
Translate this page into:
The clinical profile, management, and overall outcome of aneurysmal subarachnoid hemorrhage at the neurosurgical unit of a tertiary care center in India
Address for correspondence: Dr. Rajesh Chhabra, Department of Neurosurgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India. E-mail: drrajeshchhabra@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background and Purpose:
Several studies report good outcomes in selected patients of aneurysmal subarachnoid hemorrhage (aSAH). The purpose of our study is to project the clinical characteristics, management, and overall outcome of patients with aSAH presenting to a tertiary care center in India.
Materials and Methods:
A prospective study was conducted over a period of 10 months and all patients presenting with aSAH were studied. Patients presenting in all grades and managed with any type of intervention or managed conservatively were included to characterize their clinical and radiological profile at admission, during management, and at discharge. Outcome was assessed with the Glasgow Outcome Score (GOS) at 3 months follow-up.
Results:
Out of the 482 patients [mean age: 51.3 (±13.5); M: F = 1:1], 330 patients were fit to be taken up for intervention of the ruptured aneurysm, while 152 patients were unfit for any intervention. At 3 months follow-up, good outcome (GOS 4 and 5) was observed in 159 (33%), poor outcome (GOS 2 and 3) in 53 (11%), and death in 219 (45.4%) patients, while 51 patients (10.6%) were lost to follow-up. Most (95%) of the patients in the non-intervention group expired, and hence the high mortality rate, as we have analyzed the results of all patients of all grades, regardless of the treatment given. The predictors of poor outcome (GOS 1, 2, and 3) at 3 months follow-up, using multinomial regression model, were: World Federation of Neurological Surgeons (WFNS) grade IV and V (at admission and after adequate resuscitation) [odds ratio (OR): 35.1, 95% confidence interval (CI): 10.8-114.7] and presence of hypertension as a co-morbid illness [OR: 2.7, 95% CI: 1.6-5.6]. All patients showing acute infarction on computed tomography scan at presentation had a poor outcome.
Conclusions:
Despite recent advances in the treatment of patients with aSAH, the morbidity and mortality rates have failed to improve significantly in unselected patients and natural cohorts. This may be attributed to the natural history of aSAH, and calls for new strategies to diagnose and treat such patients before the catastrophe strikes.
Keywords
Intracranial aneurysm
overall outcome
subarachnoid hemorrhage

Introduction
During the last three decades, newer diagnostic techniques and treatment strategies have been developed for patients with aneurysmal subarachnoid hemorrhage (aSAH), leading to a decrease in the case fatality by 0.6% per year.[1] However, the case fatality rate for aSAH is still reported between 8.3 and 66.7%, with most patients dying as a result of the initial bleed or its immediate complications.[123] Thus, aSAH remains a devastating disease, carrying with it a mortality rate of 12% before receiving medical attention, an additional mortality of 40% within 1 month of admission to hospital, and 30% morbidity among the survivors.[45]
There are several reports from India of the outcome after surgical clipping or coiling of aneurysms, but few reports present the overall outcome of all patients with aSAH.[678] The purpose of this study was to describe the characteristics, management, and outcome of patients with aSAH presenting to a tertiary care center in India.
Materials and Methods
Study design and patient population
A prospective cohort study was conducted during a period of 10 months at our institute. The study was approved by the Institutional Ethics Committee and a written informed consent was taken from all patients or their next of kin, as applicable.
Inclusion criteria
All patients, of all age groups, who presented to our institute with aSAH were included in the study.
Exclusion criteria
Patients with SAH due to any other cause, for example, due to trauma, intracranial arterio-venous malformations, hypertension, coagulopathy, etc., were excluded.
Pre-intervention assessment
All patients included in the study were assessed on presentation in the neurosurgical emergency unit of our institute. The age, sex, presentation interval (interval from ictus to presentation at our institute), Glasgow Coma Scale (GCS) score, World Federation of Neurological Surgeons (WFNS) grade, and co-morbid illnesses of the patients were recorded after adequate resuscitation and hemodynamic stabilization. Computed tomography (CT) scan done on presentation or done at a primary hospital (before referral to our institute) was evaluated, and the Fisher grade and presence of hydrocephalus or acute infarction (related to SAH-associated vasospasm) were noted. The baseline work-up and pre-anesthesia check-up was done in all patients, and they were optimized for the intervention.
As per the standard of care in most experienced neurosurgical centers, early intervention was carried out in good-grade patients, with deferred treatment used for poor-grade patients.[9] At our institute, we defined good-grade patients as those with WFNS grade I, II, and III on clinical assessment after complete resuscitation and optimization of the patient. All cases who presented in unconscious status were first intubated, oxygenated, and hydration was given in order to establish a urine output of more than 50 ml/h. We follow the dictum that close monitoring for a change in the patient's grade, over the first 24 h after hospitalization, is mandatory in patients whose poor grade is primarily because of the SAH and helps to determine the appropriateness of surgery.[1011] The poor-grade patients, whose decreased consciousness was attributed to intracerebral hemorrhage (ICH), subdural hematoma (SDH), or hydrocephalus, were taken up for surgical intervention for alleviating the raised intracranial pressure, prior to clipping or coiling of the aneurysm. Based on the above criteria, the patients were divided into intervention and non-intervention groups.
All patients underwent four-vessel cerebral CT angiography on the basis of suspicion of aSAH in the plain CT. Four-vessel digital subtraction angiography (DSA) was done for those patients in whom CT angiography was negative or in whom further information with respect to aneurysmal configuration and spatial orientation was desired by the treating neurosurgeon.
Depending on the clinical and radiological features of the patients, those in good grade were taken up for early intervention (<24 h), in order to occlude the offending aneurysm and prevent re-bleed. The choice of intervention (microsurgical clipping vs. endovascular coil embolization) was governed by various factors like aneurysm location, aneurysm characteristics, expertise and preference of the treating neurosurgeon, and affordability of the patient. Being a tertiary care center in North India, mainly treating patients from low socioeconomic strata, the affordability of the patients was an important consideration in the choice of intervention.
The patients in the poor grade were managed conservatively with supportive measures, including ventilator support (if required), and observed for improvement in clinical status. Any cause for poor neurological status was addressed; for example, hydrocephalus was managed with either a ventriculoperitoneal shunt or external ventricular drainage. If they improved to good grade, these patients were then taken up for intervention. If they did not show improvement, they were managed accordingly in the hospital or referred to the primary care hospital.
Intervention
Depending upon the location of the aneurysm, standard microsurgical techniques were used to treat intracranial aneurysms. The aneurysms were clipped with Aesculap or Sugita titanium aneurysm clips. All surgeries were performed by the neurosurgical consultants at our institute. The duration of surgery, temporary clipping time, occurrence of intraoperative rupture, and any complications were recorded.
The patients in good grade, who were amenable to the endovascular approach and could afford the cost of treatment, were taken up for transfemoral endovascular coiling with Guglielmi detachable coils under standard fluoroscopic guidance. Balloon or stent-assisted coiling was employed, whenever necessary.
Post-intervention management
After the surgical or endovascular procedure, the patients were transferred to the neurosurgical ICU or high-dependency unit in the ward, depending upon the clinician's assessment of the neurological status of the patient, and followed daily from immediate postoperative period till hospital discharge or death.
The patients were assessed in the post-procedural state for their neurological status using GCS score. The length of hospital stay for each patient was noted. Any complication during the post-procedural period in the form of vasospasm, re-bleed, development of hydrocephalus, or any medical complication like pneumonia, myocardial dysfunction, septicemia, etc., was noted.
All patients were assessed with the Glasgow Outcome Score (GOS) at discharge and at 3 months follow-up visit in the out-patient clinic. Any focal neurological deficits were noted separately. The patients in the non-intervention group were followed in the out-patient clinic or through telephonic interview with relatives. For patients who could not be contacted still, questionnaires were sent to their postal addresses.
Outcome definitions
The outcome of all patients was assessed by GOS at 3 months after presentation to our institute.[12] Good outcome was defined as those patients in GOS 4 and 5, while poor outcome was defined as those patients in GOS 1, 2, and 3. In-hospital mortality was assessed as a clinical outcome measure, and the cause of death was noted for all cases of mortality.
Statistical analysis
Data are presented in descriptive form as either mean (±SD) or median [interquartile range (IQR)] in normally distributed and skewed variables, respectively. Normalcy of data was checked using Kolmogorov–Smirnov test. For normally distributed data, means were compared using unpaired Student's “t” test for two groups. For skewed data, Mann–Whitney test was applied. Qualitative or categorical variables were described as frequencies and proportions. Proportions were compared using Chi-square or Fisher's exact test, whichever was applicable. Logistic regression analysis was performed to describe the variables associated with the occurrence poor outcome in cases of aSAH. All statistical tests were two-sided and a probability value <0.05 was taken as significant.
Results
Study population
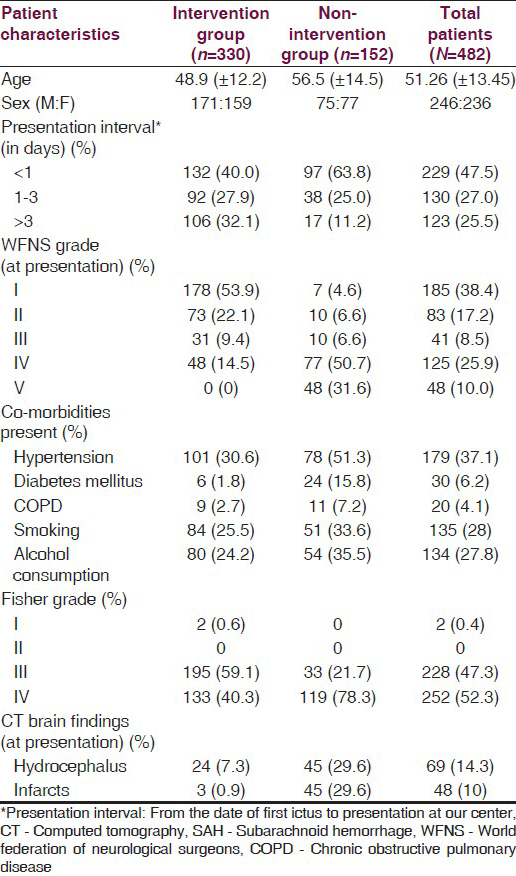
During the study period of 10 months, 482 patients of aSAH presented to the emergency neurosurgical unit of our hospital. The mean (±SD) age of the patients was 51.3 years (±13.4). The male: Female ratio was nearly 1:1. Depending on whether intervention was undertaken or not, the patients were divided into intervention and non-intervention groups. Three hundred and thirty patients underwent definitive intervention for the ruptured aneurysm, while 152 patients were managed with supportive care. In the intervention group, the ruptured aneurysm was located on the anterior cerebral artery in 145 (43.9%) patients, on the middle cerebral artery in 80 (24.2%) patients, at the internal carotid artery bifurcation in 31 (9.4%) patients, on the supraclinoid internal carotid artery in 49 (14.8%) patients, and in the posterior circulation in 25 (7.6%) patients. The percentage of patients in the intervention group with multiple aneurysms was 12.1%.
In the intervention group, 93% (307/330) underwent surgical clipping, while only 7% (23/330) underwent endovascular coiling. In the non-intervention group, 82% patients were in WFNS IV and V after resuscitation and 78% patients had Fisher grade IV SAH on CT scan. The severity of SAH and inability of these patients to recover after the initial insult meant that we could not undertake any intervention in them. The baseline characteristics of the intervention group, the non-intervention group, and the entire study group are presented in Table 1. Out of the 482 patients, 51 patients were lost to follow-up at 3 months.
Analysis of outcome at discharge/death
(a) Intervention group (330 patients): Out of the 307 patients who underwent surgical clipping of the aneurysm, 142 patients (46.3%) were conscious without any neurological deficit, 48 patients (15.6%) were conscious but had neurological deficits, and 52 patients (16.9%) were unconscious; while 65 patients (21.2%) expired. Thus, overall mortality in the surgical clipping group at discharge was 21.2%. Mortality in patients with WFNS grade I and II SAH was 14.2 and 16.2%, respectively [Table 2]. Out of the 230 patients in WFNS grade I and II at presentation, 11% had multiple aneurysms, 6.7% had posterior circulation aneurysms, and 7% had complex/giant aneurysms. In many of the patients, endovascular coiling was considered as the first treatment option, but these patients had to be operated upon due to financial constraints.
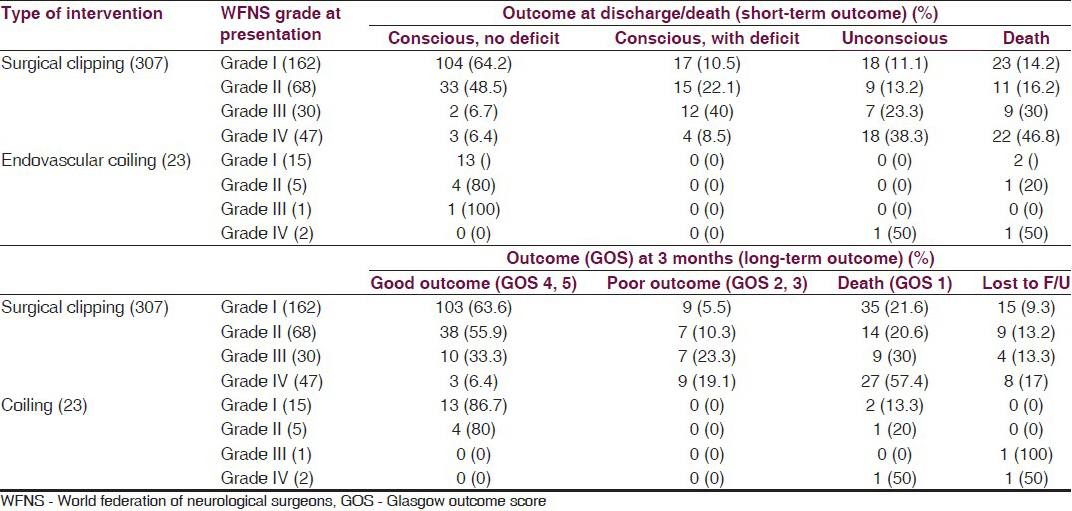
Seventy-five percent of patients in WFNS grade I and 71% of patients in WFNS grade II were conscious at discharge and were classified as having a good outcome. The percentage of patients having a good outcome at discharge decreased to 46.7% in WFNS grade III patients and to 15% in WFNS grade IV patients.
Only 23 patients out of the 330 patients in the intervention group underwent endovascular coiling. Out of these 23 patients, 18 patients (78.3%) were conscious without any neurological deficit and 1 patient (4.3%) was unconscious, while 4 (17.3%) patients expired. In this small subgroup, 13 out of 15 patients with WFNS grade I aSAH and 4 out of 5 patients with WFNS grade II aSAH were conscious with no neurological deficit at discharge. Mortality was reported in 2 out of 15 patients with WFNS grade I aSAH and in 1 out of 5 patients with WFNS grade II aSAH. One patient presenting in WFNS grade III had a good outcome, while out of two patients presenting in WFNS grade IV, one patient was discharged in an unconscious state and the other one expired.
(b) Non-intervention group (152 patients): Mortality was reported in 117 (76.9%) patients in this group during the hospital stay. The remaining 35 patients in the group either left against medical advice or were shifted in an unconscious state to a peripheral hospital for supportive care. Before shifting these patients, they were medically managed and supportive care was given in a high-dependency set-up. These patients failed to show any neurological improvement and remained in poor grade for an average of 10-15 days. These patients were then shifted to the peripheral hospital with the advice that they should come back to our tertiary center for neurosurgical intervention, if they improved to conscious state.
Analysis of outcome at 3 months follow-up
(a) Intervention group (330 patients): Out of the 307 patients who underwent surgical clipping, 154 patients (50.2%) had a good outcome (GOS 4, 5), 32 patients (10.4%) had a poor outcome, and 85 patients (27.7%) expired, while 36 patients (11.7%) were lost to follow-up. The mortality rate increased from 21.2% at discharge to 27.7% at 3 months follow-up.
Out of the 23 patients who underwent endovascular coiling for treatment of the aneurysm, 17 patients (73.9%) had a good outcome (GOS 4, 5) and 4 patients (17.4%) expired, while 2 patients (8.6%) were lost to follow-up.
The outcome at 3 months follow-up in the intervention group, with respect to each WFNS grade at admission, is detailed in Table 2.
(b) Non-intervention group (152 patients): The mortality rate increased from 76.9% at the end of hospital stay to 85.5% at 3 months follow-up. Out of the remaining 22 patients, 9 patients were lost to follow-up, while 12 were still in GOS 2 and 3 and, hence, could not be taken up for neurosurgical intervention.
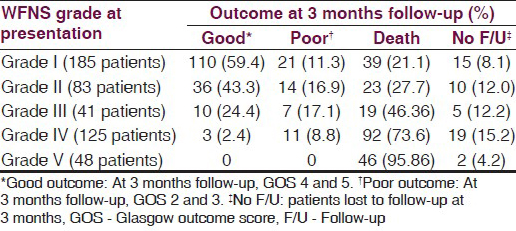
(c) Overall outcome of the study group: At 3 months follow-up, out of the 482 patients, only 159 patients (33%) were functionally independent at 3 months follow-up. Poor outcome was seen in 272 patients (56.4%) and 51 patients were lost to follow-up. The overall mortality in the study group was 219 patients (45.4%). Table 3 details the overall patient outcome with respect to the WFNS grade at presentation.
Mortality in the study group
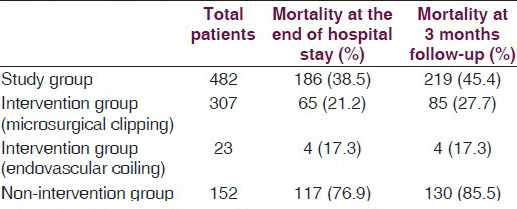
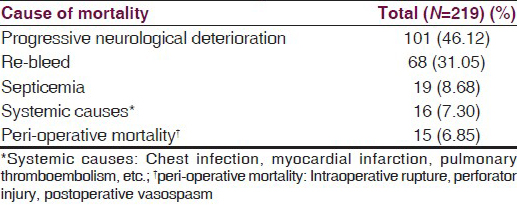
The mortality rate in our study group was 45.4% (219/482) at 3 months follow-up. The mortality rate in the intervention group was 26.9% (89 out of 330 patients), while it was 85.5% (130 out of 152 patients) in the non-intervention group [Table 4a]. Out of the 219 patients who expired at 3 months follow-up, 60% were in the non-intervention group; thus, the high mortality rate in the non-intervention group was responsible for the majority of deaths. We attribute the high mortality to the fact that one-third of our patients with aSAH were not fit for any intervention and died of the primary disease/event. In the intervention group, at short-term (at the end of hospital stay) follow-up, the mortality rate was 20.9% (69 out of 330 patients), while at 3 months follow-up, the mortality rate was 26.9%. Majority of these 20 deaths between discharge and 3 months follow-up can be attributed to those patients who were discharged in an unconscious state and succumbed to secondary medical problems like chest infections, pulmonary thromboembolism, septicemia, etc., In the entire study group, the most common cause of death in our study population at 3 months follow-up was progressive neurological deterioration in 101 patients, followed by re-bleed of the aneurysm seen in 68 patients. The causes of mortality with their respective percentages are presented in Table 4b.
Factors affecting the outcome of aSAH
The following variables were studied for their association with poor outcome of aSAH at 3 months follow-up: Age, sex, ictus-to-presentation interval, WFNS grade at presentation, presence of co-morbidities [hypertension, diabetes mellitus, chronic obstructive disease, chronic smoking habit (smoking index >100), alcohol consumption], Fisher grade at presentation, hydrocephalus, and acute infarction (related to SAH-associated vasospasm) in the CT scan at presentation.
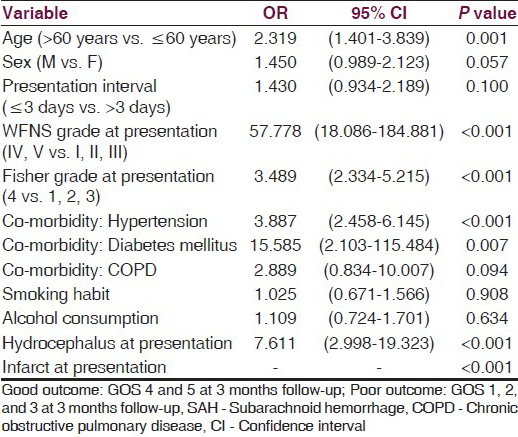
Univariate analysis showed that out of the 12 variables studied, occurrence of poor outcome in patients of aSAH was associated with the following: Age >60 years, WFNS grade (at admission and after adequate resuscitation) >III, Fisher grade at presentation >III, hypertension, diabetes mellitus, and hydrocephalus on CT scan at presentation. The odds ratios (ORs) for the variables along with the 95% confidence interval (CI) values and the P values are given in Table 5. In our study, 48 patients out of the 482 patients presented with acute infarction on the CT scan at presentation. All 48 patients had a poor outcome at 3 months follow-up. Hence, acute infarction seen on the pre-intervention CT scan was associated with poor outcome in our study.
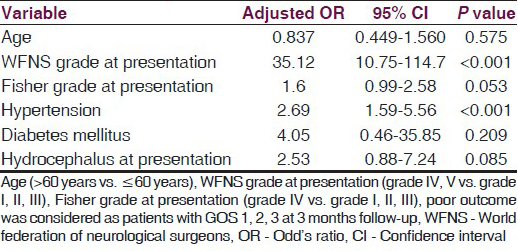
Multinomial regression model identified the variables predicting poor outcome, taking into consideration those variables that were significant (i.e., associated with poor outcome) in univariate analysis. Only WFNS grade (at admission and after adequate resuscitation) and presence of hypertension as a co-morbid illness were found to be predictors of poor outcome [Table 6].
Discussion
Despite causing only 5-10% of strokes, aSAH challenges the healthcare system as it is associated with a high early case fatality rate, and many survivors are left in a functionally dependent state. Over the past few decades, new diagnostic techniques, advances in neuroanesthesia, and technical advances in surgical clipping and endovascular coiling have revolutionized the treatment of aSAH.[2] Even with these developments in detection and management of aSAH, multicentric trials from developed countries show that the case fatality rates have not changed accordingly.[113]
The healthcare systems in developed countries have put into effect registries to detect cases of stroke and a referral system to effectively provide the best possible care at the designated centers.[13] However, developing countries like India still lag behind in establishing such facilities for their vast population. In an attempt to get an idea of the fate that befalls the patients of aSAH in our country, we studied the profile and outcome of patients presenting to a high-volume center for aneurysmal surgery in North India.
This is not a population study, but simply an analysis of patients presenting with a single disease entity to a tertiary care center. Our institute is a central government institute located in Chandigarh and we receive patients from the surrounding states of Punjab, Himachal Pradesh, and western Haryana. Majority of the cases of aSAH are referred to our center from this region of North India. Some good-grade patients are now being operated at peripheral centers, and possibly some poor-grade patients do not make it to our center. Thus, our study includes patients representing the overall patient population experiencing aSAH in this part of India. Such studies are required from developing countries as the meta-analyses reported in literature do not represent such countries and, hence, do not truly reflect the burden of disease in the world and the morbidity and mortality associated with it.[14]
Analysis of outcome
Analysis of the entire study group revealed a good outcome in 32.9% patients (159/482), poor outcome in 11% patients (53/482), and mortality in 45.4% patients (219/482), and 51 patients (10.5%) were lost to follow-up at 3 months. As mentioned in the Results section, in almost one-third of the patients presenting to us with aSAH, no intervention could be undertaken due to persistent poor neurological status even after adequate resuscitation and stabilization. This contributed significantly to the overall outcome of our study. Also, about 15% of patients undergoing surgery had WFNS grade IV aSAH and mortality in this subgroup was nearly 50%. This was one of the contributing factors for the overall high mortality.
High mortality in the intervention group could also be attributed to medical morbidities in the postoperative period such as septicemia, pneumonia, and pulmonary thromboembolism. Medical morbidities, especially pneumonia, have been documented as a significant cause of morbidity and mortality in patients of aSAH.[15] In addition to the above-mentioned factors, only 7% of patients (23/330) in the intervention group underwent coiling because of the poor socioeconomic strata of the patients. In most of the centers in the world, the percentage of patients undergoing coiling varies from 10 to 60%.[161718] Therefore, patients in whom the first option was coiling because of the location/complex nature of the aneurysm had to be surgically clipped. This contributed to the overall outcome and morbidity. There were some patients who refused surgery, even though they were in good grade, while very few patients did not undergo intervention due to complex aneurysmal anatomy (not amenable to surgery), coupled with non-affordability for coiling. In overall assessment of the disease outcome, it is important to include these patients, so as to get a complete picture.
We lost 51 patients (10.59%) to follow-up at 3 months. Few patients, operated in good grade and discharged in GOS 5, never came to us again after the first follow-up at 15 days. The reason may be that they lived in remote areas. Some of the poor-grade patients refused treatment at our hospital in view of the poor prognosis, and may have expired at home.
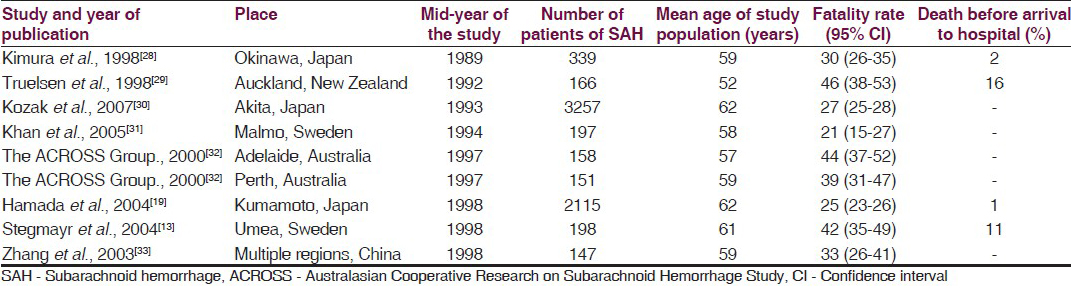
In population-/hospital-based studies available from 1972 to 2002, the case fatality rates range from 17 to 54%.[213] Langham et al., in their study of SAH in neurosurgical units in the United Kingdom and Ireland, reported an unfavorable outcome in 38.5% patients (34.6% in repaired and 81% in unrepaired patients) at 6 months follow-up.[16] Hamada et al., in their study from Japan, stated that out of the 1634 surgically treated patients, only 70.6% had a good outcome, while out of the 477 conservatively treated patients, only 5.7% had a favorable outcome.[19] In the meta-analysis of population-based studies by Nieuwkamp et al., the case fatality rates range from 8.3 to 66.7%, with the majority being more than 40%.[1] As shown in Table 7, the population-based and hospital-based studies performed during the time period 1985-2005 show that the case fatality rates for aSAH range from 21 to 46%.
There is hardly any large series available from India analyzing the overall outcome of patients with aSAH. Most of the studies available have focused on results in specific subsets of aSAH, and most of the studies mention the peri-operative morbidity and mortality. It is important to have data available about the outcome of all patients of aSAH, including patients with poor grade, patients who could not be operated or coiled, as well as those patients who did not opt for any treatment.
Our study emphasizes the need to detect and treat aneurysms before they rupture and to protect the brain from the adverse effects of SAH through new strategies.[4] The only reasonable way of preventing or reducing the morbidity and mortality related to SAH is to secure the aneurysm before it ruptures. Screening programs with relatively non-invasive modalities like CT or MR angiography would be required for the purpose.
Analysis of mortality in our study group revealed progressive neurological deterioration as the most common cause of death, followed by re-bleed of the aneurysm. Vasospasm as a cause of deterioration was included in this group. Broderick et al., in their population study, concluded that insult of the initial hemorrhage is the most common cause of mortality, followed by re-bleed of the aneurysm.[20] As per the International Cooperative Study on the Timing of Aneurysm Surgery, vasospasm and re-bleeding were the leading causes of morbidity and mortality, in addition to the initial bleed.[21] Our study again underlies the negative impact of the initial insult of SAH on the outcome.
Factors affecting the outcome of aSAH
We analyzed the factors affecting the outcome in order to determine those factors that could predict poor outcome in patients presenting to our institute. With the multinomial regression model [Table 5], WFNS grade IV, V (at admission and after adequate resuscitation) (Odd's ratio [OR]: 35.12, 95% CI: 10.75-114.7, P < 0.001) and presence of hypertension as a co-morbid illness (OR: 2.69, 95% CI: 1.59-5.56, P < 0.001) were predictors of poor outcome in our patients. All patients with acute infarction on the presenting CT scan had poor outcome in our study, and hence, this factor was highly significant as a predictor of poor outcome (OR could not be calculated, P < 0.001).
WFNS grade at presentation
Literature clearly states that WFNS grade at presentation is the most important predictor of outcome, and this held true in our study. Chiang et al., on studying 56 consecutive patients for prediction of outcome in aSAH, found the patient's worst clinical grade to be most predictive of the outcome, especially when the patient is assessed using the WFNS scale or the GCS.[22] The International Cooperative Study on the Timing of Aneurysm Surgery by Kassell et al. observed that WFNS grade had a direct correlation with the outcome of aSAH.[21] In the analysis by Broderick et al., using death or total dependence at 30 days as the outcome variable, only age and the WFNS score were significant predictors of outcome.[20]
Hypertension
The presence of hypertension as a co-morbid illness was predictive of poor outcome in our study population. Hypertension is associated with increased risk of SAH and is also associated with poor outcome in patients of aSAH. Feigin et al., in their study, concluded that smoking, hypertension, and excessive alcohol remain the most important risk factors for SAH.[23] Kassell et al. reported that both the patient's condition at the time of presentation and the postoperative results are adversely affected by the presence of hypertension.[21] Juvela et al., in a recent study, stated that hypertension is a risk factor for poor outcome and cerebral infarction after aSAH.[24]
Infarction on CT scan at presentation
In our study, none of the patients having acute infarction on the presenting CT brain were functionally independent at 3 months follow-up. Lagares et al. analyzed the data obtained from 294 consecutive cases of aSAH and determined that outcome was related to the presence of hypodensities on CT scan.[25] Rosengart et al. observed that cerebral infarction was the most important factor associated with outcome in patients with SAH.[26] Vergouwen et al. stated that cerebral infarction after subarachnoid hemorrhage contributes to poor outcome by vasospasm-dependent and -independent effects.[27] [33]
Conclusion
The entity of aSAH continues to challenge the healthcare system in India and other developing countries. We have to look at early detection strategies and an efficient referral system in order to treat such patients in time. Unlike other forms of stroke, aSAH provides us with a window of opportunity to detect and treat the aneurysm before it ruptures and SAH occurs. Population-based studies need to be taken up in India, as they will be the first step to evolving a screening program that could help detect and treat intracranial aneurysms before the catastrophe strikes.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: A meta-analysis. Lancet Neurol. 2009;8:635-42.
- [Google Scholar]
- Case-fatality rates and functional outcome after subarachnoid hemorrhage: A systematic review. Stroke. 1997;28:660-4.
- [Google Scholar]
- Impact of early surgery on outcome after aneurysmal subarachnoid hemorrhage. A population-based study. Stroke. 1993;24:1649-54.
- [Google Scholar]
- Subarachnoid hemorrhage: Is it time for a new direction? Stroke. 2009;40(Suppl 3):S86-7.
- [Google Scholar]
- Subarachnoid haemorrhage: What happens to the cerebral arteries? Clin Exp Pharmacol Physiol. 1998;25:867-76.
- [Google Scholar]
- Subarachnoid hemorrhage in Kashmir: Causes, risk factors, and outcome. Asian J Neurosurg. 2011;6:57-71.
- [Google Scholar]
- Study of patient characteristics/profile and factors determining the (immediate) outcome in spontaneous subarachnoid hemorrhage. J Assoc Physicians India. 2011;59:505-8.
- [Google Scholar]
- Factors and outcomes associated with early and delayed aneurysm treatment in subarachnoid hemorrhage patients in the United States. Neurosurgery. 2012;71:670-8.
- [Google Scholar]
- Does the impact of elective temporary clipping on intraoperative rupture really influence neurological outcome after surgery for ruptured anterior circulation aneurysms.–A prospective multivariate study? Acta Neurochir (Wien). 2013;155:237-46.
- [Google Scholar]
- Poor-grade subarachnoid hemorrhage: Is surgical clipping worthwhile? Neurol India. 2011;59:212-7.
- [Google Scholar]
- Management of poor-grade patients with aneurysmal subarachnoid hemorrhage in the acute stage: Importance of close monitoring for neurological grade changes. Surg Neurol. 2004;62:531-7.
- [Google Scholar]
- Functional outcome 3 months after stroke predicts long-term survival. Cerebrovasc Dis. 2008;25:423-9.
- [Google Scholar]
- Declining mortality from subarachnoid hemorrhage: Changes in incidence and case fatality from 1985 through 2000. Stroke. 2004;35:2059-63.
- [Google Scholar]
- Case fatality after subarachnoid haemorrhage: Declining, but why? Lancet Neurol. 2009;8:598-9.
- [Google Scholar]
- Incidence, risk factors, and outcome of postoperative pneumonia after microsurgical clipping of ruptured intracranial aneurysms. Surg Neurol Int. 2013;4:24.
- [Google Scholar]
- ; Steering Group for National Study of Subarachnoid Haemorrhage. Variation in outcome after subarachnoid hemorrhage: A study of neurosurgical units in UK and Ireland. Stroke. 2009;40:111-8.
- [Google Scholar]
- Microsurgical clipping and endovascular coiling of intracranial aneurysms: A critical review of the literature. Neurosurgery. 2008;62:1187-203.
- [Google Scholar]
- Clipping versus coiling for ruptured intracranial aneurysms: A systematic review and meta-analysis. Stroke. 2013;44:29-37.
- [Google Scholar]
- Incidence and early prognosis of aneurysmal subarachnoid hemorrhage in Kumamoto Prefecture, Japan. Neurosurgery. 2004;54:31-8.
- [Google Scholar]
- Initial and recurrent bleeding are the major causes of death following subarachnoid hemorrhage. Stroke. 1994;25:1342-7.
- [Google Scholar]
- The International Cooperative Study on the Timing of Aneurysm Surgery. Part 1: Overall management results. J Neurosurg. 1990;73:18-36.
- [Google Scholar]
- Toward more rational prediction of outcome in patients with high-grade subarachnoid hemorrhage. Neurosurgery. 2000;46:28-36.
- [Google Scholar]
- Risk factors for subarachnoid hemorrhage: An updated systematic review of epidemiological studies. Stroke. 2005;36:2773-80.
- [Google Scholar]
- Hyperglycemia, excess weight, and history of hypertension as risk factors for poor outcome and cerebral infarction after aneurysmal subarachnoid hemorrhage. J Neurosurg. 2005;102:998-1003.
- [Google Scholar]
- Prognostic factors on hospital admission after spontaneous subarachnoid haemorrhage. Acta Neurochir (Wien). 2001;143:665-72.
- [Google Scholar]
- Prognostic factors for outcome in patients with aneurysmal subarachnoid hemorrhage. Stroke. 2007;38:2315-21.
- [Google Scholar]
- Cerebral infarction after subarachnoid hemorrhage contributes to poor outcome by vasospasm-dependent and -independent effects. Stroke. 2011;42:924-9.
- [Google Scholar]
- Demographic study of first-ever stroke and acute myocardial infarction in Okinawa, Japan. Intern Med. 1998;37:736-45.
- [Google Scholar]
- Changes in subarachnoid hemorrhage mortality, incidence, and case fatality in New Zealand between 1981-1983 and 1991-1993. Stroke. 1998;29:2298-303.
- [Google Scholar]
- Trends in the incidence of subarachnoid hemorrhage in Akita Prefecture, Japan. J Neurosurg. 2007;106:234-8.
- [Google Scholar]
- Seasonal patterns of incidence and case fatality of stroke in Malmo, Sweden: The STROMA study. Neuroepidemiology. 2005;24:26-31.
- [Google Scholar]
- Epidemiology of aneurysmal subarachnoid hemorrhage in Australia and New Zealand: Incidence and case fatality from the Australasian Cooperative Research on Subarachnoid Hemorrhage Study (ACROSS) Stroke. 2000;31:1843-50.
- [Google Scholar]




