
Translate this page into:
Myasthenia gravis and numb chin syndrome with lung carcinoma
*Corresponding author: Rajesh Kumar Gupta, Department of Neurology, Division of Neuroimmunology, University of Texas Health Science Centre, Houston, Texas, United States. rajneuro@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta RK, Gupta A, Um DS, Neda ZK. Myasthenia gravis and numb chin syndrome with lung carcinoma. J Neurosci Rural Pract. 2024;15:159-61. doi: 10.25259/JNRP_387_2023
Dear Editor,
We present the case of a man in his 50s with a history of smoking and previous treatment for right-sided nasopharyngeal squamous cell carcinoma using chemotherapy and radiotherapy in 2016. He was currently in remission when he visited our neurology clinic with chronic headaches, which were determined to be a combination of cervicogenic headache and migraine. During his initial appointment, he also mentioned experiencing dysphagia and difficulty opening his mouth, which he attributed to his previous throat cancer and surgery. However, upon examination, we observed weakness in his bulbar muscles, raising suspicion for myasthenia gravis (MG).
Laboratory testing confirmed the presence of antiacetylcholine receptor (AChR) antibodies, with a level of 0.52 nmol/L, and he was initiated on intravenous immunoglobulin treatment. A computed tomography (CT) scan of his chest ruled out thymoma but revealed a 3.1-cm solid mass in the medial aspect of the posterior left lobe [Figure 1a]. An initial transbronchial biopsy of the lung mass did not indicate malignancy but showed chronic inflammation and aggregates of anthracotic-laden macrophages. For his MG, he was subsequently prescribed pyridostigmine 60 mg 3 times daily and prednisone 60 mg once daily.
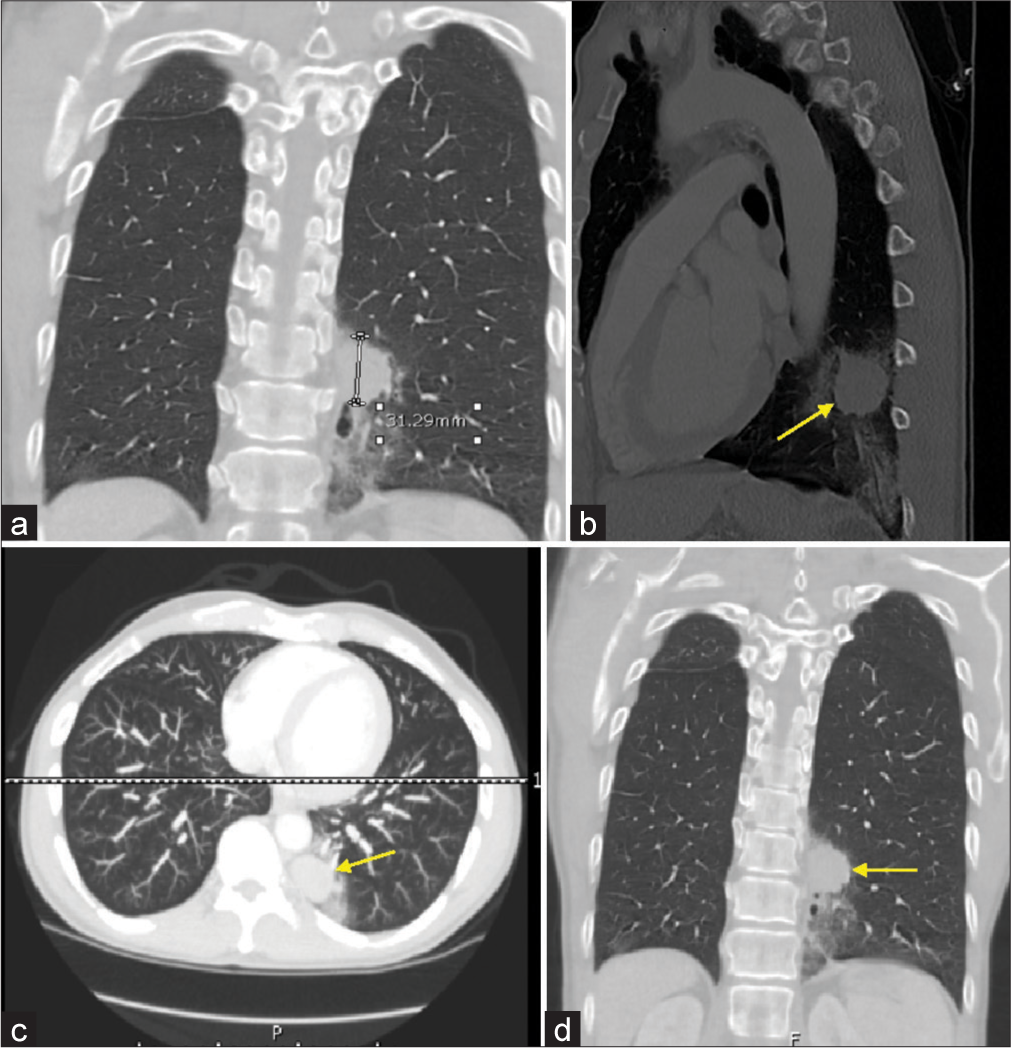
- A 55-year-old patient presented with numb chin syndrome and myasthenia gravis. (a) Initial computed tomography (CT) chest showing mass measuring 3.1 cm. (b-d) Repeat CT chest revealed mass measuring 3.4 cm (Yellow arrows showing the lung mass).
During a routine follow-up appointment 8 months later, he reported numbness on the right side of his chin. Given the suspicion of systemic malignancy, a repeat CT scan of the chest was recommended, which revealed an increased size of the lung mass to 3.4 cm with lymphangitis carcinomatosis and alveolar hemorrhage [Figure 1b-d]. A repeat transbronchial biopsy confirmed a poorly differentiated squamous cell carcinoma that was positive for cytokeratin 5/6 and negative for thyroid transcription factor-1 and synaptophysin [Figure 2a-c].
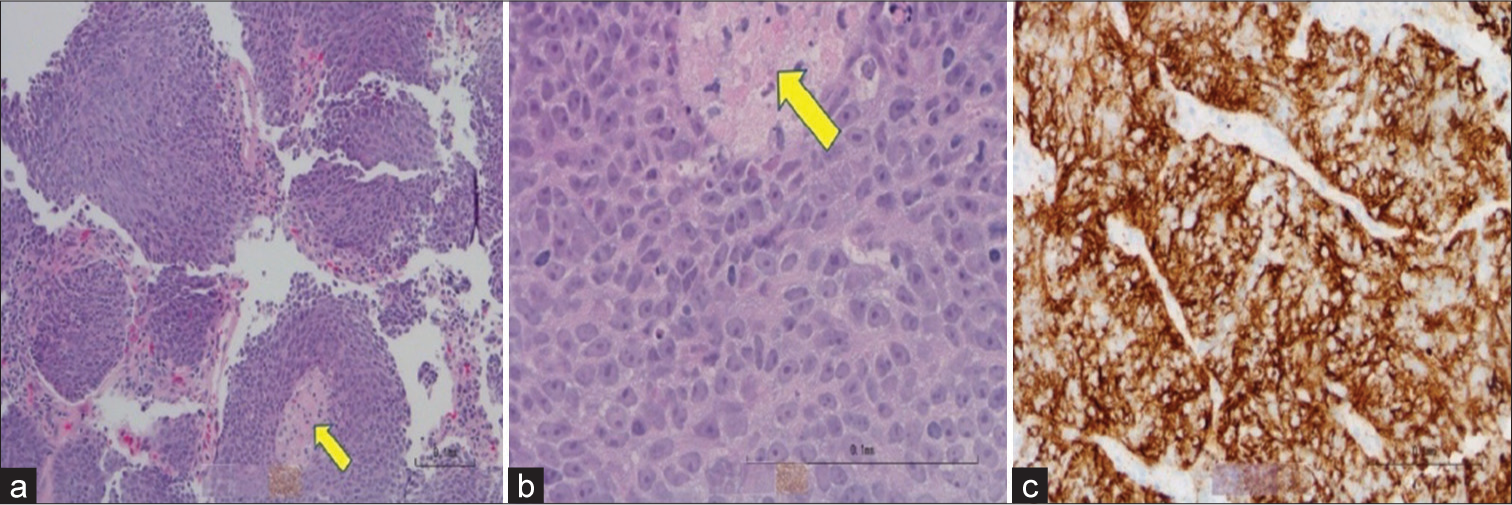
- Immunohistochemistry slides from biopsy. (a) Hematoxylin and Eosin lower power of the biopsy revealed nests of tumor cells with focal necrosis (yellow arrow). (b) Hematoxylin and Eosin high power of the biopsy revealed malignant cells with enlarged nuclei, prominent nucleoli, and scant cytoplasm. Necrosis is indicated by the yellow arrow. (c) Cytokeratin 5 and 6 stain highlighted malignant squamous cells.
A staging positron emission tomography (PET) scan showed a primary 3.0 cm left lower lung mass, a 1.6 cm right lower lung nodule, smaller bilateral pulmonary nodules, multicompartmental lymphadenopathy in the chest, and likely bone metastasis involving the right seventh rib, right L3–4 facet joint, right anterior fourth rib, right posterior 11th rib, right ischial tuberosity, and the left iliac bone.
Given his malnutrition and anorexia, the patient was deemed unsuitable for chemotherapy by the oncology team. He was referred to palliative care and started on a fentanyl patch and liquid formulation of hydromorphone (DILAUDID). As his pain, loss of appetite, nausea, and overall decline worsened, he was enrolled in hospice care. Unfortunately, the patient passed away 5 months after the diagnosis of lung cancer.
Numb chin syndrome (NCS) is a sensory neuropathy of mental nerve which is a continuation of the inferior alveolar nerve, arising from mandibular division of trigeminal nerve. NCS typically presents with sensory symptoms alone such as numbness of lower lip and chin, as it lacks a motor component.[1] The most common causes of NCS include dental procedures, dental infections, and neoplasms.[2]
Laurencet et al. reported five cases of patients with chin numbness associated with metastatic diseases including small-cell lung cancer, prostate cancer, and breast cancer.[3] The authors concluded that this clinical sign is thought to be due to bone metastases or leptomeningeal seeding. However, this symptom can also arise due to the involvement of the mental nerve. Moreover, they also indicated a survival period of <1 year in these cases. This underscores the importance of giving significant attention to malignancy in patients with NCS. The plausible causes of NCS in our patient could be perineural invasion or paraneoplastic neuropathy along the tract from trigeminal to mental nerve as PET scan showed no direct metastatic involvement of mandible, base of skull, and trigeminal nerve.
Concomitant presence of lung cancer and MG has been increasingly reported, most commonly with small cell carcinoma and adenocarcinoma of the lung. However, the association with squamous cell carcinoma is relatively less common, with only one case reported in our review. Sakamaki et al. described a case of seropositive anti-AChR Ab MG patient without thymoma associated with squamous cell carcinoma of the lung where patient had bulbar complaints at presentation.[4] Lambert-Eaton myasthenic syndrome is the most common paraneoplastic syndrome (PNS) associated with lung cancer. However, the growing presence of MG with lung cancer raises the possibility MG as a PNS.[5] Our case further supports the likelihood of MG as one of the paraneoplastic manifestation of lung cancer. Clinicians should continue immunotherapy with antitumor medication for better prognosis.
This case report highlights a rare case of MG and numb chin syndrome in a patient who developed metastatic lung disease and discusses the significance of considering malignancy in patients presenting with either or both of these syndromes. We also emphasize the possibility of MG as a PNS in lung carcinoma.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Numb chin syndrome leading to a diagnosis of salivary ductal adenocarcinoma: A case report and review of the literature. Front Neurol. 2017;8:343.
- [CrossRef] [Google Scholar]
- Mental nerve neuropathy: Patient characteristics and neurosensory changes. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:364-70.
- [CrossRef] [PubMed] [Google Scholar]
- Mental neuropathy: Report of five cases and review of the literature. Crit Rev Oncol Hematol. 2000;34:71-9.
- [CrossRef] [PubMed] [Google Scholar]
- Non-small-cell lung cancer associated with non-thymomatous myasthenia gravis. Jpn J Thorac Cardiovasc Surg. 2006;54:207-11.
- [CrossRef] [PubMed] [Google Scholar]
- Myasthenia-like paraneoplastic syndrome with multiple cranial nerve tumor infiltration: A case report and literature review. Medicine (Baltimore). 2023;102:e33774.
- [CrossRef] [PubMed] [Google Scholar]




