
Translate this page into:
Plethysmography motion artifact can be an indicator of peripheral stimulus delivery during intraoperative somatosensory evoked potential recording

*Corresponding author: Balaji Vaithialingam, Second floor, Second cross, Gundappa Gowda Road, Ejipura main road, Viveknagar, Bengaluru - 560 047, Karnataka, India. balamedicine04@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sravani K, Masapu D, Vaithialingam B. Plethysmography motion artifact can be an indicator of peripheral stimulus delivery during intraoperative somatosensory evoked potential recording. J Neurosci Rural Pract. 2024;15:519-20. doi: 10.25259/JNRP_555_2023
Dear Editor,
Somatosensory evoked potential (SSEP) is a well-known modality for monitoring the sensory tract integrity (peripheral nerve, dorsal column, and sensory tract) during spine surgeries.[1] The SSEP entails recording responses from cranial/epidural electrodes after peripheral nerve stimulation. Peripheral electrical stimulation can cause a motion artifact in the pulse-oximeter plethysmography waveform during intraoperative SSEP recording, interfering with the pulse oximetry reading. On the contrary, this SSEP motion artifact in the pulse oximeter can have clinical utility during neuromonitoring. Low perfusion, electromagnetic interference, and motion can all cause artifacts in the plethysmography waveform of the pulse oximeter. Plethysmography waveform motion artifacts can be caused by either the patient’s respiration or the movement resulting in a low signal-to-noise ratio and inaccurate pulse oximeter readings. During intraoperative upper-limb SSEP recording, needle electrodes are placed at the wrist between the palmaris longus and flexor carpi radialis tendon (anode at the wrist crease and cathode 3 cm proximal to anode) to stimulate the median nerve.[2] Because the median nerve is a mixed nerve, it produces both antidromic and orthodromic conduction when stimulated. Antidromic conduction causes potentials to travel along the dorsal somatosensory pathway, which can be recorded using scalp electrodes. Orthodromic conduction, on the other hand, causes muscle contraction, which causes motion artifacts in the pulse oximetry plethysmography waveform [Figures 1a and b]. The presence of plethysmography artifacts during the SSEP recording has both advantages and disadvantages. The current delivery following median nerve stimulation for SSEP recording can be confirmed intraoperatively by visualization of finger movement. Because finger movements are not always visible under surgical drapes, this median nerve stimulation artifact in the pulse-oximeter plethysmography waveform can be used as an alternative for confirming stimulus delivery. The inability to obtain an intraoperative SSEP recording is most commonly due to technical reasons (inability to stimulate the peripheral nerve due to failure of current delivery or high impedance of scalp recording electrodes). During a technical glitch scenario, the presence of a plethysmography artifact can ensure peripheral nerve stimulation with adequate current delivery. The motion artifacts are unavoidable, as the frequency band of the signal due to finger movement (>0.1 Hz) overlaps with the frequency band of the pulse wave signal of the pulse oximeter (0.5–4 Hz).[3] Muscle relaxants can help with SSEP recording by increasing the signal-to-noise ratio and removing pulse-oximetry artifacts caused by finger movement. Because SSEP recording is part of multimodal monitoring, which is frequently used in conjunction with motor evoked potential monitoring, it is critical to avoid using muscle relaxants intraoperatively. Anesthesiologists must be aware of the median nerve stimulation artifact in the pulse-oximeter plethysmography waveform during SSEP monitoring. Even though plethysmography motion artifacts are unwanted, the anesthesiologist can use this pulse-oximeter motion artifact during SSEP recording as an alternative method to confirm the peripheral stimulus delivery.
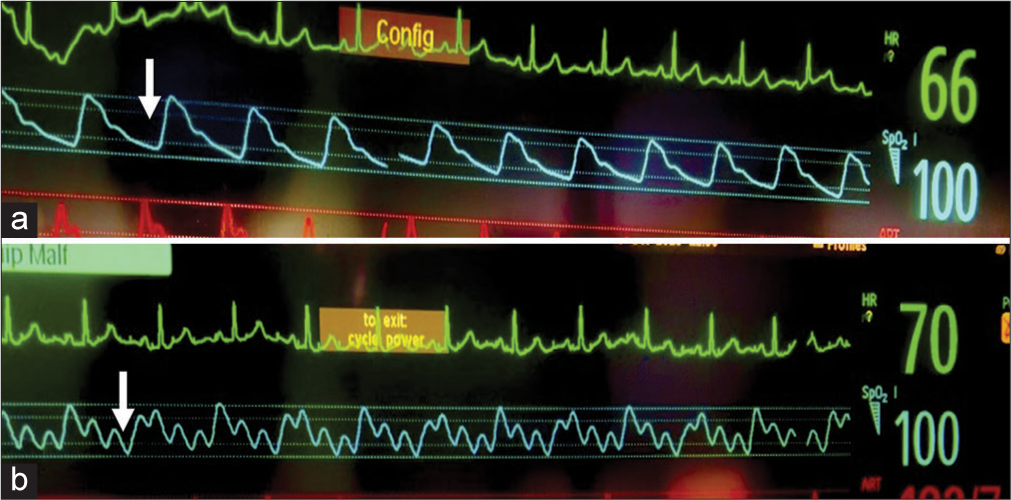
- (a) A normal pulse-oximeter plethysmography waveform (arrow). (b) Pulse-oximeter plethysmography waveform showing motion artifact (arrow) due to peripheral stimulus delivery during median nerve somatosensory evoked potential recording.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Intraoperative neurophysiological monitoring in spinal surgery. World J Clin Cases. 2015;3:765-73.
- [CrossRef] [PubMed] [Google Scholar]
- Recommendations of the international society of intraoperative neurophysiology for intraoperative somatosensory evoked potentials. Clin Neurophysiol. 2019;130:161-79.
- [CrossRef] [PubMed] [Google Scholar]
- Design of filter to reject motion artifact of pulse oximetry. Comput Stand Interfaces. 2004;26:241-9.
- [CrossRef] [Google Scholar]




