
Translate this page into:
Penetrating Anterior Skull Base Fracture Inflicted by a Cow's Horn
Address for correspondence: Dr. Adomas Bunevicius, Hospital of Lithuanian University of Health Sciences Kaunas Clinics, Kaunas, Lithuania. E-mail: a.bunevicius@yahoo.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Farm workers are at increased risk for animal-inflicted head injuries that are associated with significant morbidity and occasionally may be fatal. These injuries may cause permanent eye damage with or without concomitant skull base fracture. Here, we present a male farmer who suffered a cow attack that resulted in perforating orbital injury with comminuted frontobasal cranial fracture caused by a cow's horn. The next day, the patient developed nasal and orbital cerebrospinal fluid (CSF) leak. Computed Tomography cisternography revealed CSF leakage to frontal and maxillary sinuses. The patient was treated using prophylactic antibiotic therapy, lumbar drainage, and underwent craniotomy for debridement and dural tear plastic. Post operative course was uneventful and there were no signs of CSF leak 1 year after the surgery. The case illustrates unusual injury inflicted by a cow's horn and underscores the importance of careful investigation for underlying skull base fracture and CSF leakage in patients sustaining perforating orbital injuries. Adequate and timely management of dural tears is associated with favorable outcomes.
Keywords
Animal-inflicted injuries
cerebrospinal fluid leak
skull base fractures

INTRODUCTION
Large farm animal-inflicted injuries are rare and most commonly occur among people living in rural areas with head injuries being the most common.[1] The largest retrospective chart review from Ireland reported a total of 130 farm-related injuries during a 7-year period with a total of four livestock related fatalities; of which in two cases, dismal outcomes were attributed to intracranial lesions inflicted by a cattle attack.[2] Horn-related cranial injury is another rarely described consequence of cattle attack, which can cause orbital and skull base damage resulting in vision loss and/or cerebrospinal fluid (CSF) leak. These complications place patients at increased risk for fatal meningitis or intracranial abscess and seizures as remote consequences.[3] Thus, early and adequate management is critical for patients presenting with animal-inflicted transorbital intracranial lesions. However, to the best of our knowledge, there are limited published data regarding identification and management of animal attack victims presenting with animal horn inflicted penetrating orbital lesion with associated skull base fracture and CSF leak.[34]
Here, we describe a male farmer who suffered a cow attack causing horn inflicted perforating orbital damage with concomitant comminuted frontobasal skull fracture and subsequent orbital and nasal CSF leakage.
CASE REPORT
A 35-year-old male farmer was transferred to the Ophthalmology Department from a rural hospital due to vision loss following cow's attack causing horn inflicted penetrating stabbing wound to his left eye. On admission, the patient complained of inability to see with his left eye, headache, and left cheek numbness. Ophthalmologic examination demonstrated complete left eye vision loss, hyphema, ruptured sclera, and dilated pupil. Noncontrast head computed tomography (CT) scan demonstrated comminuted fracture of the left superior orbital roof with intracranial displacement of free superior orbital roof fragments and 1.6 cm × 2.5 cm anterior cranial fossa defect [Figure 1]. In addition, frontal contusion areas, pneumocephalus and fractures of frontal and maxillary sinuses, and zygomatic arch were noted on admission head CT. He had no other associated injuries. He immediately underwent surgery, in which scleral defect with damaged lens and retina was removed; and lacerations were repaired. The next day, the patient complained of clear liquid dripping from his nose and left eye. For suspected nasal and orbital CSF leak, the patient was transferred to the Neurosurgery Department, where he was immediately placed on external lumbar drain and head CT with intrathecal contrast (omnipaque 240 – 9 ml) injection was performed. CT cisternography showed signs of CSF leakage into frontal and maxillary sinuses, nasal cavity, and left orbit [Figure 2]. CSF had normal cell count, nevertheless following microbiology consultation; the patient was started with prophylactic intravenous ceftriaxone 2 g t.i.d. The patient was discussed with the ear, nose, and throat service and the decision was made to perform revision, debridement, and repair of dural tear through bifrontal extradural approach. During the surgery, splintery fracture of orbital roof and internal wall of the frontal sinus as well as two irregular 0.5 cm × 1.0 cm and 2.5 cm × 1.5 cm dural defects were noted. Surgical debridement and removal of free bone fragments were performed followed by duroplasty using absorbable fibrin sealant patch and temporal muscle. Two days after the surgery, the patient was feeling well and there were signs neither of CSF leak nor pleocytosis. Therefore, external lumbar drain was removed and the patient was discharged home. At 1-year follow-up visit, there were no signs of CSF leak and noncontrast head CT demonstrated postoperative superior orbital roof defect.
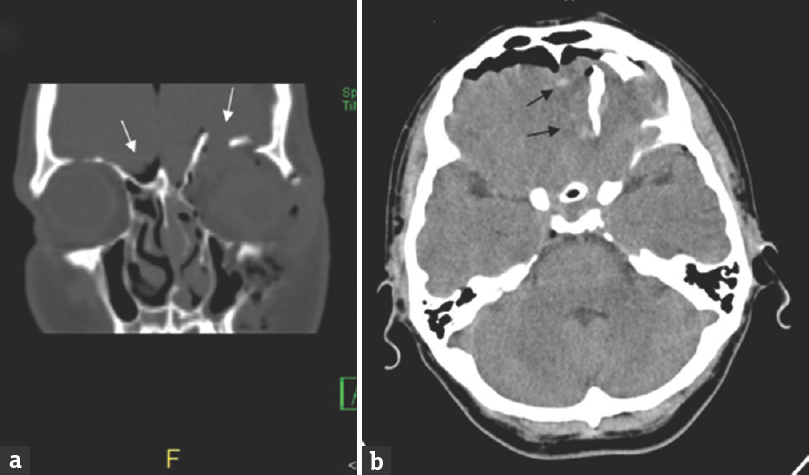
- Admission noncontrast head computed tomography scan demonstrating comminuted fracture of the left superior orbital roof with intracranial dislocation of superior orbital roof fragments and pneumocephalus in coronal plane (white arrows in a) with frontal lobe cerebral contusions in axial plane (black arrows in b)
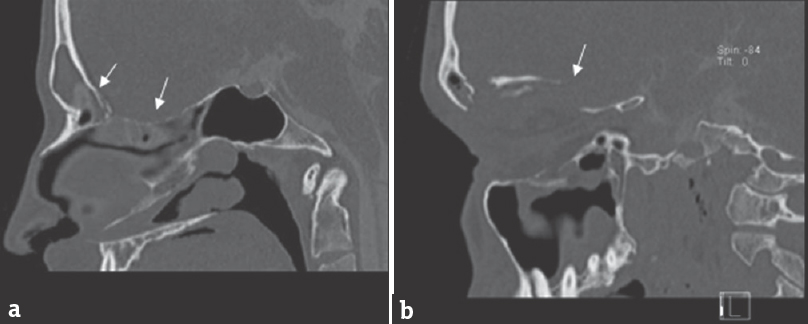
- Head computed tomography with intrathecal contrast injection demonstrating contrast leakage to frontal sinus, nasal cavity (a), and left orbit (b) (white arrows)
DISCUSSION
A recent retrospective large series by Caglayan et al. regarding animal-related injuries[1] reported that 29% of injuries were attributed to cow attack, with maxillofacial and cranial injuries comprising 44% and 18% of all injuries, respectively. To the best of our knowledge, there is limited published data regarding identification and management of transorbital perforating intracranial lesions inflicted by animal horn. We have identified two previously published case reports presenting perforating orbital injury associated with frontobasal skull fracture inflicted by a cattle's horn[3] and wild deer's antler[4] suggesting that frontobasal fractures should be suspected and carefully investigated in patients sustaining animal inflicted penetrating orbital injury since CSF leak and free intracranial bone fragments are associated with increased risk of meningitis, abscess, or seizures. Therefore, such injuries should be promptly identified and adequately managed to remove free bone fragments and close dural defect. In our case, orbital roof fracture with pneumocephalus and frontal contusions was documented on admission head CT, but the decision was made to admit the patient to ophthalmology service for immediate surgical repair of eye lesions. CSF leak was noted on the next day and prompted immediate neurosurgery consultation, external lumbar drainage, and CT cisternography.
In the present case, CSF leak was managed by performing duroplasty through bifrontal extradural approach because it allowed utmost exposure for removal of free bone fragments and repair of dural defects. In two previously published cases, the dural tears were also successfully managed through transcranial approach.[34] Endoscopic approach could be another viable option for isolated CSF rhinorrhea repair, but combined CSF leak with free intracranial bone fragments can be more reliably approached and managed through craniotomy.[5] Therefore, we consider that early transcranial approach is a viable option when managing patients presenting with penetrating transorbital injury associated with CSF leak because it allows careful inspection of intracranial lesions, removal of free intracranial bone fragments, and repair of dural tear(s). Because of medially and caudally displaced bone fragments and unknown size of expected irregularly shaped dural tear in the present case, minimally invasive approaches such as transorbital or supraorbital was outright rejected and bifrontal extradural approach was adopted because it allows the widest exposure to the anterior cranial fossae.
CONCLUSIONS
The presented case illustrates that frontobasal skull base fractures with dural tear causing CSF leak should be suspected in patients presenting with penetrating orbital damage inflicted by animal horn. Early duroplasty through craniotomy is an effective approach for CSF leak management and complication prevention.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Large animal-related injuries in a rural population in Northeastern Turkey. Indian J Surg. 2013;75:200-3.
- [Google Scholar]
- Farm-related trauma in the West of Ireland: An occupational hazard. Ir J Med Sci. 2014;183:601-4.
- [Google Scholar]
- Penetrating orbito-cranial and ocular cow-horn injuries. Niger J Clin Pract. 2007;10:177-9.
- [Google Scholar]
- An unusual case of a penetrating skull-base injury caused by a wild deer's antler. Cent Eur Neurosurg. 2009;70:48-51.
- [Google Scholar]
- A systematic review of the endoscopic repair of cerebrospinal fluid leaks. Otolaryngol Head Neck Surg. 2012;147:196-203.
- [Google Scholar]




