
Translate this page into:
Retrospective Analysis of Arthrodesis from Various Options after Anterior Cervical Discectomy
Address for correspondence: Dr. Vinaysagar Sharma, H. No. 1-218, Vaishanavi Gruha, Lower Lane, Station Bazaar, Kalaburagi - 585 102, Karnataka, India. E-mail: drvinaysagar@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Anterior cervical discectomy is a surgical procedure performed to treat a herniated/degenerated disc in the cervical region. There have been various studies comparing arthrodesis rates among various procedures. Our patients belonged to varied socioeconomic background and underwent anterior cervical microdiscectomy without/with instrumentation.
Aim:
The present study was performed to study and compare the arthrodesis rates in the patients operated for anterior cervical microdiscectomy with and without fusion/instrumentation procedures at our institution.
Materials and Methods:
This is a retrospective study performed at Vydehi Institute of Medical Sciences and Research Centre, Bengaluru. Pre- and post-operative X-rays were assessed in 96 patients who had undergone anterior cervical discectomy with/without fusion from June 2012 to June 2015. Radiographic arthrodesis was assessed in all patients. An arbitrary grading was designed by us and categorized into Grade I to IV. The criteria considered for adequate arthrodesis in this study were: (a) <2° movement on dynamic X-rays, (b) restored disc space height (±2 mm accepted), and (c) evidence of solid bone mass around disc space. Arthrodesis was categorized as Grade I if all the above 3 criteria on X-rays was fulfilled, Grade II if any 2 of the criteria was fulfilled, Grade III if any 1 of the criteria was fulfilled, and Grade IV when pseudoarthrosis/none of the criteria was fulfilled. Grade I arthrodesis was noted in about 79 patients (82.2%), Grade II in 14 patients, and only 3 patients had Grade III arthrodesis. There were no patients with absent arthrodesis/pseudoarthrosis.
Results:
Satisfactory arthrodesis was noted in 82% of the total patients, with patients undergoing fusion ± instrumentation procedure having better results.
Conclusions:
Arthrodesis by an interbody graft/implant with/without plating increases chances of success as compared to anterior cervical discectomy alone. Patients should be motivated for any of the available options for fusion/instrumentation
Keywords
Arthrodesis
cervical fusion
cervical microdiscectomy
fusion outcome

INTRODUCTION
Cervical spondylosis and disc herniation are common causes for neck pain and brachalgia.[1] Smith and Robinson described anterior cervical fusion for cervical spondylosis in 1955.[2] Fusion after discectomy aims to limit the motion, maintain the disc height, address neck pain, and maintains the normal cervical spine lordosis.[34] Instrumentation adds to the spinal stability and reduces risk of graft extrusion. Various arthrodesis techniques are available to restore the intervertebral height and cervical spine lordosis.[56]
A bone graft provides a favorable healing environment due to its relatively large surface area of cancellous bone. However, postoperative graft site pain is the most common complaint of the patient.[7]
To avoid the complications arising after bone harvesting, interbody fusion cages were devised to promote immediate stability of the cervical spine and promote arthrodesis. Various options include titanium spacers and cages, polyetheretherketone (PEEK) cages, combination of spacer and plates, hydroxyapatite, ceramics, biocompatible osteoinductive polymers, and bone morphogenetic protein.[789]
The purpose of this study was to evaluate the efficacy in terms of arthrodesis by various options available after anterior cervical discectomy.
MATERIALS AND METHODS
This study was performed at Vydehi Institute of Medical Sciences and Research Centre, Bengaluru. Over a period from June 2012 to June 2015, a total of 149 patients underwent 1 or 2 level anterior cervical discectomy without/with fusion (ACDF) ± instrumentation (ACDFI) using various options available and patient choice. Various options used were ACDF with stand-alone iliac bone autograft/hydroxyapatite G-bone/titanium cage and ACDF by iliac bone autograft/hydroxyapatite G-bone/titanium cage with titanium plate and Cage and plate combination titanium implant. Various options used for arthrodesis have already been existent and are proven methods for cervical fusion. Patients undergoing corpectomy, >2 level discectomy and posterior approaches for discectomy were excluded from the study. Postoperative anterior-posterior and lateral X-ray projections with dynamic flexion and extension X-ray views taken at 6 months and 1 year were analyzed. A maximum follow-up of 1 year was considered for the study to assess the arthrodesis. Due to financial restrictions, X-rays were the only investigation done in the postoperative and follow-up period for assessment of arthrodesis. Out of 149, 53 patients were lost to follow-up. Hence, only 96 patients have been included for the study analysis. X-rays of immediate postoperative period and at follow-up were compared. The criteria considered for adequate arthrodesis in this study were:
-
<2° movement on dynamic X-rays
-
Restored disc space height (±2 mm accepted) and
-
Evidence of solid bone mass around disc space.
Grades for arthrodesis were assigned accordingly. Arthrodesis was categorized as:
-
Grade I if all the above 3 criteria on X-rays was fulfilled
-
Grade II if any 2 of the criteria was fulfilled
-
Grade III if any 1 of the criteria was fulfilled
-
Grade IV when pseudoarthrosis/none of the criteria was fulfilled.
No pain questionnaire was done in the postoperative follow-up period as it was not a routine protocol at the institute during the study. Arthrodesis grades with various options were compared and analyzed.
RESULTS
The follow-up period was 12 months on an average. Mean age group noted was 45.67 years. A male preponderance was noted in the study (81.25%). Most of the patients presenting were manual laborers (29.6%).
C5–6 was the most common level involved (48.9%). C6–7 level being the next common level involved (56%) as shown in Table 1.

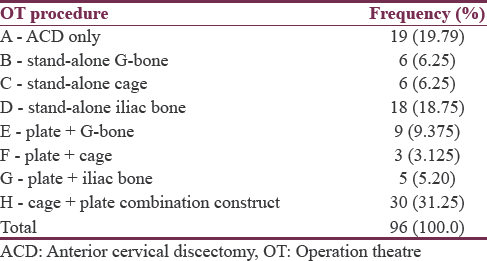
The most frequent procedure performed was anterior cervical discectomy with cage and plate combination interbody implant (31.25%) as shown in Table 2.
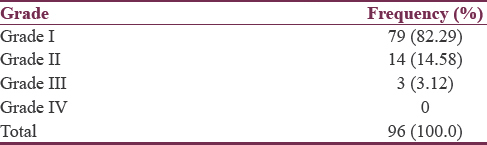
Grade I arthrodesis was noted in about 79 patients (82.2%), Grade II in 14 patients and only 3 patients had Grade III arthrodesis. There were no patients with absent arthrodesis/pseudoarthrosis as shown in Table 3.
DISCUSSION
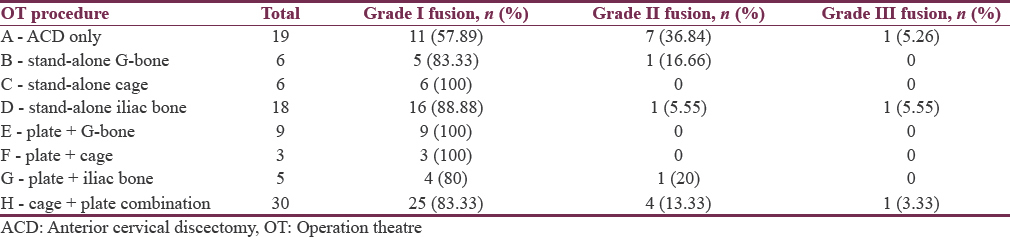
Cervical disc disease which is not responding to conservative treatment or associated with progressive/worsening neurological deficits demands surgical treatment.[10] Various fusion techniques have been described in the literature with usually a good outcome.[268910] ACD alone was favored for its simplicity, low cost, and absence of the autograft/implant-related complications. Fusion procedure is believed to have better results than the ACD alone as shown in Tables 4 and 5.[11]

Oktenoglu et al. in their series of 20 patients comparing ACD alone with ACDF with iliac graft and plate insertion showed 69% reduction in disc height at a follow-up of 1 year. Out of 11 patients of ACD only, 6 patients had a reduction in disc height.[3] In our series, anterior cervical discectomy alone without any fusion procedures were performed in 19.79% cases (19 patients) in view of low cost and not consenting for iliac bone graft harvest. Out of 19 cases operated for ACD only, Grade II arthrodesis was seen in 7 patients of whom disc height was reduced in 4 patients, and 3 patients had >2° movement on flexion-extension views. One patient had a Grade III arthrodesis showing a lack of solid bone mass and a reduced disc space.
ACDF was advocated to prevent disc space collapse, stabilization of cervical architecture, and promote bony fusion. Iliac crest autograft has been used for the interbody fusion.[26] Autograft showed 65% successful fusion rate in a study by Kim et al.[12] Iliac crest autograft appears to be the gold standard when the fusion of the motion segment is considered for pain relief and functional improvement.[13] Anterior cervical interbody fusion is complimented by anterior cervical plating to maintain sagittal balance more effectively and increase fusion rates by immobilizing the segment.[11] In our series, among the 18 patients who underwent ACDF with stand-alone iliac bone graft, reduced disc height was noted in 2 patients with one among them also having a lack of solid bone mass around disc space (1 patient of Grade II and 1 of Grade III arthrodesis). One patient among the five patients undergoing ACDF by iliac bone graft and plating had a lack of solid bone mass around disc space (Grade II arthrodesis) with no patient showing disc space reduction.
In a study by Samartzis et al., a total of 69 patients undergoing ACDF by iliac autograft with/without plating were analyzed. Sixty-six patients (95.7%) achieved a solid fusion (100% non-plated; 90.3% plated). Nonunions were noted in the three patients with instrumentation. No statistically significant difference in fusion rates (P > 0.05) was observed between nonplating and plating groups.[14] In our series, ACDF by iliac autograft with plating had one patient of improper fusion and two patients in stand-alone iliac autograft group as described above.
Considering harvesting complications such as peripheral nerve injury, prolonged pain, wound infection, hematoma and cosmetic deformity, and alternative interbody implants were introduced into practise.[2611] Hydroxyapatite and tricalcium phosphates (ceramics), titanium disc spacers/cages, biopolymers, tantalum blocks, cylindrical titanium mesh, and polymethyl-methacrylate started getting used as interbody implants.[11]
Bruneau et al. had 99% (67 of 68 operated levels) complete interbody fusion in their study of ACDF by hydroxyapatite with plate system.[10] In our series, out of 6 cases of stand-alone hydroxyapatite graft, only 1 patient had (Grade II arthrodesis) >2° movement on flexion-extension views and among 9 patients with hydroxyapatite graft and plating 100% Grade I arthrodesis was noted.
According to Jacobs et al. cage would be a gold standard when fusion rates are ignored, and complication rates are considered.[13] Although solid fusion is achieved by stand-alone titanium cages, they have failed to preserve the disc space height and preserve a natural intervertebral alignment.[15] Stand-alone PEEK cages have a risk of subsidence, but clinical outcomes and fusion rates are good enough.[16] Cabraja et al. noted a solid arthrodesis in 93.2% of cases in Titanium cage group and 88.1% of cases in PEEK cage group. A good lordotic correction can be achieved by both the cage types. Hence, they remarked that clinical and radiological outcomes are not influenced by the type of graft in ACDF by Titanium/PEEK cages.[17] In our study, ACDF with stand-alone cage (PEEK/Titanium) has achieved a 100% Grade I arthrodesis in all the 6 cases.
In a study by Saoud and Mashally, 100% fusion in both ACDF with stand-alone cage (50 cases) and ACDF with cage and cervical plating group (50 cases) was observed. However, cage subsidence of 52% was noted in the former group and 12% in the latter group at a follow-up of 18 months.[9] In our series, both groups of cage with/without plating, Grade I arthrodesis in 100% of the total cases: six and three cases, respectively (total 9) was achieved.
A Keogh et al. used a cage and plate combination implant in their study. Twenty-three patients were available for their complete study, and all had complete bone union or evidence of stability.[8] Among the ACDF cases in our series, the maximum number of patients underwent ACDF by cage and plate combination construct (31.25%) considering the low cost of the implant and the technical ease in usage. Twenty-five patients (83.33%) with Grade I arthrodesis, four patients with Grade II arthrodesis (lack of solid bone mass around disc space), and one patient with Grade III arthrodesis (lack of solid bone mass around disc space and reduced disc space height) were noted in the above-mentioned category.
Lee et al. found fusion rates of 87.1% in iliac autograft with plating group, 79.5% in cage plus plate group, and 63.2% in the cage alone group.[18] Xie and Hurlbert compared anterior cervical discectomy alone with ACDF and ACDFI and found the fusion rates of 67%, 93%, and 100% in ACD, ACDF, and ACDFI groups, respectively.[19]
Almost 82% out of the total patients in the present series had a satisfactory Grade I arthrodesis. Pseudoarthrosis was not seen in any of the patients in the series. ACD with fusion by interbody titanium/PEEK cage with/without anterior cervical plating and ACD with interbody G-bone with cervical plating had 100% Grade I arthrodesis though the number of cases in each category was relatively small. About 83.33% of patients who underwent ACDF by the cage and plate combination implant had Grade I arthrodesis.
Grade II arthrodesis was seen the maximum in only ACD cases (36.84%) and the least in iliac bone stand-alone graft cases (5.5%).
Considering Grade II and Grade III as inadequate arthrodesis, nearly, half (42%) of the ACD only group had inadequate arthrodesis. On the other hand, other techniques of arthrodesis were all comparable in terms of improper arthrodesis (11%–20%) rates showing no significant difference between the techniques.
The drawback of this study is that it is retrospective in nature and hence randomization was not done.
CONCLUSIONS
Arthrodesis by an interbody graft/implant with/without plating increases chances of success as compared to anterior cervical discectomy alone. As most of the patients are from rural areas and of low economic status, patients should be counseled and motivated for any form of fusion option to have a better outcome.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Anterior cervical fusion by the smith-Robinson approach. J Neurosurg. 1968;29:397-404.
- [Google Scholar]
- Cervical spine surgery: An historical perspective. Clin Orthop Relat Res. 2011;469:639-48.
- [Google Scholar]
- Anterior cervical microdiscectomy with or without fusion. J Spinal Disord Tech. 2007;20:361-8.
- [Google Scholar]
- Anterior discectomy and fusion for the management of neck pain. Spine (Phila Pa 1976). 1999;24:2224-8.
- [Google Scholar]
- Sagittal cervical alignment after cervical disc arthroplasty and anterior cervical discectomy and fusion: Results of a prospective, randomized, controlled trial. Spine (Phila Pa 1976). 2009;34:2001-7.
- [Google Scholar]
- Outcomes following anterior cervical discectomy and fusion: The role of interbody disc height, angulation, and spinous process distance. J Spinal Disord Tech. 2005;18:304-8.
- [Google Scholar]
- Bone graft substitutes in anterior cervical discectomy and fusion. Eur Spine J. 2009;18:449-64.
- [Google Scholar]
- Anterior cervical fusion using the intExt combined cage/plate. J Orthop Surg (Hong Kong). 2008;16:3-8.
- [Google Scholar]
- A comparative study of ACD with peek stand alone cervical cages versus cage and plate fixation, study of 100 patients. World Spinal Column J. 2012;3:1-6.
- [Google Scholar]
- Anterior cervical interbody fusion with hydroxyapatite graft and plate system. Neurosurg Focus. 2001;10:E8.
- [Google Scholar]
- Surgical management of cervical disc disease: From no fusion to fusion and back again. Clin Neurosurg. 2005;52:331-7.
- [Google Scholar]
- An early comparative analysis of the use of autograft versus allograft in anterior cervical discectomy and fusion. Korean J Spine. 2012;9:142-6.
- [Google Scholar]
- Systematic review of anterior interbody fusion techniques for single- and double-level cervical degenerative disc disease. Spine (Phila Pa 1976). 2011;36:E950-60.
- [Google Scholar]
- Does rigid instrumentation increase the fusion rate in one-level anterior cervical discectomy and fusion? Spine J. 2004;4:636-43.
- [Google Scholar]
- Anterior cervical arthrodesis using a “stand alone” cylindrical titanium cage: Prospective analysis of radiographic parameters. Spine (Phila Pa 1976). 2010;35:1545-50.
- [Google Scholar]
- Anterior cervical discectomy and fusion using a stand-alone polyetheretherketone cage packed with local autobone: Assessment of bone fusion and subsidence. J Korean Neurosurg Soc. 2013;54:189-93.
- [Google Scholar]
- Anterior cervical discectomy and fusion: Comparison of titanium and polyetheretherketone cages. BMC Musculoskelet Disord. 2012;13:172.
- [Google Scholar]
- Comparative analysis of 3 different construct systems for single-level anterior cervical discectomy and fusion: Stand-alone cage, iliac graft plus plate augmentation, and cage plus plating. J Spinal Disord Tech. 2013;26:112-8.
- [Google Scholar]
- Discectomy versus discectomy with fusion versus discectomy with fusion and instrumentation: A prospective randomized study. Neurosurgery. 2007;61:107-16.
- [Google Scholar]




