVM and disconnection of the arteriovenous communication could eliminate the abnormality eliminating the need of resection. Fistulas in pediatric patients are associated with varicose veins in a high percentage; in these cases, the patient may experience mass effect symptoms; in adult patients, the symptoms are more frequently associated with hemorrhages. Regard therapeutic strategies, the endovascular management studies had showed obliteration rates of 86.5% and the surgical treatment offers similar rates, 86.8%.
In contrast, in AVM, resection of the entire lesion is necessary because of the multiplicity of the communicating shunts and occluding only the feeding arteries leaves behind the nidus, which can cause further recruitment of newer arterial feeders and the draining veins must also need to be obliterated because they persist after resection and may recruit recommunication with collaterals. The pathological features of a congenital pial AVF arise principally from its high-flow nature. Treatment of pial AVF by simply cutting off the shunt connection through surgery or endovascular intervention is sufficient, with removal of the entire vascular malformation was unnecessary.[1011]
Disconnection of the high-flow system leads to elimination of the abnormality and also the venous varices.
Management including the disconnection of the AVF was traditionally accomplished surgically by either clip application or cauterization of the vessel with proven effective. However, some lesions may be in deeply located or surgically inaccessible locations and as such surgery was associated with high risk. Recently, endovascular applications have been reported as successful means of disconnecting AVF with a variety of different agents such as balloons, coils, glue, silk sutures, or polyvinyl alcohol.[912]
Accessing the lesion through an endovascular technique eliminates the risks associated with surgical craniotomy and surgical-dissection approach. However, endovascular methods are not always successful or safe and many times may be unsuitable or develop postprocedural complications are well known. High-flow fistula makes it difficult to deliver the desired embolic agent precisely to the fistulous point. Delivery of embolic material into the draining vein can compromise venous outflow of the fistula or cause pulmonary embolism-like complications. Similarly, compromised venous outflow in the setting of an incompletely obliterated fistula can have disastrous consequences.[891314] As endovascular technologies continue to rapidly advance, we expect higher pial AVF detection rates, as well as higher success rates with endovascular flow disconnection of arteriovenous shunting.[314151617]
CONCLUSION
Pial AVFs are rare intracranial vascular malformations, and due to poorly understood natural course and associated significant morbidity, early prompt diagnosis and appropriate management are very important and highly desired. Early decision of endovascular therapy can lead to good neurological outcome and avoid or eliminate the risk of pial diurnal AVF-related complications. The goal of treatment is to remove the pial fistulas of high flow, to be disposed parallel disappear aneurysms and varicose veins. The aim is to close the fistula with obliteration of the vessels that feed the lesion and preserving venous drainage. Total resection of the lesion is unnecessary.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Endovascular treatment of brain arteriovenous fistulas. AJNR Am J Neuroradiol. 2009;30:851-6.
- [Google Scholar]
- Onyx embolization of intracranial pial arteriovenous fistula. J Cerebrovasc Endovasc Neurosurg. 2016;18:291-5.
- [Google Scholar]
- Balloon-assisted onyx embolization of cerebral single-channel pial arteriovenous fistulas. J Neurosurg Pediatr. 2011;7:637-42.
- [Google Scholar]
- Angiographic architecture of intracranial vascular malformations and fistulas – Pretherapeutic aspects. Neurosurg Rev. 1986;9:253-63.
- [Google Scholar]
- Intracranial arteriovenous fistula manifesting as progressive neurological deterioration in an infant: Case report. Neurosurgery. 1991;28:619-22.
- [Google Scholar]
- Interdisciplinary evaluation of cerebral hemodynamics in the treatment of arteriovenous fistulae associated with giant varices. Neurosurgery. 1994;35:778-82.
- [Google Scholar]
- Intracranial pial arteriovenous fistulae: Diagnosis and treatment techniques in pediatric patients with review of literature. J Clin Imaging Sci. 2016;6:2.
- [Google Scholar]
- Endovascular embolization of congenital intracranial pial arteriovenous fistulas. Neuroimaging Clin N Am. 1992;2:309-17.
- [Google Scholar]
- Giant intracranial varices secondary to high-flow arteriovenous fistulae. J Neurosurg. 1987;66:198-203.
- [Google Scholar]
- Surgical and endovascular flow disconnection of intracranial pial single-channel arteriovenous fistulae. Neurosurgery. 2001;49:1351-63.
- [Google Scholar]
- Posterior cranial fossa single-hole arteriovenous fistulae in children: 14 consecutive cases. Neuroradiology. 2004;46:474-81.
- [Google Scholar]
- Intracranial pial arteriovenous fistulas with single-vein drainage. Report of three cases and review of the literature. J Neurosurg. 2004;100:201-5.
- [Google Scholar]
- Supratentorial cerebral arteriovenous fistulas (AVFs) in children: Review of 41 cases with 63 non choroidal single-hole AVFs. Acta Neurochir (Wien). 2005;147:17-31.
- [Google Scholar]
- Vascular malformations of the brain in hereditary hemorrhagic telangiectasia (Rendu-osler-weber disease) Surg Neurol. 1994;41:374-80.
- [Google Scholar]
- Surgical treatment of pial cerebellar arteriovenous fistulas with aneurysm of the main feeding artery. Surg Neurol. 2006;65:90-4.
- [Google Scholar]
- Pial arteriovenous fistulas: Dilemmas in prenatal diagnosis, counseling and postnatal treatment. Report of three cases. Ultrasound Obstet Gynecol. 2005;26:293-6.
- [Google Scholar]




