
Translate this page into:
Cerebral aneurysm in a patient with Loeys-Dietz syndrome
Address for correspondence: Dr. Luis Rafael Moscote-Salazar, Universidad de Cartagena, Cartagena de Indias, Colombia, E-mail: mineurocirujano@aol.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
The Loeys-Dietz syndrome (LDS) is an autosomal dominant genetic disease, characterized by the presence of cerebral, thoracic or abdominal arteries aneurysms or dissections, and skeletal manifestations. There are two different types: Type I with craniofacial manifestations and a triad of arterial tortuosity, hypertelorism, and bifid uvula or palate, and type II with cutaneous manifestations that have no craniofacial abnormalities or cleft palate, but have bifid uvula.
The symptomatic patient was a 46-year-old woman with LDS, who presented with aneurysm rupture of the abdominal aorta, which was surgically resolved and genetic mutation was identified in the resected specimen and blood, confirming the clinically suspected diagnosis. During her stay in the institution, brain magnetic resonance imaging (MRI) was performed, which revealed the presence of two intracranial aneurysms, one located in the carotid artery and one in the vertebral artery, the latter with a wide neck [Figures 1 and 2]. The management was decided by endovascular therapy, thus embolization of the aneurysms was performed. The patient evolved satisfactorily.
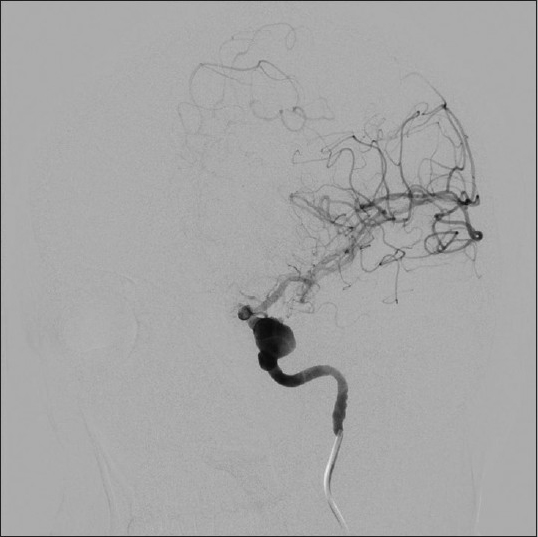
- Cerebral angiography, oblique view, with right internal carotid injection showing a cavernous aneurysm
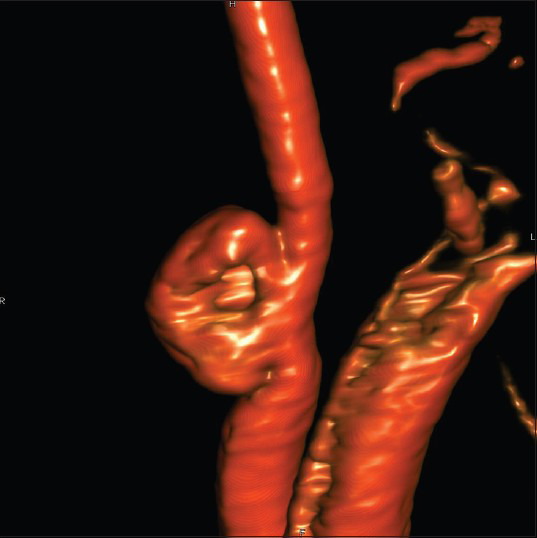
- Vertebral angiogram with 3D rotational reconstruction image demonstrating a right vertebral artery aneurysm
In 2005, this rare syndrome was described by Loeys et al. The endovascular management of intracranial aneurysms associated with Loeys-Dietz syndrome has been reported rarely in the literature.[1]
Vascular dilatation or dissection of the aorta and/or aneurysms and arterial tortuosity can be detected by angioresonance or an angio view in 95% of the cases. Patients may have mitral valve prolapse, ectasia of the pulmonary artery, patent ductus arteriosus, atrial septal defects or a bicuspid aortic valve. The skeletal manifestations include: Pectus excavatum or pectus carinatum, scoliosis, joint laxity, like: Positive thumb and wrist signs and/or equine varus feet; arachnodactyly, flat feet, osteoporosis, brachycephaly or trigonocephaly, and may have malar hypoplasia with retrognathia.[2]
Cutaneous findings include: Thin skin with very visible venous circulation, friable, and poor healing. Others: Disorders of refraction (myopia), dental enamel dysplasia, and atlantoaxial instability. Spontaneous rupture of the spleen, intestine or uterus during pregnancy, have also been reported. Complications include rupture of aneurysms, with a mean age of 26 years, and a high rate of obstetric complications.[3]
The differential diagnosis includes Marfan syndrome, congenital contractural arachnodactyly, mitral valve prolapse, aortic enlargement, skin and skeletal findings, (MASS) syndrome, vascular Ehlers Danlos, and others pathologies. In the Loeys-Dietz syndrome, abdominal aneurysms have been identified in 10% of patients; the aneurysms may involve the iliac arteries. Diagnosis of the Loeys-Dietz syndrome is based primarily on the clinical features and is confirmed by molecular genetic testing of the TGFBR1 and TGFBR2 genes. The approach to patients with intracranial aneurysms, in the context of Loeys-Dietz syndrome, by the endovascular technique, is safe and effective and should be considered in the integrated management strategies for this rare disease.[456]
References
- Clipping of a cerebral aneurysm in a patient with Loeys-Dietz syndrome: Case report. Neurosurgery. 2011;69:E746-55.
- [Google Scholar]
- TGFBR1 and TGFBR2 mutations in patients with features of Marfan syndrome and Loeys-Dietz syndrome. Hum Mutat. 2006;27:770-7.
- [Google Scholar]
- Analysis of multigenerational families with thoracic aortic aneurysms and dissections due to TGFBR1 or TGFBR2 mutations. J Med Genet. 2009;46:607-13.
- [Google Scholar]
- Association of intracranial aneurysm and Loeys-Dietz syndrome: Case illustration, management, and literature review. Neurosurgery. 2011;69:E488-93.
- [Google Scholar]
- Arterial tortuosity and aneurysm in a case of Loeys-Dietz syndrome type IB with a mutation p. R537P in the TGFBR2 gene. Turk J Pediatr. 2012;54:198-202.
- [Google Scholar]
- Aneurysm syndromes caused by mutations in the TGF-beta receptor. N Engl J Med. 2006;355:788-98.
- [Google Scholar]




