
Translate this page into:
Behavioral Problems and Intelligence Quotient Changes in Pediatric Epilepsy: A Case–Control Study
Address for correspondence: Dr. Shyama Choudhary, 5, Ramnagar, Behind RTO Office, Jodhpur - 342 010, Rajasthan, India. E-mail: shyama04dr.snmc@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Epilepsy is the most common chronic neurological disease and has neurological impairment as an important comorbidity.
Objective:
To find behavioral problems and intelligence quotient (IQ) changes associated with epilepsy and to know the association of variables such as frequency, type of seizures, and duration of disease with cognitive impairment.
Materials and Methods:
A descriptive cross sectional study, consisting of 50 cases (patients of epilepsy) and 50 controls (other patients of same socioeconomic status) was conducted at S.P. Medical College, Bikaner. The patients were subjected to detailed clinical history, thorough examination, Pediatric Symptom Checklist, and Bhatia's Battery of Performance intelligence Test. Data analysis was carried out with the help of SPSS 22 software.
Results:
The prevalence of behavioral problems in generalized and partial seizure group was high (42% and 53.8%) as compared to control group (9%). Low IQ was present more in the patients (44%) of generalized and partial seizure group as compared with the control group, and results were statistically significant. Furthermore, behavioral problems were more in patients who were having more number of seizures (≥3 per year) with significant P values (χ2 = 5.067, P = 0.024).
Conclusion:
We conclusively found that behavioral problems and cognitive factors, apart from control of seizures, must be kept in mind to determine how well a child with epilepsy progresses toward independence.
Keywords
Checklist
cognitive dysfunction
cross-sectional study
epilepsy

INTRODUCTION
Epilepsy is the most common chronic neurological disease in the general population and childhood.[12] For epidemiological classification purposes, epilepsy is considered to be present when two or more unprovoked seizures occur at an interval >24 h.[3] A seizure is a transient, paroxysmal, pathophysiological disturbance of cerebral function caused by spontaneous, excessive discharge of neurons.[1] Less than one-third of seizures in children are caused by epilepsy.[3]
Neurological impairment is an important comorbidity of chronic epilepsy.[4] A long rich history of research has characterized relationship between cognitive status and variety of clinical epilepsy factors including etiology, age of onset, seizure type and severity, duration, antiepileptic medication, and many other factors.[45678] Several epilepsy factors influencing cognitive development have been identified.[9]
Seizure type is frequently seen as important risk factor for cognitive impairment.[9] Children with generalized seizures in general and tonic–clonic seizures in particular appear to be at higher risk for cognitive impairment compared to those with focal onset, regardless if the seizure was idiopathic or symptomatic.[2] Furthermore, individuals with generalized tonic–clonic seizures show the greatest intellectual deficit, those with simple partial seizures show the least deficit, and those with partial complex seizures had intermediate levels of intellectual development.[4]
Epileptic syndromes appear more predictive of cognitive impairment than seizure type. For example, children with benign rolandic epilepsy and juvenile myoclonic epilepsy rarely show decline in intellectual functioning regardless of number of seizures.[6] An important issue for prognosis in epilepsy is whether cognitive decline occurs over time. It has been shown that intellectual deterioration occurs in the course of epilepsy.[89101112] Frequency of seizures has been found to be correlated with behavioral problems in children with epilepsy.[1314]
Epilepsy is known to have a large impact on cognitive development and educational achievement; prognosis should not concentrate only on seizure outcome. Children who have low intelligence quotient (IQ) scores and epilepsy have an even higher death risk. Hence, the purpose of study is to find a relation between epilepsy and associated behavioral problems and IQ changes and to find association of frequency, type of seizures, and duration of disease with cognitive impairment so that pediatrician does early intervention in children with epilepsy and prevents decline in IQ leading to better psychosocial functioning and educational outcome in such children.
MATERIALS AND METHODS
It was a case–control study conducted in Department of Pediatrics in collaboration with Department of Psychiatry, S.P. Medical College and Associated Group of Hospitals Bikaner (Rajasthan). Fifty patients with epilepsy (35 males and 15 females) admitted or visiting OPD in age group 6–12 years constituted cases. Patients with seizures due to other medical conditions such as dyselectrolytemia, pyogenic and tuberculous meningitis, and simple febrile convulsions were excluded from cases. Fifty patients (33 males and 17 females) with same socioeconomic status as of the case constituted control group. Study was approved by ethical committee of the institution. For epidemiological classification purposes, epilepsy is considered to be present when two or more unprovoked seizures occur at an interval >24 h.[3] Case group was further divided into subgroups : generalized seizure group (24 patients) and partial seizure group (26 patients) and subgroups were compared with the control group through Chi-square test. Mean value of IQ was calculated and compared with control group. Patients of the case group were divided on the basis of frequency of seizures per year, and their behavioral problems and IQ changes were compared with the control group. Furthermore, a correlation was established between IQ changes, behavioral problems, and duration of disease. All the patients included in the study were subjected to detailed history and thorough clinical examination by a predesigned pro forma. The patients under study were categorized into various epileptic syndromes as defined by International League against Epilepsy (1989).
Pediatric Symptom Checklist (PSC) consists of 35 items that are rated on a 3-point scale with responses: never, sometimes, and often. The items are scored on a total score which is the simple sum of all item ratings. Regarding validity, PSC cutoff score of 28 has a sensitivity of 95% and a specificity of 68% when compared clinician's rating of children's dysfunction.
Bhatia's Battery of Performance Test of Intelligence is developed to test the intelligence of Indian Population. It includes following five subtests: (i) Kohs Block Design Test: This battery includes 10 designs from the 17 designs from the Kohs test. The time for first five designs is 2 min and for the remaining five, the time is 3 min. The cards with a variety of colored designs are shown to the test taker and he/she is asked to reproduce them using a set of colored blocks. (ii) Alexander Pass along Test: All the designs of the original test are included in this battery. The first four of these have to be completed in 2 min, and the rest of the four have to be completed in 3 min. (iii) Pattern Drawing Test: This test is constructed by Bhatia. This test includes eight cards. Every card has a pattern, and the individual is required to draw these patterns in one go without lifting the pencil. The time for the first four cards in 2 min and for the rest of the four cards, it is 3 min. (iv) Immediate memory: This test has two parts: digit span forward and digit span backward. The test taker is required to repeat the numbers the examiner says. The number of digit is increased on every trail. The test is continued till the individual repeats it successfully in the same order. In digit span backward test, the numbers are repeated in the backward position, from the last to the first. This recall is also continued till the individual successfully repeats the sequence. (v) Picture Construction Test: This test requires the individual to construct a picture that is given in parts. The parts are meaningfully combined to construct the picture. The time for first two pictures is 2 min and for the rest of the three pictures, it is 3 min. Individual administration of this test takes <1 h.
Statistical analysis
SPSS 22 software (IBM) was used for statistical analysis. For comparison of dichotomous variables, Chi-square test was used. Difference was considered significant when P < 0.05.
RESULTS
Behavioral problems were more prevalent (44%) in cases than controls (χ2 = 8.048, P = 0.008) as shown in Figure 1. One-third (34%) of cases had low IQ as compared to 8% of controls (χ2 = 8.680, P = 0.003) as shown in Figure 2. Mean IQ of the cases (89 ± 16.45) was significantly lower than control group (103.8 ± 14.83) (z test = 4.470, P = 0.0001). The prevalence of behavioral problems in generalized seizure group was significantly higher (42%) than control group (9%) (χ2 = 3.600, P = 0.05). Behavioral problems were more (53.8%) in partial seizure group as compared to control group (χ2 = 8.785, P = 0.003). The prevalence of low IQ was significantly higher in the patients of generalized seizure group (37.5%) than the control group (χ2 = 7.824, P = 0.005). The prevalence of low IQ in partial seizure group was significantly higher than control group (χ2 = 5.067, P = 0.024). Furthermore, behavioral problems were more prevalent in patients having more number of seizures (≥3 per year) (χ2 = 5.067, P = 0.024). Negative correlation was found between IQ changes, duration of disease, and behavioral problems in epilepsy patients.
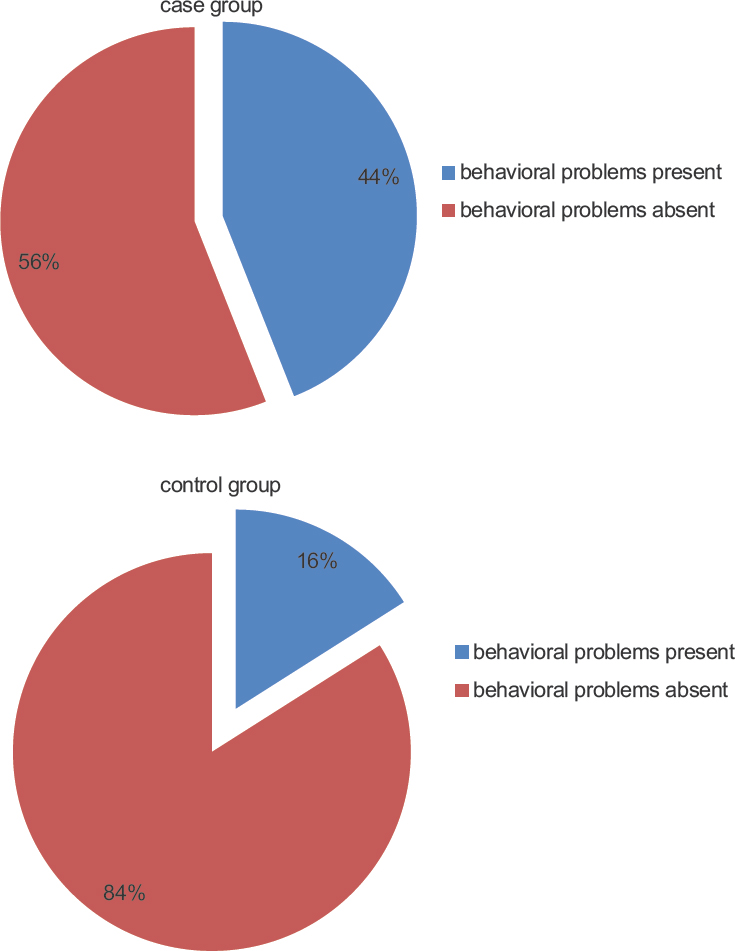
- Comparison of case and control group on the basis of prevalence of behavioral problems (χ2 = 8.048, P = 0.008)
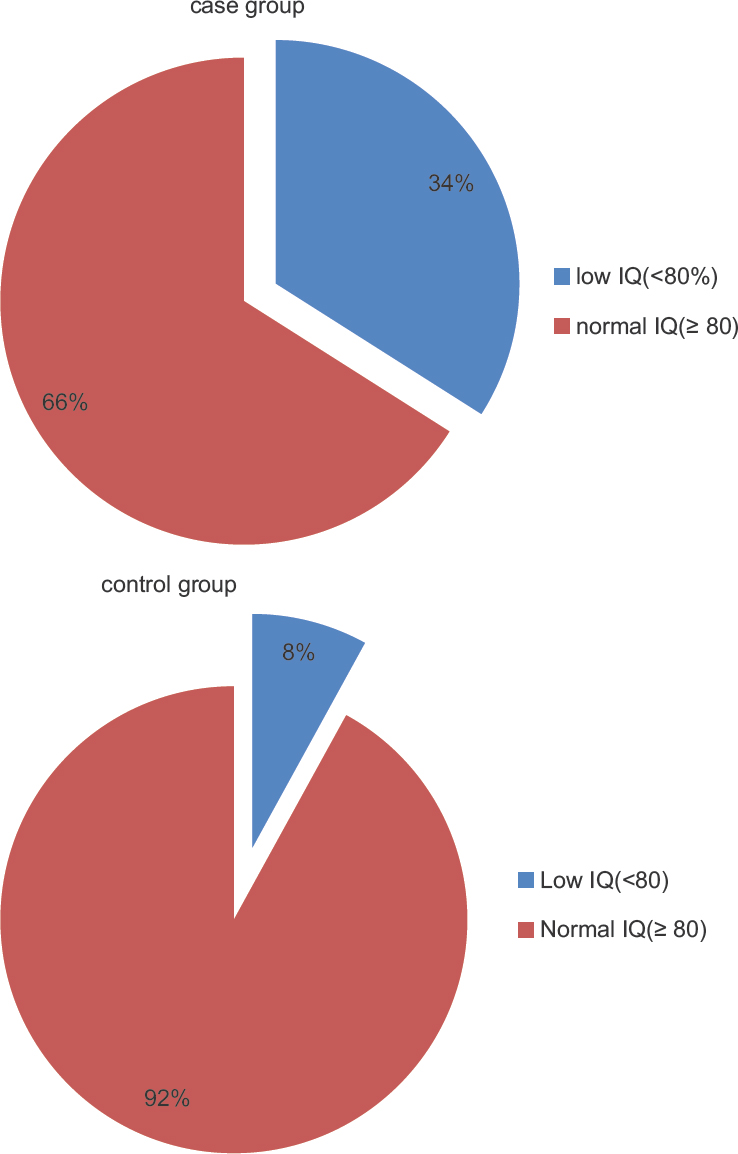
- Comparison of case and control group on the basis of prevalence of intelligence quotient (χ2 = 8.680, P = 0.003)
DISCUSSION
People with intellectual disability (ID) have a higher rate of epilepsy diagnoses than the general population. Approximately, 14%–24% of the ID population is affected by epilepsy.[15] Bowley and Kerr[16] reported that having ID along with epilepsy affects a person's physical morbidity, which in turn leads to increased mortality and a greater burden on their family.
Rutter et al. found that 28.6% of children with uncomplicated seizures and 58.3% of those with seizures and additional neurological damage had psychosocial and behavioral problems.[17] Dodson[18] reported that children with epilepsy have an IQ score that is 10 points lower than their healthy, age-matched peers. In another study, it was found that the children with epileptic syndromes have more psychosocial problems than their peer group and they perform poorly in the school.[19] Childhood epilepsy is often associated with memory, attention and analytic deficits, reading comprehension problems, dyslexia, dyscalculia, and academic underperformance. For some epileptic children, poor reading ability is associated with specific electroencephalogram abnormalities.[20] Experiencing seizures at school, learning problems, and imposed limitations on participation in sports, playground activities, and driving may further limit normal peer interaction and social development.[21] In our study, intellectual deficits were significantly higher in cases. IQ tends to be lower in children with earlier onset and multiple seizure types, longer and more frequent seizures, less seizure control while on medication, toxic drug levels due to medication, and multiple drug toxicity.[22] Poor academic performance has been observed most notably in arithmetic, followed by spelling, reading comprehension, and word recognition.[202223] In fact, children with epilepsy have been found to be 12–28 months behind nonepileptic peers in reading and 28 months behind in comprehension.[24]
According to one study, children with seizures were at increased risk for mental health, developmental, and physical comorbidities.[25] In our study, mean IQ was normal in both the case group and control group, but it was significantly lower in the epileptic patients as compared to control group. In our study, it was found that the prevalence of behavioral problems was higher in partial seizure group (P = 0.003). Earlier, many studies have shown that in epilepsy, psychosocial and behavioral problems coexist. In one study, it was found that frequent epileptiform discharges and polytherapy were associated with reduced educational achievement.[26] Again, when both the seizure groups were compared with control group, it was seen that low IQ (<80) was in 37.5% (P = 0.05) of the patients with generalized seizure disorders and in 30.7% (P = 0.24) of the patients with partial seizures. In one study, IQ was found low in generalized seizure patients as compared to partial seizures.[27] It was also indicated that individuals with generalized tonic–clonic seizures show the greatest intellectual deficit, those with simple partial seizures showed the least deficit, and those with partial complex seizures had intermediate levels of intellectual impairment.[24]
Cases were further classified on the basis of frequency of seizures and behavioral problems associated with it. In patients with high frequency of seizures (≥3 per year), 92.3% of the patients were having some or the other behavioral problem as compared to 51.6% in the low frequency (<3 episodes per year, P = 0.024). Frequency of seizures has been found to be correlated with behavioral problems in children with epilepsy.[1328]
Finally, the prevalence of behavioral problems and low IQ in cases were compared on the basis of duration of the disease. It was found that in patients with long disease duration, IQ was mostly on the lower side, and significant number of patients had behavioral problems [Figure 3]. Behavioral problems in such patients could be as result of low IQ or vice versa. There is a general suggestion in the literature that early age of onset and long duration of the epilepsy have a negative influence on the patients’ cognitive abilities.[29] Early age of onset has also been associated with more behavioral problems.[30] It has been reported that three variables accounted for the variance in IQ scores, specifically years with seizure disorder (38%), followed by seizure duration (16%) and age of onset (9%).[20]
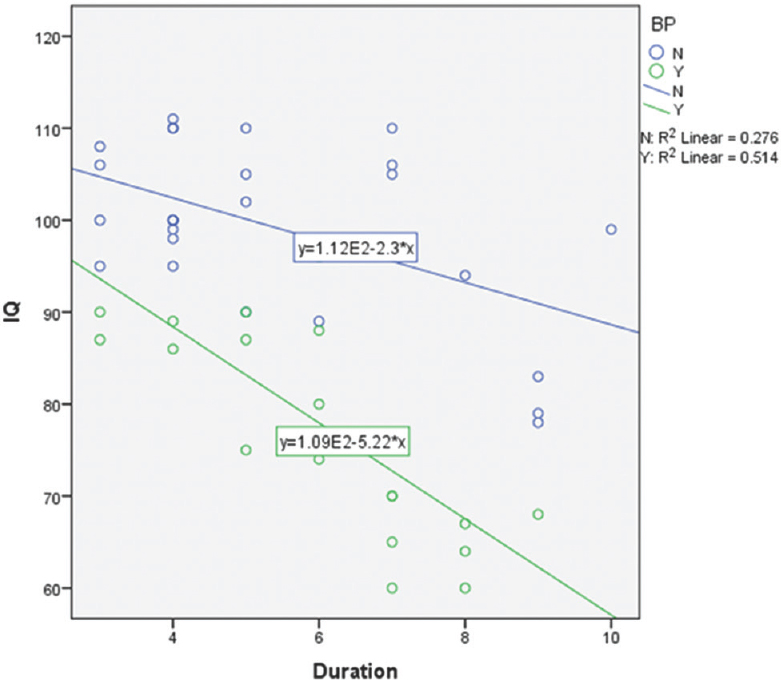
- Correlation of intelligence quotient, duration of disease, and behavioral problems in epilepsy patients
CONCLUSION
Epilepsy is associated with intellectual deficits and behavioral problems that correlate with frequency of seizures and duration of disease. Having intellectual deficits along with epilepsy affects a person's physical morbidity, which in turn leads to increased mortality and a greater burden on their family. The pediatrician must look out for epilepsy in children so that the early intervention can be warranted and a decline in IQ can be prevented which will improve psychosocial functioning and educational outcome in children.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Neurocognitive disorders. Kaplan & Sadock's Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Philadelphia: Wolters Kluwer; 2015. p. :723.
- Educational underachievement in children with epilepsy: A model to predict the effects of epilepsy on educational achievement. J Child Neurol. 2005;20:175-80.
- [Google Scholar]
- Seizures in childhood. In: Nelson Textbook of Pediatrics (19th ed). Philadelphia, PA: Saunders, An Imprint of Elsevier; 2016. p. :2013.
- [Google Scholar]
- The relative influence of epileptic EEG discharges, short nonconvulsive seizures, and type of epilepsy on cognitive function. Epilepsia. 2004;45:54-63.
- [Google Scholar]
- Memory and epilepsy: Characteristics, course, and influence of drugs and surgery. Curr Opin Neurol. 2001;14:211-6.
- [Google Scholar]
- Lateralization of verbal memory and unilateral hippocampal sclerosis: Evidence of task-specific effects. J Clin Exp Neuropsychol. 1993;15:608-18.
- [Google Scholar]
- Seizure-related factors and non-verbal intelligence in children with epilepsy. A population-based study from Western Norway. Seizure. 2005;14:223-31.
- [Google Scholar]
- Is epilepsy a progressive disorder? prospects for new therapeutic approaches in temporal-lobe epilepsy. Lancet Neurol. 2002;1:173-81.
- [Google Scholar]
- Predicting cognitive impairment in epilepsy: Findings from the bozeman epilepsy consortium. J Clin Exp Neuropsychol. 1995;17:909-17.
- [Google Scholar]
- Correlates of behavior problems in children with epilepsy. Epilepsia. 1992;33:1115-22.
- [Google Scholar]
- Depression in epilepsy: Etiology, phenomenology, and treatment. Epilepsia. 1999;40(Suppl 10):S21-47.
- [Google Scholar]
- Epidemiology and treatment of epilepsy in patients who are mentally retarded. CNS Drugs. 2000;13:117-28.
- [Google Scholar]
- Epilepsy and intellectual disability. J Intellect Disabil Res. 2000;44(Pt 5):529-43.
- [Google Scholar]
- A Neuropsychiatric Study in Childhood. London, Philadelphia: Heinemann Medical, J.B. Lippincott Co; 1970.
- Epilepsy, cerebral palsy, and IQ. In: Pellock JM, Dodson WE, Bourgeois BF, eds. Pediatric Epilepsy Diagnosis and Therapy. New York: Demos Medical Publishing; 2002. p. :613-27.
- [Google Scholar]
- Symptoms of anxiety and depression among adolescents with seizures in Irbid, Northern Jordan. Seizure. 2000;9:412-6.
- [Google Scholar]
- Fundamentals of Clinical Child Neuropsychology 1988
- The neuropsychology of epilepsy. In: Reynolds CR, Fletcher-Janzen E, eds. Handbook of Clinical Child Neuropsychology. Boston, MA: Springer US; 1997. p. :506-16.
- [Google Scholar]
- Neurobehavioral abnormalities in epilepsy. Pediatric Behavioral Neurology. Boca Raton: CRC Press; 1996. p. :269-87.
- Children with Complex Medical Issues in School: Neuropsychological Descriptions and Interventions 2008
- The neuropsychology of pediatric epilepsy and antiepileptic drugs. In: Reynolds CR, Fletcher-Janzen E, eds. Handbook of Clinical Child Neuropsychology. Boston, MA: Springer US; 2009. p. :505-28.
- [Google Scholar]
- A national profile of childhood epilepsy and seizure disorder. Pediatrics. 2012;129:256-64.
- [Google Scholar]
- Differential diagnosis and treatment of psychiatric disorders in children and adolescents with epilepsy. Epilepsy Behav. 2004;5(Suppl 3):S10-7.
- [Google Scholar]
- Psychopathology in children: Improvement of quality of life without psychiatric symptom reduction? Eur Child Adolesc Psychiatry. 2005;14:364-70.
- [Google Scholar]
- Effect of major motor seizure frequency upon cognitive-intellectual functions in adults. Epilepsia. 1977;18:21-9.
- [Google Scholar]




