
Translate this page into:
Cerebral Hydatid Cyst in a Young Immunocompromised Patient in Parakou
Address for correspondence: Dr. Thierry Adoukonou, Department of Neurology, University of Parakou, Parakou, Benin. E-mail: adoukonouthierry@yahoo.fr
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
We report the case of a 30-year-old human immunodeficiency virus (HIV)-positive HIV patient who was poorly followed. She was admitted on November 30, 2017, for the management of febrile encephalitis syndrome with motor deficit of the left hemicorps and generalized seizures. In biology, we found a nonspecific inflammatory syndrome. The cerebral imaging without and with injection found a cystic formation multilobed right fronto-parietal of approximately 83 mm × 62 mm, the presence of an annular calcification of approximately 8 mm with a commitment under falcator, and a contralateral ventricle dilation. Treatment with antiepileptic, antibiotic, antiparasitic, and corticosteroid therapy was marked by death the day before the neurosurgical procedure after initial improvement.
Keywords
Cerebral cyst
human immunodeficiency virus
hydatid cyst

INTRODUCTION
Hydatidosis is a rare cosmopolitan disease caused by the accidental infestation of man with the tapeworm Echinococcus granulosus (echinococcus), a parasite of canids.[1] The hydatid cyst can lodge in several viscera of the human body and the most usual ones are liver, lungs, and brain. The positive diagnosis is mainly imaging showing a characteristic appearance. The cerebral hydatid cyst is rarely reported in our country.
MEDICAL OBSERVATION
We report the case of a 30-year-old woman who has been immunosuppressed to the human immunodeficiency virus (HIV) for 6 years and was on high-active antiretroviral therapy and who was not observant. She was admitted on November 30, 2017, for the management of motor deficit of the left side of rapidly progressive installation. The story reveals an onset dating back to March 2017 with the onset of fever, episodes of generalized tonic–clonic epileptic seizures, and motor deficit of the left hemibody that appeared 2 months later.
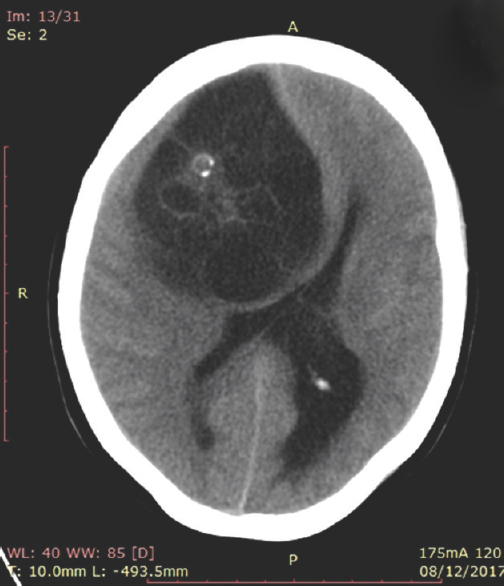
After wandering in several health centers, she consulted a neurologist 8 months after the onset of signs, At the admission the examination showed a deterioration of general state, she was sleepy with decrease of consciousness with a Glasgow Coma Scale of 12 (E3V4M5); motor weakness in left side and bilateral Babinski sign. Biology test showed the HIV-positive with HIV1; the blood cell count showed predominantly lymphocytic leukocytosis and C-reactive protein at 40 mg/L. The cerebral computed tomography (CT) without and with injection found a cystic formation multiseptate right parietal fronto of approximately 83 mm × 62 mm and the presence of an annular calcification of approximately 8 mm. There is falcorial involvement and contralateral ventricular dilatation [Figures 1 and 2]. Based on CT-scan images, a diagnosis of cerebral hydatid cyst was made. She was hospitalized and treated with phenobarbital, clonazepam, adjunctive corticosteroid therapy, albendazole, and cotrimoxazole. Thirty-six hours after the beginning of the treatment, there was an improvement of the general state, of the state of consciousness, and of the motor deficit with a muscular force to 3/5 and a stop of the epileptic seizures. A neurosurgical intervention was proposed, but the patient and her family decided to return against medical advice for financial reasons. She returned 6 weeks later in a state of epilepticus and was transferred to intensive care. The surgery was finally accepted and scheduled for January 30, 2018, but unfortunately, she died the morning of January 30, 2018.

- Cerebral computed tomography – scan without injection
- Computed tomography – scan with injection
DISCUSSION
The hydatid cyst, also called hydatid echinococcosis or hydatidosis, is a parasitic disease caused by E. granulosus. It is a parasite that touches the human body through animal contact. It is a cosmopolitan disease, found mainly in traditional sheep-rearing countries (developing countries) and sometimes a real public health problem.[1] Brain localization is rare (1%–4% of cases). It occurs mainly in children and young adults, with a clear predominance of the male sex.[234] The circumstances of discovery are not specific and the clinic may be dominated by signs of intracranial hypertension (HTIC), convulsive seizures, motor and/or sensory deficit signs, as well as disorders of consciousness. A cerebellar syndrome may also be observed in rare cases since the preferred location of the cyst at the cerebral level is the white matter at the supratentorial stage. The location under tentorial is rare.[456] The diagnosis of certainty is with brain imaging (CT or magnetic resonance imaging). There is no specific biological assessment of orientation (hydatid serology often negative), and the diagnosis of certainty is done at the cerebral scanner which reports a pathognomonic aspect. It is a well-circumscribed liquid mass as “drawn with compass,” spherical or oval of variable size (often bulky in the child), united or multivesicular with thin wall, and unmodified after injection of contrast medium.[46]
The differential diagnosis is done with:[6]
-
Cystic astrocytoma – its edges are irregular, its wall is thick with a nodule wall
-
Porencephalic cavities and arachnoid cysts (peripheral seat and nonspherical shape)
-
Squamous cyst – more irregular contours and heterogeneous density
-
A brain abscess.
Once identified, hydatidosis should be treated by surgery or by a technique called aspiration puncture. In the absence of treatment, the spontaneous involution of the cyst is very rare; the evolution toward the calcification is exceptional (1% of the cases) and indicates their chronicity.[3478]
CONCLUSION
The hydatid cyst of the brain remains a rare condition. There is no biological assessment of orientation. Only cerebral imaging makes it possible to pose the diagnosis of certainty with its characteristic appearance. The management is essentially surgical. Prevention is the only way to eradicate the cyst.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Growth of intracerebral hydatid cyst evaluated by computed tomography (1case) Neurochirurgie. 1990;36:312-4.
- [Google Scholar]
- Hydatid infestation of the brain: Difficulties with computed tomography diagnosis and surgical treatment. Pediatr Neurosurg. 1994;20:78-83.
- [Google Scholar]




