
Translate this page into:
Neurofibromatosis type 2: Intracranial calcifications as a clue to diagnosis
Address for correspondence: Dr. Senthil Kumar Aiyappan, Department of Radiodiagnosis and Imaging, Saveetha Medical College and Hospital, Thandalam, Kancheepuram - 602 105, Tamil Nadu, India. E-mail: senthilkumarpgi@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
We hereby report a case of neurofibromatosis type 2 (NF-2) with typical imaging findings on computed tomography (CT) and magnetic resonance imaging (MRI) which was diagnosed on the basis of intracranial calcifications.
A 20-year-old male patient presented with complaints of right-sided diminished hearing and vision for the past 2 months. Initially plain CT of the brain was done which showed the presence of multiple small calcified subependymal nodules, bilateral choroid plexus calcifications, falx, tentorial calcifications and calcified nodule along the basal cistern region [Figure 1a–c]. Plain CT also showed the presence of optic nerve sheath calcification on right side suggestive of optic nerve sheath meningioma [Figure 1d]. Possibility of NF-2 was thought and the patient was subjected to MRI of brain and spine with contrast which showed the presence of small enhancing masses within bilateral internal acoustic meatus suggestive of vestibular schwannomas [Figure 2a] and a small right posterior parafalcine enhancing lesion suggestive of meningioma [Figure 2b]. In addition, intraspinal tumors were noted in cervical and lumbar regions [Figure 2c and d] along with paraspinal tumors in bilateral upper dorsal regions [Figure 2c]. In view of all these imaging findings, a diagnosis of type 2 neurofibromatosis was made. There was family history of early death of patient's father, the cause of which not known and the patient is the only sibling and unmarried. MRI brain and spine of the patient's mother was normal. The patient and his family were advised genetic counseling and testing to a higher center.
NF-2 is an autosomal dominant disorder characterized by the presence of schwannomas, meningiomas and ependymomas.[1] Bilateral vestibular schwannomas or family history of NF-2 with unilateral vestibular schwannoma or any of the two, meningioma, glioma, neurofibroma, schwannoma, posterior sublenticular capsular cataract, is the main diagnostic criteria for NF-2.[1] Intracranial calcifications are uncommon in NF-2 and can be tumoral or non-tumoral in origin. Although subependymal calcifications are always associated with tuberous sclerosis, similar calcifications can be seen in NF-2.[2] Non-tumoral calcifications with or without tumoral calcifications can suggest a diagnosis of NF-2 in patients whom there is no obvious lesion in cerebellopontine angles on CT.[2] Hence, further evaluation with MRI is required in those patients for accurate diagnosis. It is very difficult to radiologically distinguish schwannomas and meningiomas; however, intense heterogeneous enhancement, hyperintense and heterogeneous signal on T2-weighted images, craniocaudal location and absence of dural tail sign suggest schwannomas.[3]
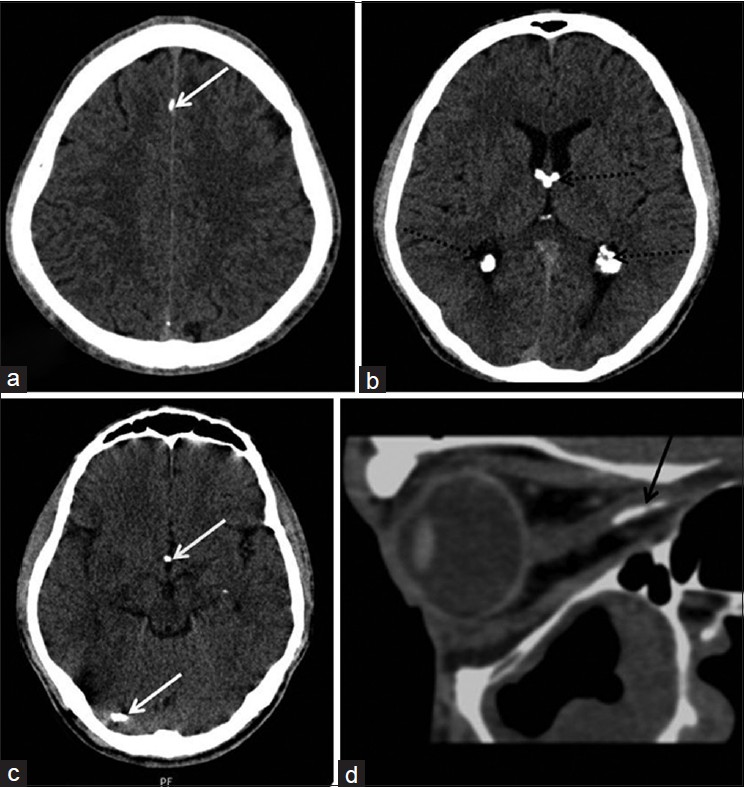
- Axial plain CT sections (a-c) showing multiple small calcifications along falx, right tentorium, basal cistern (white arrows), subependymal locations along with bilateral choroid plexus calcifications (dotted black arrows). (d) Sagittal multiplanar reformatted CT image showingperipheral curvilinear calcification along optic nerve (black arrow)
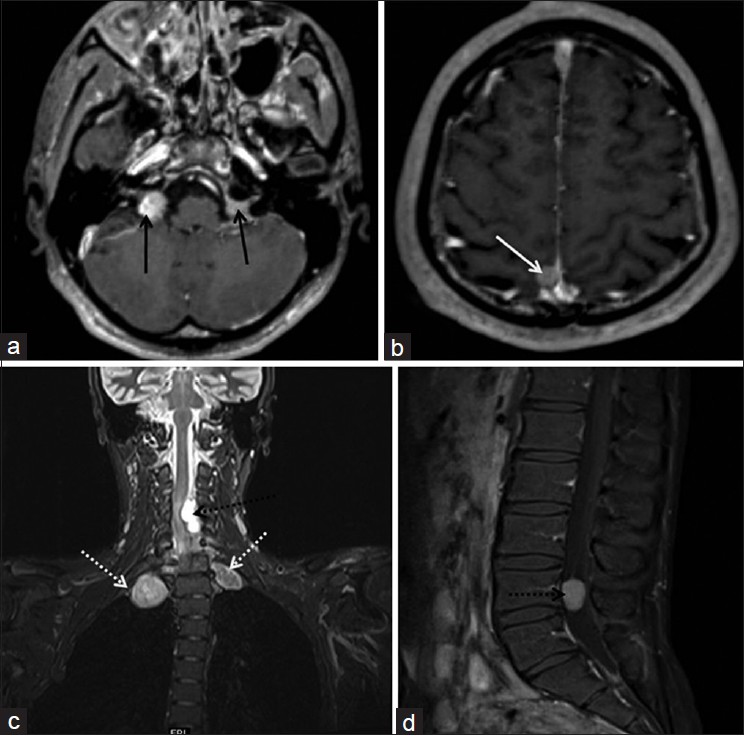
- (a and b) Axial contrast MRI showing small vestibular schwannomas within bilateral acoustic canal (black arrows) and a posterior parafalcine meningioma (white arrow). (c) Coronal MR cervical spine image showing tumors in bilateral paraspinal location (dotted white arrow) and within the cervical spinal canal (dotted black arrow). (d) Sagittal post contrast images of lumbar spine showing enhancing intraspinal tumor (dotted black arrow)
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Neurofibromatosis type 2 (NF2): A clinical and molecular review. Orphanet J Rare Dis. 2009;4:16.
- [Google Scholar]
- An uncommon case of neurofibromatosis type 2: A tribute to the intracranial calcifications. J Clin Imaging Sci. 2013;3:21.
- [Google Scholar]
- MR imaging features of spinal schwannomas and meningiomas. J Neuroradiol. 2005;32:42-9.
- [Google Scholar]




