
Translate this page into:
Normative Data for Median Nerve Conduction in Healthy Young Adults from Punjab, India
Address for correspondence: Dr. Sharat Gupta, SST Nagar, Rajpura Road, Patiala - 147 001, Punjab, India. E-mail: sharatgupta29@yahoo.co.in
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Nerve conduction studies (NCSs) are essential for diagnosing various kinds of focal and diffuse neuropathies. Due to the paucity of local NCS data, electrodiagnostic laboratories in Punjab rely on values from Western and other Indian studies.
Aim:
This study was conducted to provide normative data for median nerve conduction parameters (motor and sensory) in Punjabi populace.
Materials and Methods:
A cross-sectional study was done on 290 participants (150 males and 140 females), aged 17–21 years, as per standardized protocol. The data were analyzed separately for both genders using SPSS version 20. It consisted of distal latencies and conduction velocities of motor and sensory divisions of median nerve. Student's unpaired t-test was used for statistical analysis.
Results:
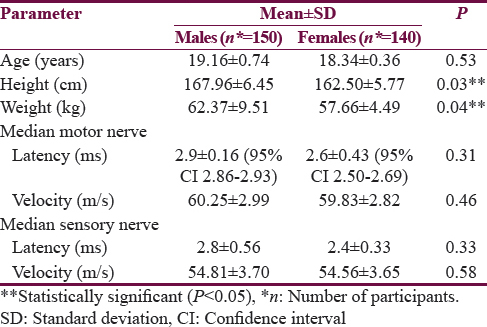
There was no effect of gender on any of the median nerve conduction parameters. Height and weight had nonsignificant negative and positive correlation, respectively (P > 0.05), with conduction velocity in both motor and sensory median nerves. For median motor nerve, the values of distal latency and conduction velocity in males were 2.9 ± 0.16 ms and 60.25 ± 2.99 m/s, respectively, whereas, in females, they were 2.6 ± 0.43 ms and 59.83 ± 2.82 m/s. Similarly, for median sensory nerve, the latency and velocity values in males were 2.8 ± 0.56 ms and 54.81 ± 3.70 m/s, whereas, in females, they were 2.4 ± 0.33 ms and 54.56 ± 3.65 m/s, respectively.
Conclusion:
The data in this study compared favorably with already existing data. It would help the local electrodiagnostic laboratories in assessing the median nerve abnormalities with greater accuracy in this population subset.
Keywords
Distal latency
median nerve
nerve conduction velocity
neuropathies
neurophysiology
peripheral neuropathy

INTRODUCTION
Nerve conduction studies (NCSs) are the most commonly used electrodiagnostic tests to determine the conduction in motor and sensory nerves.[1] NCS involves activation of nerves with small, safe electrical impulses over multiple points on the skin of limbs and thereafter measuring the obtained responses.[2] NCS is diagnostically helpful in patients suspected of having almost any kind of peripheral nervous system disorder including disorders of nerve roots, peripheral nerves, muscle, and neuromuscular junction.[3] The median nerve study is one of the most commonly performed NCS tests. It has been extensively used in research field as well as in clinical practice.[45]
NCS is influenced by various factors such as age, gender, ambient temperature, height, and weight.[6] Since these factors vary greatly among different geographical locations, thus it is imperative that each neurophysiology laboratory needs to have normative data that are specific for the population that it serves so as to accurately identify abnormal patients.[7] Although many studies have been conducted worldwide and in other parts of India regarding normative data for median nerve,[8910111213] there is an extreme paucity of similar data from this part of the country. Hence, the local electrodiagnostic laboratories in Punjab have to rely on standard values generated by other authors while diagnosing various median nerve abnormalities, thereby increasing the chances of reporting false-positive or false-negative results.
The present study was, therefore, designed to obtain a set of NCS values for motor and sensory median nerves so as to establish normative data for local laboratories. The results of this study were also compared with other similar studies already published worldwide.
MATERIALS AND METHODS
The present study was carried out over a period of 3 years in the neurophysiology laboratory of the institute. The procedures followed were in accordance with the ethical standards of the Institutional Committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2000.
Study participants
The present cross-sectional study was conducted among 17–21-year-old healthy medical students of the institute. The sample size was calculated using Cochran's formula for continuous data, and the participants were selected using simple random sampling technique.[14] Written consent was obtained from all of the participants after explaining them the details of the study in their own language. All those participants were included who were apparently healthy and volunteered for the study. Out of the initial 339 participants, 49 were subsequently excluded as per the exclusion criteria whereas the remaining 290 eligible participants were made to undergo NCS procedure.
Exclusion criteria
Those participants were excluded who had a personal/family history of any systemic disorder (e.g., diabetes mellitus, hypertension, and thyroid disorders), any neuromuscular disorder, neuropathy, myopathy, personal history of limb injury or alcoholism/cigarette smoking, or the usage of medications that could affect the results (e.g., hypolipidemic drugs and antidepressants).
Medical and biochemical examination
Before taking NCS recordings, all the participants were subjected to the following:
-
Detailed history by way of self-administered questionnaire, to know about medical history and lifestyle
-
Detailed general physical and systemic examination including a preliminary neurological assessment to test muscle power, deep tendon reflexes, and sensations
-
Serum urea, creatinine, electrolytes, and fasting blood glucose levels.
Nerve conduction study
It was performed as per the guidelines of a standardized protocol for median motor and sensory nerve testing as was adopted elsewhere.[1516] The data were recorded with a PC-based RMS EMG EP Mark-II Channel machine (Recorders and Medicare Systems Pvt. Ltd., Chandigarh, India).
Before starting the test, age was calculated to the nearest completed year, standing height (in centimeter) was measured without shoes, and weight (in kilograms) with minimal clothing was also noted. The participants were made to sit comfortably on a chair and were asked to avoid unnecessary movement and to remove all the metallic ornaments that they might be wearing. The laboratory temperature was maintained at 25–27°C. For the safety of the participants, it was ensured that the machine was properly earthed. The actual procedure of conducting NCS is discussed below:
For median motor nerve conduction, the low cut filter was 2–5 Hz and the high cut filter was 10 kHz. Similarly, for median sensory nerve conduction, the low cut was set at 5–10 Hz whereas the high cut filter was set at 2–3 kHz. The amplitude was between 20,000 and 100,000 times; electronic impedance was kept below 5kΩ and the sweep speeds were maintained at 2–5 ms/division and 1–2 ms/division for median motor and sensory nerves, respectively. A stimulus of 50 ms to 1000 μs and a current of 0–50 mA were applied for effective stimulation of median nerve. Supramaximal stimuli (i.e., 20%–30% more than the current required for maximal action potential) were delivered to obtain adequate responses.
The median motor nerve was examined orthodromically using two stainless steel electrodes (Natus Medical Inc., Canada) that were placed on skin surface after first applying conducting jelly (to ensure optimum conduction and reduced impedance) on them and then fixing them with self-adhesive surgical tape. Disc-shaped recording electrode (1 cm diameter) was placed over the belly of abductor pollicis brevis, the reference electrode was placed on its tendon (i.e., 4 cm distally over the first metacarpophalangeal joint), and the ground electrode was placed between the stimulating and recording electrodes. The NCS was done on the right upper limb of the participants. Before applying the electrodes, stimulation and recording areas on the skin were cleaned with 70% alcohol solution. The nerve was stimulated at two points along its course using bipolar surface bar electrodes, in which the anode and cathode terminals are placed 20 mm apart. Proximal stimulation was given at the elbow crease, medial to the biceps brachii tendon whereas the distal stimulation was performed at the wrist (3 cm proximal to the distal wrist crease) between the tendons of flexor carpi radialis and palmaris longus muscles.
The median sensory nerve was examined antidromically with surface electrodes. Two spring-loaded, stainless steel ring-shaped recording electrodes (Natus Medical Inc., Canada) that fit around the digit were placed over the proximal and distal interphalangeal joints of the index finger, with one of these serving as recording electrode and the other as a reference electrode. The stimulation sites were similar to those for median motor nerve.
Distal latency in milliseconds was displayed by the machine following each stimulation. Distance between the cathode ends of the proximal and the distal stimulation points was measured using a flexible measuring tape to the nearest centimeter and fed into the machine to calculate the conduction velocity in meters per second. Velocity is determined for motor and sensory median nerves by dividing the distance of separation between stimulation and recording sites with latency. Recordings were repeated until the best possible response was obtained. All the printed records were verified by a consultant neurologist to ensure highest possible accuracy in results. Thereafter, the latencies and velocities of both motor and sensory divisions of median nerve were analyzed separately for males and females.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences software version 20 (SPSS Inc., Chicago, IL, USA). All the values were expressed in mean and standard deviation. Student's unpaired t-test was used to assess the significance of difference between the mean values of median nerve latency and velocity of males and females. P < 0.05 was considered statistically significant. The normal reference range of nerve conduction values was set by the 2½ and 97½ percentiles so that the reference ranges contain the central 95% of the distribution.
RESULTS
This study was conducted on a total of 290 participants (150 males and 140 females) aged 17–21 years. Table 1 summarizes the gender-wise comparison of the mean anthropometric and NCS parameters, i.e., distal latency and conduction velocity. It is evident from this table that, while the groups were comparable with respect to age, but the height and weight of males were significantly higher as compared to females (P < 0.05). Furthermore, the latency and velocity values of both motor and sensory divisions of median nerve were comparable between these two groups (P > 0.05).
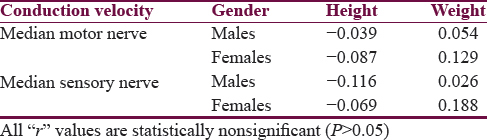
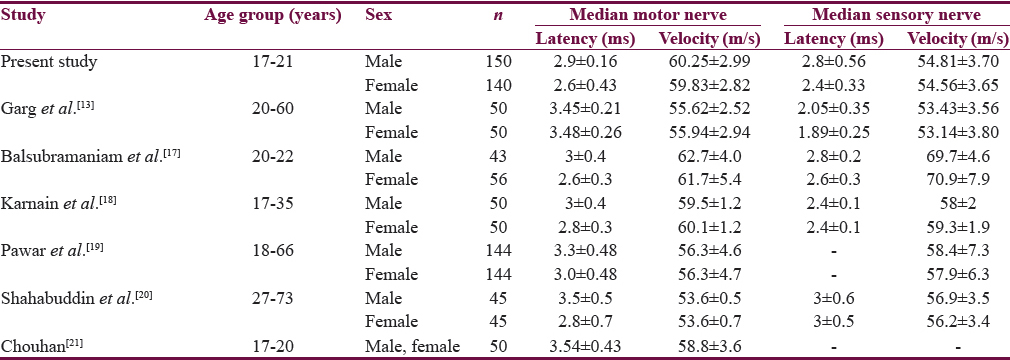
It was observed that height and weight had a nonsignificant negative and positive correlation, respectively, with conduction velocity of both motor as well as sensory median nerves [Table 2]. While doing a gender-wise comparison of the conduction velocity of median motor and sensory nerves according to height, it was observed that, in all the groups, the results were statistically nonsignificant (P > 0.05) [Table 3]. Furthermore, on doing a similar comparison according to weight of the participants, the values were again found to be comparable among both genders (P > 0.05) [Table 4]. A detailed comparison of the results of this study with those obtained by other authors[131718192021] is presented in Table 5.


DISCUSSION
The results of this study have shown that neither latency nor velocity is influenced in young adults by gender, both in case of motor and sensory divisions of median nerve. These findings are in complete agreement with most of the other authors.[7132223] We also agree with the results of Pawar et al.[19] regarding their reporting of nonsignificant difference in the motor and sensory median nerve velocities with respect to gender. However, we disagree with them regarding the significant effect of gender on latency values of these nerves. Our results are in absolute disagreement with a few other studies[1824] which have reported significantly higher values of both latency and velocity in males when compared with age-matched females.
In our study, there was a nonsignificant negative correlation of both motor and sensory median nerve velocity with height. These results are in conformity with many researchers,[32025] but are exactly opposite to the reports of a significant positive correlation between height and median nerve velocity reported in some studies.[1726] Our mean value for median motor latency is similar to those obtained by Balsubramaniam et al.[17] and Karnain et al.[18] It is slightly higher than the values of Garg et al.,[13] Pawar et al.,[19] Shahabuddin et al.,[20] and Chouhan.[21] Our mean value for sensory median DL is similar to Balsubramaniam et al.[17] and Karnain et al.[18] It is higher than Garg et al.[13] but lower than Shahabuddin et al.[20] The median motor nerve conduction was faster in our participants than previous reports[8131920] while it was similar with some others.[171821] The median sensory conduction was slower in our participants as compared to elsewhere[17181920] but was similar to that of Garg et al.[13]
Age difference of the participants included by the present and previous studies may have contributed to the above-noted differences in the results. There is evidence to suggest that nerve conduction slows down with advancing age.[322252728] Therefore, while the present study was confined to a narrow age group (17–21 years), most of the other researchers had included a large age group (including elderly population) which might have led to the increase in latency values with consequent reduction of the velocity values in their participants, thereby creating discrepancies between their results and our own. Another major reason for the observed differences is that since most of the available studies are western, hence the consequent methodology and geographical differences as well as the variations in the lifestyle, dietary, and morphological characteristics of study participants might also have influenced the study results.
The findings of this study assume clinical significance due to the fact that the integrity of the median nerve is imperative for normal functioning of hands. Median nerve is highly susceptible to damage by metabolic disturbances, entrapment neuropathies, and/or ischemia.[29] Nonetheless, median nerve abnormalities often remain undiagnosed in a vast majority of patients, but with NCS, more subclinical cases can be diagnosed at initial stages itself.[30]
Study limitations
A major limitation of our study was the noninclusion of a wider age group, thus limiting the benefit of this study to a specific section of the society. This was due to the time and resource constraints. However, the study was conducted strictly as per standardized guidelines, thereby ensuring as much accuracy as possible. Another limitation was that skin temperature of the participants was not recorded, due to which it was not possible to fully assess the possible effects of temperature in this study.
Future research directions
Clinical research should continue to assess the normative data in other peripheral nerves (e.g., common peroneal, sural, tibial, and ulnar). The values need to be determined in a wider age group so as to enable local electrodiagnostic laboratories to cater to a larger population. Furthermore, more such studies need to be conducted by other authors so as to generate reference data that is specific to their local populace.
CONCLUSION
This study has established normative data for median nerve conduction in Punjabi population. The overall mean motor and sensory median nerve conduction parameters compared favorably with existing literature data. Our values will prove useful in the accurate interpretation of median nerve abnormalities in young adults from this part of India, by reducing the incidence of false positives/negatives.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We are indebted to the all the study participants, without whose active participation this study would not have been possible.
REFERENCES
- Blink reflex, H-reflex and nerve-conduction alterations in leprosy patients. Lepr Rev. 2006;77:114-20.
- [Google Scholar]
- Nerve conduction studies: Essentials and pitfalls in practice. J Neurol Neurosurg Psychiatry. 2005;76(Suppl 2):ii23-31.
- [Google Scholar]
- Impact of anthropometric measures on sural nerve conduction in healthy subjects. J Ayub Med Coll Abbottabad. 2008;20:112-4.
- [Google Scholar]
- The relationship between nerve conduction study and clinical grading of carpal tunnel syndrome. J Orthop Surg (Hong Kong). 2003;11:190-3.
- [Google Scholar]
- Amplitude of sensory nerve action potential in early stage diabetic peripheral neuropathy: An analysis of 500 cases. Neural Regen Res. 2014;9:1389-94.
- [Google Scholar]
- Influence of age, gender, and sidedness on ulnar nerve conduction. J Clin Neurophysiol. 2013;30:98-101.
- [Google Scholar]
- Nerve conduction studies in healthy Iraqis: Normative data. Iraqi J Med Sci. 2009;7:75-92.
- [Google Scholar]
- Normative values of motor and sensory nerve conduction studies. Galle Med J. 2010;15:43-4.
- [Google Scholar]
- Determination of the median nerve residual latency values in the diagnosis of carpal tunnel syndrome in comparison with other electrodiagnostic parameters. J Res Med Sci. 2013;18:934-8.
- [Google Scholar]
- Assessment of motor nerve conduction in healthy obese Indian population. Int J Clin Exp Physiol. 2014;1:277-82.
- [Google Scholar]
- To assess the nerve conduction velocity declination rate according to age in median nerve of healthy subjects. Int J Sci Res. 2016;5:1036-8.
- [Google Scholar]
- Nerve conduction studies in the upper limb in the malwa region-normative data. J Clin Diagn Res. 2013;7:201-4.
- [Google Scholar]
- Sampling Techniques (3rd ed). New York: John Wiley & Sons; 1977.
- Nerve conduction study among healthy Malays. The influence of age, height and body mass index on median, ulnar, common peroneal and sural nerves. Malays J Med Sci. 2006;13:19-23.
- [Google Scholar]
- Electrodiagnosis in Diseases of Nerve and Muscle: Principles and Practice (3rd ed). Philadelphia: Davis; 2001. p. :131-68.
- Upper limb nerve conduction parameters of healthy young adults. Asian Pac J Health Sci. 2016;3:121-6.
- [Google Scholar]
- Gender effect on upper limb nerve conduction study in healthy individuals of North India. J Pharm Biomed Sci. 2013;33:1589-93.
- [Google Scholar]
- Normative data of upper limb nerve conduction in Central India. Indian J Physiol Pharmacol. 2011;55:241-5.
- [Google Scholar]
- Normative values for nerve conduction study among healthy subjects from Aurangabad, India. Int J Recent Trends Sci Technol. 2013;8:56-61.
- [Google Scholar]
- Motor nerve conduction studies of median nerve in young adult group. Int J Bio Med Res. 2012;3:1751-3.
- [Google Scholar]
- Normative data of nerve conduction studies in the upper limb in Kuwait: Are they different from Western data? Med Princ Pract. 1998;7:203-8.
- [Google Scholar]
- Gender and arm length: Influence on nerve conduction parameters in the upper limb. Arch Phys Med Rehabil. 1994;75:265-9.
- [Google Scholar]
- Nerve conduction study in healthy individuals, a gender based study. Health Renaiss. 2010;8:169-75.
- [Google Scholar]
- Standardized nerve conduction studies in the upper limb of the healthy elderly. Am J Phys Med Rehabil. 1992;71:263-71.
- [Google Scholar]
- Influence of height on the nerve conduction study parameters of peripheral nerves. J Clin Diag Res. 2011;5:260-3.
- [Google Scholar]
- Median nerve conduction in healthy Nigerians: Normative data. Ann Med Health Sci Res. 2016;6:85-9.
- [Google Scholar]
- Effects of age, gender, height, and weight on late responses and nerve conduction study parameters. Acta Neurol Taiwan. 2009;18:242-9.
- [Google Scholar]
- Median neuropathy. In: Dyck PJ, Thomas PK, eds. Peripheral Neuropathy (4th ed). Philadelphia: Elsevier Saunders; 2005. p. :1435-61.
- [Google Scholar]




