
Translate this page into:
Psychometric Properties and Correlates of the Beck Hopelessness Scale in Family Caregivers of Nigerian Patients with Psychiatric Disorders in Southwestern Nigeria
Address for correspondence: Dr. Olutayo Aloba, Department of Mental Health, Obafemi Awolowo University Teaching Hospitals Complex, Ife, Osun State, Nigeria. E-mail: alobatee2002@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives:
To examine the construct and correlates of hopelessness among family caregivers of Nigerian psychiatric patients.
Materials and Methods:
This is a cross-sectional, descriptive study involving 264 family caregiver-patients’ dyads recruited from two university teaching hospitals psychiatric clinics in Southwestern Nigeria.
Results:
Exploratory factor analysis revealed a two-factor 9-item model of the Beck Hopelessness Scale (BHS) among the family caregivers. Confirmatory factor analysis of the model revealed satisfactory indices of fitness (goodness of fit index = 0.97, comparative fit index = 0.96, Chi-square/degree of freedom (CMIN/DF) = 1.60, root mean square error of approximation = 0.048, expected cross-validation index = 0.307, and standardized root mean residual = 0.005). Reliability of the scale was modestly satisfactory (Cronbach's alpha 0.72). Construct validity of scale was supported by significant correlations with the family caregivers’ scores on the Zarit Burden Interview, mini international neuropsychiatric interview suicidality module, General Health Questionnaire-12 (GHQ-12), and Patient Health Questionnaire-9. The greatest variance in the family caregivers’ scores on the BHS was contributed by their scores on the psychological distress scale (GHQ-12).
Conclusions:
The BHS has adequate psychometric properties among Nigerian psychiatric patients’ family caregivers. There is the need to pay attention to the psychological well-being of the family caregivers of Nigerian psychiatric patients.
Keywords
Beck Hopelessness Scale
Nigerian family caregivers
psychiatric patients

INTRODUCTION
One factor that has been consistently recognized as the strongest predictive factor for suicide, either attempted or completed is hopelessness.[123] Hopelessness has been defined as the manifestation of a current reasoning attitude that reflects adverse or unfavorable anticipation concerning the future.[4] It has been demonstrated that there is a positive correlation between caregiving and caregivers’ psychological distress.[5] Family caregivers are usually the providers of informal care for patients with chronic mental disorders.[67] The provision of care to a family member with a chronic mental disorder can be quite daunting, and there is the tendency for family caregivers to experience being oppressed by the associated tasks involved.[8] In developing countries, such as Nigeria, family caregivers have a central role in the societal reintegration of their relatives affected with severe mental disorders, which is mainly due to the dearth of professionals that are required for their rehabilitation.[9] Studies have also demonstrated that the overwhelming burden arising from providing care for a family member with severe mental disorder can adversely affect the caregivers’ psychological well-being.[1011] About a quarter of family caregivers of patients with chronic mental disorders either resident or not with their relative fulfill the criteria for possible cases of psychiatric disorders according to the General Health Questionnaire (GHQ).[12]
An electronic literature search revealed that most of the studies of hopelessness among family caregivers in developed countries, involved those of patients with oncological disorders.[13141516] Most of the studies among Nigerian family caregivers of patients with chronic medical disorders have focused predominantly on measuring the burden experienced by the family caregivers.[81718] It has been suggested that medical care providers need to take into consideration the susceptibility to psychological distress among the family caregivers of patients with chronic medical disorders.[15] Studies have also reported that family caregivers with depression or anxiety due to the burden of caregiving have a higher prevalence of suicidal ideation and were at an elevated risk for suicide.[19] Hopelessness in caregivers may reduce their stress absorbing abilities and increased levels of hope has been reported to have statistically significant correlations with reduced psychological dysfunctions among caregivers.[14] The most globally recognized and utilized scale for the measurement and quantification of hopelessness is the Beck Hopelessness Scale (BHS).[20] No study has examined the construct of hopelessness and its correlates among Nigerian family caregivers of psychiatric patients.
MATERIALS AND METHODS
This is a cross-sectional descriptive study involving 264 family caregiver-patient dyads, who were recruited over a period of 6 months (September, 2015 to February, 2016) from the outpatient psychiatric clinics of two tertiary health-care centers in Southwestern Nigeria. These two tertiary referral centers provide health-care services for a large number of surrounding rural communities. Eligibility criteria for the patients were (1) aged 18 years and above, (2) must have been an outpatient in these centers for at least 6 months, (3) the severity of psychopathological disturbance being experienced by the patient is not to the extent where it will interfere with their ability to give consent. The inclusion criteria for family caregivers were (1) must have been responsible for providing care for the patient within the preceding 3 months, without any financial benefits, (2) patient must identify him or her as been the principal caregiver, (3) must be aged 18 years and above, (4) must not have a chronic mental or medical disorder that could independently affect their functioning, (5) must give consent to participate in the study. The study protocol was approved by the Ethics and Research Committees of the two health-care institutions.
Measures
Study measures completed by the patients
Patients’ sociodemographic and illness-related questionnaire
This is a semi-structured questionnaire that included variables such as, age, gender, marital status, and number of years of education.
Global Assessment of Functioning Scale
This scale was utilized to objectively measure the level of patients’ functioning. Scores on the scale range from 0 to 100, with higher functioning indicated by higher scores on the scale.[21]
Positive and negative syndrome scale
A clinician-administered scale which consists of 30 items evaluating positive (7 items), negative (7 items), and general (16 items) symptoms of psychosis, with each item measured on a 7-point Likert scale.[22]
Hamilton Depression Rating Scale
This clinician-administered scale consisting of 17 items was utilized to measure the level of depressive symptoms over the preceding week among the patients.[23] Higher scores reflects greater depressive symptoms severity.
Young Mania Rating Scale
This scale was employed in assessing the severity of manic symptoms among the patients with bipolar disorder. It consists of 11 items and the total score on the scale range from 0 to 60, with higher scores reflecting greater mental state disturbance in the context of a manic episode.[24]
Study measures completed by the family caregivers
Caregiver sociodemographic information form
This consist of family caregivers’ variables such as age, gender, marital status, employment status, and relationship to the patient, number of years of education, and duration of providing care for the patient.
Beck Hopelessness Scale
This is a 20-item scale developed in 1974 by Beck et al.[25] The scale has been described as the most consistent instrument to predict suicide.[26] The response to each item on the scale is either a yes or no. Each item is worded such that the respondent completing the scale either admits a “yes” to a negatively worded item or indicates a “no” to a positively worded item. Total score on the complete scale range from 0 to 20, with greater levels of hopelessness reflected by higher scores on the scale.
Mini international neuropsychiatric interview suicidality module
Suicidality among the family caregivers was evaluated with the mini international neuropsychiatric interview (MINI) suicidality module section.[27] The total score on this module was calculated by summing up the points per questions depending on the respondents’ responses. The previous studies have reported strong positive correlations between hopelessness and suicidality.[2829]
Zarit Burden Interview
The level of burden subjectively experienced by the family caregivers was quantified with the 22-item Zarit Burden Interview (ZBI).[30] Each item is measured on a five-point Likert scale, ranging from 0 (never) to 4 (almost always). Higher scores reflect a more severe level of subjective burden by the family caregivers. The scale has been shown to exhibit satisfactory psychometric properties among the caregivers of Nigerian patients with chronic mental disorders.[818313233]
General Health Questionnaire-12
The Yoruba language translated version of this 12-item psychological distress scale has been demonstrated to be reliable and valid.[34] Each of the items was scored using the 0-0-1-1 method and individuals with an aggregate score of three points and above were recognized as been psychological distressed.[35]
Patient Health Questionnaire-9
This is a brief 9-item subjectively completed scale for screening and measuring the severity of depressive symptomatology.[36] Each item is scored on a four-point Likert scale (not at all-0 to nearly every day-3), producing a total score ranging from 0 to 27. Adequacy of reliability and validity of the Patient Health Questionnaire-9 (PHQ-9) has been reported among different Nigerian clinical and nonclinical populations.[373839]
Data analysis
This was performed with the 21st version of the International Business Machine's Statistical Package for Social Scientists (IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp). The reliability of the BHS was explored by calculating the Cronbach's alpha while the construct validity of the BHS was examined with correlational analyses with selected family caregivers’ and patients’ variables. Exploratory factor analysis (EFA) applying principal axis factoring (PAF) with oblimin rotation was employed to examine the loading patterns of the items of the BHS among the family caregivers. The fit of the factor model of the BHS extracted with PAF was then subjected to confirmatory factor analysis (CFA) performed using the analysis of moment structures software, 20th version. Satisfactory model fit was based on the Hu and Bentler criteria,[40] in which the goodness of fit index (GFI) and comparative fit index (CFI) values will be close to or >0.95; root mean square error of approximation (RMSEA) and standardized root mean residual (SRMR) square <0.05, minimal expected cross-validation index (ECVI) value, Chi-square/degree of freedom ratio (CMIN/DF) <2.0, and a nonsignificant Chi-square P value. Regression analyses were employed to identify which variable significantly predicted the family caregivers’ hopelessness scores. The level of statistical significance was set at P < 0.05 and all statistical tests were two-tailed.
RESULTS
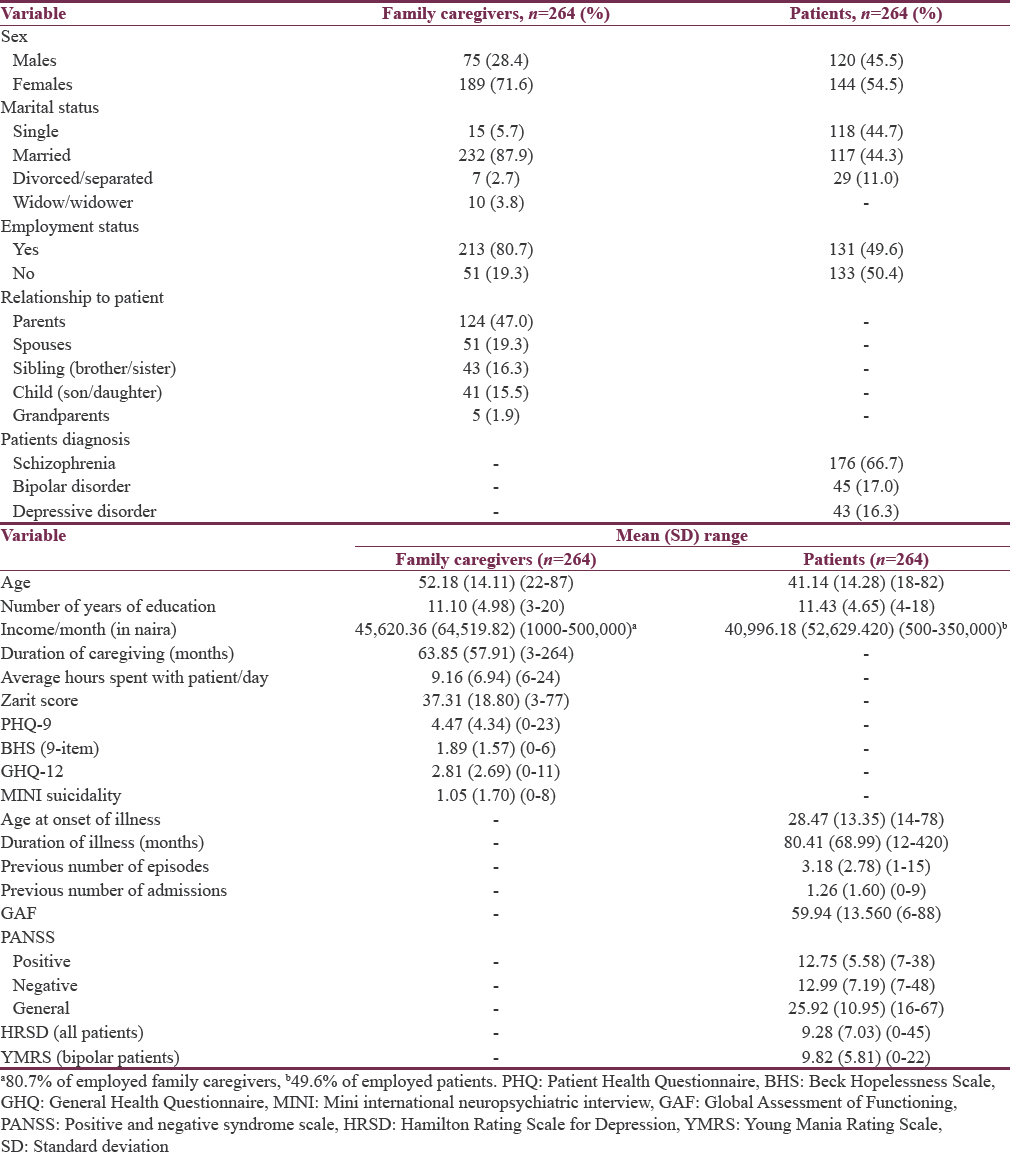
Descriptive statistics of the family caregivers (n = 264) and the patients (n = 264)
The duration of caregiving and the average hours spent per day with their relative were 63.85 (standard deviation [SD] 57.91) months and 9.16 (SD 6.94) hours, respectively. The largest proportion of the family caregivers were females (71.6%) and those who were married (87.9%). Among the family caregivers, the mean score on the 9-item BHS was 1.89 (SD 1.75) [Table 1].
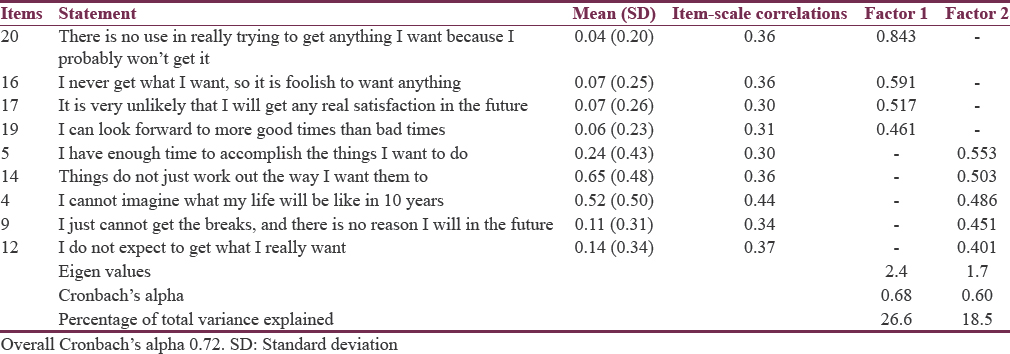
Descriptive details and Cronbach's alpha of the Beck Hopelessness Scale among the family caregivers (n = 264) with the factor loading extracted with principal axis factoring
Initial examination of the descriptive characteristics of the 20 items of the BHS revealed that item total scale correlations were <0.30 for items 3, “When things are going badly, I am helped by knowing they cannot stay that way forever”, six, “In the future, I expect to succeed in what concerns me the most” and ten, “My past experiences have prepared me well for the future”. These 3 items were eliminated since a correlation value <0.3 indicated that the corresponding item does not correlate adequately with the overall scale.[41] The remaining 17 items were subjected to PAF with oblimin rotation because we assumed that the extracted factors will be correlated. The Kaiser-Meyer-Olkin of sampling adequacy was acceptable (>0.50)[42] and Bartlett's test of sphericity[43] indicated that our data were appropriate for subjection to factor analysis. We decided to retain only the scale's items with factor loading values that exceeds 0.40. Following this approach, we had to eliminate 8 items due to factor loading values <0.40, leaving 9 items (4, 5, 9, 12, 14, 16, 17, 19, and 20). We than repeated the PFA with these 9 items, which finally yielded a two-factor model of the BHS shown in Table 2, with Factor 1 (4 items, Eigen value 2.4) and Factor 2 (5 items, Eigenvalue 1.7) accounting for 26.6% and 18.5% of the variance, respectively, with both factors cumulatively accounting for 45.1% of the total variance in the BHS among the family caregivers. Cronbach's alpha for the 9-item BHS was 0.72. Figure 1 depicts the CFA path diagram. The GFI (0.97), CFI (0.96), CMIN/DF (1.60), RMSEA (0.048), ECVI (0.307), and SRMR (0.005) all indicated adequateness of our model fit. The Chi-square fit index had a significant P value (0.034), which may be attributed to the relatively large sample size, which can lead to diminished Chi-square values.[44]
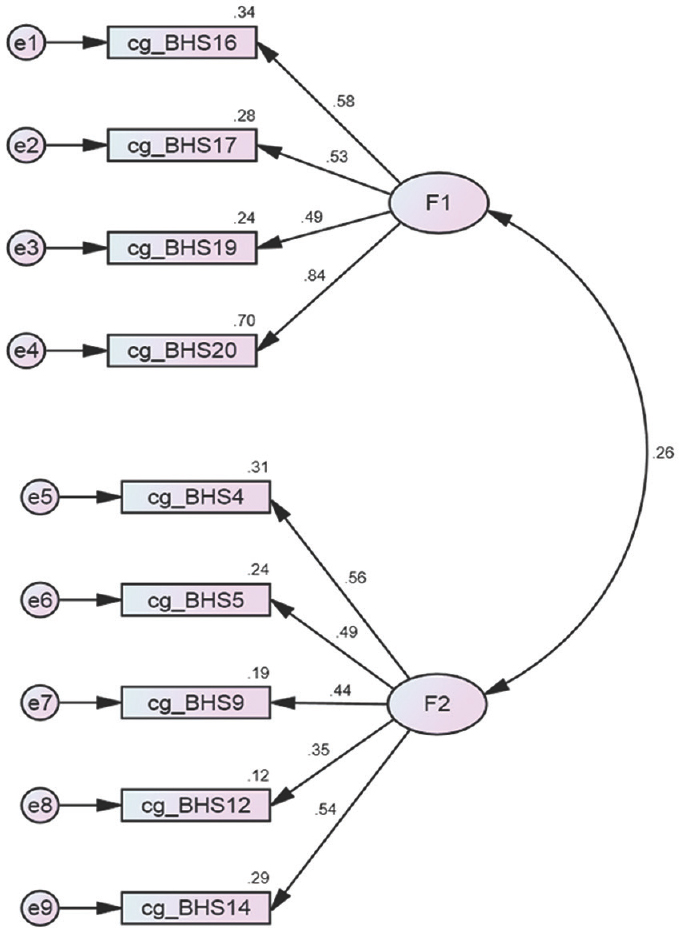
- Path analysis with confirmatory factor analysis showing the factor loading of each item on the two-factor nine items Beck Hopelessness Scale among the family caregivers. Goodness of fit indices: χ2 = 36.9; df = 23; CMIN/DF = 1.60; P = 0.034; GFI = 0.97; CFI = 0.96; SRMR = 0.005; RMSEA = 0.048; ECVI = 0.307. GFI: Goodness of fit index, CFI: Comparative fit index, SRMR: Standardized root mean residual, RMSEA: Root mean square error of approximation, ECVI: expected cross-validation index
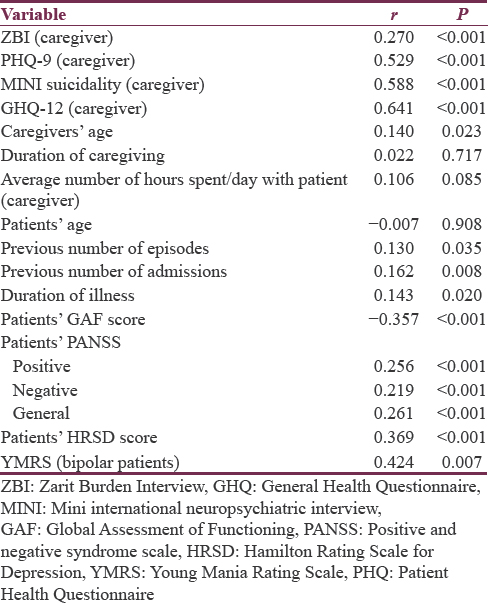
Correlational analyses of the 9-item Beck Hopelessness Scale with the family caregivers’ and patients’ characteristics
As seen in Table 3, bivariate analysis revealed that BHS had significant positive correlations with the PHQ-9 (r = 0.529, P < 0.001), MINI Suicidality module (r = 0.588, P < 0.001), GHQ-12 (r = 0.641, P < 0.001), and modest positive correlations with the ZBI (r = 0.270, P < 0.001).
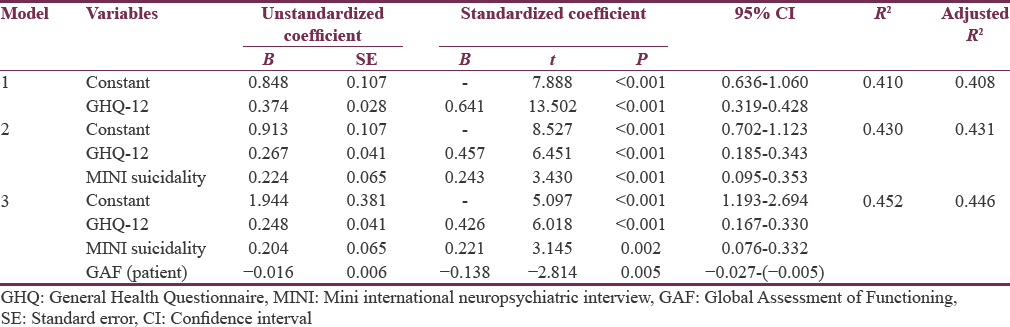
Multiple linear regression models
Linear regressions employing a stepwise approach indicated that the combinations of the family caregivers’ score on the GHQ-12, MINI Suicidality module, and patients’ Global Assessment of Functioning scores statistically predicted their scores on the BHS. It can also be observed that the largest variance (approximately 41%) in the BHS among the family caregivers was contributed by their scores on the GHQ-12 scale [Table 4].
DISCUSSION
The factorial structure of the BHS, after eliminating all the items with either low item-scale correlations or low factor loadings, produced a two-factor 9-item model among the Nigerian psychiatric patients’ family caregivers. We decided to label the factors as “negative cognition regarding the future (Factor 1)” and “negative expectations regarding the future (Factor 2).” The scale's developers utilizing principal component analysis as the factorial structure extraction method in their original study involving 294 individuals who had previously attempted suicide yielded a model with three factors namely “feeling about the future,” “loss of motivation,” and “future expectations.”[25] Among all, the previous studies that had examined the factor structure of the BHS, none had been able to replicate a factor model structure that is exactly similar to what was described by the scale's developers either in terms of the number of factors or the items constituting the factors.[45] The lack of specificity or exactness regarding the factor structure of the BHS in both patients and nonclinical population has been previously described.[46] In the context of patients’ population, a three-factor BHS model has been advanced to be the most applicable,[47] an observation that has been recently reported among Nigerian patients with psychiatric disorders.[45] Because of the lack of clarity regarding the definition and construct of hopelessness in the nonclinical general population, it has been suggested that there may be a difference in the factor structure of the BHS between patients and the general population.[48] The factor structure of the BHS may be less complicated in the nonclinical population.[49] Similar to what was observed in this study, a number of previous authors have reported a two-factor model of the BHS in the nonclinical population. A descriptive study involving 544 undergraduate American students applying PAF with oblique rotation and CFA yielded a two-factor model consisting of 16 items (Factor 1–9 items and Factor 2–7 items), and the indices of fitness obtained with CFA were to some extent comparable to those of our model.[50] A two-factor 11-item model of the BHS was also described in 340 Italian college students with the authors applying EFA with oblique rotation.[48] We noted that the two-factor 9 item BHS model we observed among our family caregivers shared some similarities to the model among the Italian students, the Factor 1 in their model consisted of 5 items made of items 11, 16, 17, 19, and 20 while our Factor 2 was composed of four of these items (16, 17, 19, and 20). In addition, a two-factor BHS model consisting of 18 items with adequate indices of fitness has also been described in a Japanese community survey involving 154 adults[49] and another model consisting of 15 items in two samples (889) of male recruits in the United State Navy.[51] Careful examination of the entire two-factor BHS models revealed lack of similarities among them despite the satisfactory psychometric properties and indices of fitness of each model described by the different authors. It has been suggested that the lack of unanimity regarding the factor structure of the BHS in all previous studies may be attributable to factors such as diverseness in the statistical analyses (e.g., differences in model extraction techniques, application of different response formats, and the different language adaptation of the scale in some studies).[52] Some of the studies that examined the psychometric qualities of the BHS employed a five-point Likert scaling response format[4951] while others adopted the usual dichotomous response format approach.[4850] Demands have been made for more studies to further explore and ratify the theoretical structure of hopelessness, particularly in the general nonpatient populations,[50] due to the dearth of research regarding the construct and applicability of the BHS in the nonclinical population.[47] Previous authors have suggested the utility of BHS models consisting of different numbers of the scale's items, for example, 14 items,[53] 15 items,[51] 12 items,[54] and even a four-items scale.[46]
The Cronbach's alpha (0.72) of the two-factor 9-item BHS among our family caregivers was modestly acceptable. Internal consistency of a scales’ items indicated by Cronbach's alpha of 0.70 and higher is generally recognized as acceptable.[55] In addition, the item-scale correlations of the 9 items on our two-factor model (0.30–0.44) were relatively lower compared to what has been reported in association with other two factor models.[484950] The scale's internal consistency in studies that have examined its reliability in the nonclinical population has been described to be lower (Cronbach's alpha ranging from 0.65 to 0.85),[5056] compared to what has been reported among patient population (Cronbach's alpha ranging from 0.83 to 0.93).[485758]
We noted among our family caregivers that the BHS had modestly statistically significant positive correlations with their scores on the ZBI, PHQ-9, MINI suicidality module, and GHQ-12 scales. We believe that these correlations lend credence to the construct validity of the scale among our respondents. Most of the studies in developed countries that had examined the construct of hopelessness among family caregivers were focused primarily on those caring for patients with oncological disorders.[13141659] In a cross-sectional survey of caregivers of patients with gynecological cancer in Turkey, the authors reported similar correlations between hopelessness measured with the BHS and burden.[14] Similar correlations between the BHS and scales evaluating depressive symptoms have been reported in caregivers of patients with chronic medical disorders.[131416] Studies among the clinical population have consistently affirmed the positive correlations between hopelessness assessed with the BHS and measures of suicidality.[6061] Thus, our observation of the association between the BHS and suicidality among family caregivers of Nigerian patients with psychiatric disorders is a further attestation to the BHS as a prognostic factor for suicidal ideation and attempt.[6263] The highest correlation we observed between the family caregivers’ BHS and GHQ-12 further supports the construct validity of the scale. Family caregivers of mentally ill patients have a higher likelihood of reporting poorer subjective psychological health compared to noncaregivers.[64] Caution needs to be exercised in generalizing our findings to family caregivers of patients in other regions of Nigeria because we recruited family caregivers from only two referral tertiary health care centers.
CONCLUSION
Our study appears to indicate the necessity to pay attention to the mental health well-being of Nigerian family caregivers of psychiatric patients.[64] The BHS despite the ambiguity associated with its factor structure has exhibited satisfactory psychometric properties as a measure of hopelessness among our respondents.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Clinical rating scales in suicide risk assessment. Gen Hosp Psychiatry. 2000;22:445-51.
- [Google Scholar]
- Hopelessness and positive and negative future thinking in parasuicide. Br J Clin Psychol. 2005;44(Pt 4):495-504.
- [Google Scholar]
- Can we predict suicide and non-fatal self-harm with the beck hopelessness scale? A meta-analysis. Psychol Med. 2007;37:769-78.
- [Google Scholar]
- Hopelessness depression: A theory-based subtype of depression. Psychol Rev. 1989;96:358-72.
- [Google Scholar]
- How is an informal caregiver's psychological distress associated with prolonged caregiving? Evidence from a six-wave panel survey in Japan. Qual Life Res. 2015;24:2907-15.
- [Google Scholar]
- Relationship of family caregiver burden with quality of care and psychopathology in a sample of Arab subjects with schizophrenia. BMC Psychiatry. 2010;10:71.
- [Google Scholar]
- A little knowledge: Caregiver burden in schizophrenia in Malawi. Soc Psychiatry Psychiatr Epidemiol. 2008;43:160-4.
- [Google Scholar]
- Correlates of caregiver burden among family members of patients with schizophrenia in Lagos, Nigeria. Schizophr Res Treatment 2013 2013:353809.
- [Google Scholar]
- Unsung samaritan in the lives of people with mental illness: An Indian experience. India J Soc Works. 2014;75:1-26.
- [Google Scholar]
- Living with a schizophrenic patient: A comparative study of burden as it affects parents and spouses. Psychiatry. 2002;65:110-23.
- [Google Scholar]
- Caregiver burden and psychotic patients’ perception of social support in a Nigerian setting. Soc Psychiatry Psychiatr Epidemiol. 2001;36:86-93.
- [Google Scholar]
- Caregivers’ stresses when living together or apart from patients with chronic schizophrenia. Community Ment Health J. 2002;38:303-10.
- [Google Scholar]
- Determinants of hopelessness and depression among Chinese hospitalized esophageal cancer patients and their family caregivers. Psychooncology. 2013;22:2529-36.
- [Google Scholar]
- The strain and hopelessness in family caregivers of patients with gynecologic cancer receiving chemotherapy. Int J Hematol Oncol. 2012;22:170-80.
- [Google Scholar]
- Determinants of a hopeful attitude among family caregivers in a palliative care setting. Gen Hosp Psychiatry. 2014;36:165-71.
- [Google Scholar]
- Caregivers of advanced cancer patients: Feelings of hopelessness and depression. Cancer Nurs. 2007;30:412-8.
- [Google Scholar]
- Perceptions of burden of caregiving by informal caregivers of cancer patients attending University of Calabar Teaching Hospital, Calabar, Nigeria. Pan Afr Med J. 2014;18:159.
- [Google Scholar]
- Factors associated with caregiver burden in a child and adolescent psychiatric facility in Lagos, Nigeria: A descriptive cross sectional study. BMC Pediatr. 2011;11:110.
- [Google Scholar]
- Suicidal ideation and suicide attempts in anxious or depressed family caregivers of patients with cancer: A nationwide survey in Korea. PLoS One. 2013;8:e60230.
- [Google Scholar]
- Quick assessment of hopelessness: A cross-sectional study. Health Qual Life Outcomes. 2006;4:13.
- [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (4th ed). Washington DC: American Psychiatric Association; 1994.
- The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13:261-76.
- [Google Scholar]
- Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. 1967;6:278-96.
- [Google Scholar]
- A rating scale for mania: Reliability, validity and sensitivity. Br J Psychiatry. 1978;133:429-35.
- [Google Scholar]
- The measurement of pessimism: The hopelessness scale. J Consult Clin Psychol. 1974;42:861-5.
- [Google Scholar]
- The prediction of parasuicide repetition in a high-risk group. Br J Clin Psychol. 1999;38(Pt 4):375-86.
- [Google Scholar]
- The mini-international neuropsychiatric interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22-33.
- [Google Scholar]
- CSF 5-HIAA, suicide intent and hopelessness in the prediction of early suicide in male high-risk suicide attempters. Acta Psychiatr Scand. 2006;113:44-7.
- [Google Scholar]
- Problems reported by self-harm patients: Perception, hopelessness, and suicidal intent. J Psychosom Res. 2002;53:819-22.
- [Google Scholar]
- Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist. 1980;20:649-55.
- [Google Scholar]
- Burden and psychological distress among Nigerian family caregivers of schizophrenic patients: The role of positive and negative symptoms. Turk Psikiyatri Derg. 2012;23:40-5.
- [Google Scholar]
- Factors associated with emotional distress among caregivers of patients with schizophrenia in Katsina, Nigeria. Soc Psychiatry Psychiatr Epidemiol. 2011;46:11-6.
- [Google Scholar]
- Caregiver burden in families of patients with depression attending Obafemi Awolowo University teaching hospitals complex Ile-Ife Nigeria. Gen Hosp Psychiatry. 2014;36:743-7.
- [Google Scholar]
- Reliability and the factor structure of the Yoruba version of the 12-item general health questionnaire. Acta Psychiatr Scand. 1991;84:125-9.
- [Google Scholar]
- The GHQ-12 as a screening tool in a primary care setting. Soc Psychiatry Psychiatr Epidemiol. 1990;25:276-80.
- [Google Scholar]
- The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-13.
- [Google Scholar]
- Somatic symptoms in depression: Evaluation of their diagnostic weight in an African setting. Br J Psychiatry. 2004;184:422-7.
- [Google Scholar]
- Validity of the patient health questionnaire (PHQ-9) as a screening tool for depression amongst Nigerian university students. J Affect Disord. 2006;96:89-93.
- [Google Scholar]
- Assessment of mental disorders using the patient health questionnaire as a general screening tool in western Nigeria: A community-based study. J Neurosci Rural Pract. 2012;3:6-11.
- [Google Scholar]
- Cutoff criteria for indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ Model. 1999;6:1-55.
- [Google Scholar]
- Discovering Statistics Using SPSS (3 Revised Edition). London: SAGE; 2009. p. :856.
- A Beginner's Guide to Structural Equation Modeling. Mahwah, NJ: Lawrence Erlbaum Associates; 2nd ed. p. :200.
- The yoruba version of the beck hopelessness scale: Psychometric characteristics and correlates of hopelessness in a sample of Nigerian psychiatric outpatients. Compr Psychiatry. 2015;56:258-71.
- [Google Scholar]
- does beck's hopelessness scale really measure several components? Psychol Med. 2001;31:367-72.
- [Google Scholar]
- Hopelessness and terminal illness: The construct of hopelessness in patients with advanced AIDS. Palliat Support Care. 2004;2:43-53.
- [Google Scholar]
- Hopelessness in a community population: Factorial structure and psychosocial correlates. J Soc Psychol. 1998;138:581-90.
- [Google Scholar]
- Further validity and reliability evidence for beck hopelessness scale scores in a nonclinical sample. Edu Psychol Meas. 2001;61:303-16.
- [Google Scholar]
- Distinguishing optimism from pessimism: Relations to fundamental dimensions of mood and personality. J Pers Soc Psychol. 1992;62:1067-74.
- [Google Scholar]
- The structure of the Beck Hopelessness Scale: A confirmatory factor analysis in UK students. Pers Individ Dif. 2011;51:17-22.
- [Google Scholar]
- Hopelessness in i.v. drug users not in treatment and seeking HIV testing and counselling. Drug Alcohol Depend. 1994;34:99-103.
- [Google Scholar]
- The experience of hopelessness in a population of Greek cancer patients receiving palliative care. Int J Soc Psychiatry. 2008;54:262-71.
- [Google Scholar]
- Research Methods in Applied Settings: An Integrated Approach to Design and Analysis. Mahwah, NJ: Lawrence Erlbaum Associates; 2000.
- Assessing the dimensionality of optimism and pessimism using a multimeasure approach. Cognit Ther Res. 1994;18:143-60.
- [Google Scholar]
- Development and validation of the xhosa translation of the beck inventories: 3. Concurrent and convergent validity. J Psychol Afr. 2008;18:227-36.
- [Google Scholar]
- Psychological Testing and Assessment. New York: Allyn and Bacon; 2002.
- Examination of the relationship between hopelessness levels and coping strategies among the family caregivers of patients with cancer. Cancer Nurs. 2015;38:E28-34.
- [Google Scholar]
- Relationship between hopelessness and ultimate suicide: A replication with psychiatric outpatients. Am J Psychiatry. 1990;147:190-5.
- [Google Scholar]
- Hopelessness and eventual suicide: A 10-year prospective study of patients hospitalized with suicidal ideation. Am J Psychiatry. 1985;142:559-63.
- [Google Scholar]
- Depression, Hopelessness, and suicidal ideation in the terminally ill. Psychosomatics. 1998;39:366-70.
- [Google Scholar]
- Hopelessness, depression and suicidal intent in parasuicide. Br J Psychiatry. 1984;144:127-33.
- [Google Scholar]
- Assessing health status in informal schizophrenia caregivers compared with health status in non-caregivers and caregivers of other conditions. BMC Psychiatry. 2015;15:162.
- [Google Scholar]




