
Translate this page into:
Multidetector-row computed tomography in cerebral hydatid cyst
Address for correspondence: Dr. Nisar A. Wani, Department of Radiodiagnosis and Imaging, Sher-I-Kashmir Institute of Medical Sciences, Srinagar – 190 011, Jammu & Kashmir, India. E-mail: nisar.wani@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Intracranial localization is a rare manifestation of hydatid cyst disease (Echinococcosis). It comprises only 2% of cases of Echinococcosis infection even in endemic areas and is predominantly seen in children. Clinical manifestations resulting from raised intracranial tension are nonspecific. Imaging with computed tomography (CT) may suggest the diagnosis preoperatively with reasonable accuracy. Multidetector-row CT (MDCT) with its high resolution multiplanar reformations can demonstrate the relationship of the cyst with adjacent brain structures and thus help in planning surgery. This has a practical utility in places where magnetic resonance imaging is not available. We describe a case of cerebral hydatid cyst in a 13-year-old boy who was diagnosed with MDCT, which helped in planning its surgical removal.
Keywords
Cerebral hydatid cyst
multidetector-row CT
papilledema

Introduction
Echinococcosis, a zoonosis with worldwide distribution is caused by the larvae of Echinococcus granulosus and Echinococcus multilocularis. Man is infected as an accidental host after eating food contaminated with Echinococcus eggs in the excreta of definitive hosts, such as dogs. The larvae after hatching from the eggs enter the portal circulation and land in the liver, which is the most commonly involved organ.[1] After entering the systemic circulation, the larvae may grow into hydatid cysts in other organs, such as the lungs and the brain. The hydatid cyst grows slowly in the brain and produces symptoms as a result of mass effect and compression due to raised intracranial pressure.[12] Diagnosis of intracranial hydatid cyst can be accomplished by serology and imaging with computed tomography (CT) and magnetic resonance imaging (MRI).[3] MRI is preferred for planning surgery.
Case Report
A 13-year-old boy presented to the emergency department with onset of acute vomiting and generalized tonic-clonic seizures since 5 days. He had been having headache for a month or so, which also aggravated recently. On examination, he was stuporous with Glasgow Coma Scale (GCS) score of 10/15; papilledema was present on both the sides. An urgent CT of head was performed on a 64-slice multidetector-row CT (MDCT) before and after intravenous injection of iodinated contrast. Noncontrast CT showed a large, well-defined rounded mass measuring 9 × 8 cm in the right occipital region of the brain. Hypodense mass lesion in the right occipital lobe showed homogenous fluid attenuation of <15 Hounsfield units (HU) with a thin and smooth peripheral wall; no perilesional edema was present in the adjacent white matter, and no calcification was seen [Figure 1]. Thin curvilinear septations were seen inside the cyst attached to the posterior cyst wall, which was better demonstrated by a sagittal reformatted image, representing a daughter cyst [Figure 2]. Postcontrast CT did not show any contrast enhancement in the cyst wall or in the peripheral mural septation (daughter cyst) posteriorly inside the cyst [Figure 3]. Compressed brain parenchyma was seen all around the periphery of the cystic mass, although it appeared effaced along the posterior aspect [Figures 1–3]. There was mass effect due to the cyst in the form of effacement of right lateral ventricle and midline shift toward left [Figures 1, 3]. CT findings of a large intraaxial cyst in the brain without any edema or enhancement were compatible with a possible diagnosis of right occipital lobe hydatid cyst. All three dimensions of the cyst in the transverse, anteroposterior, and superoinferior orientations, along with its relationship with the adjacent cortex and deep structures of the brain were depicted well by MDCT. Chest radiography and ultrasonography of abdomen did not reveal any hydatid in lung or liver. The patient was operated and a large cyst was found in the right occipital lobe on craniotomy, which was removed in toto taking special care not to rupture the cyst. Gross and microscopic examination of the cyst contents confirmed its hydatid nature. The patient made unremarkable recovery and was discharged on the 10th postoperative day. No recurrent or residual cyst was present on the follow-up scan after 2 months.
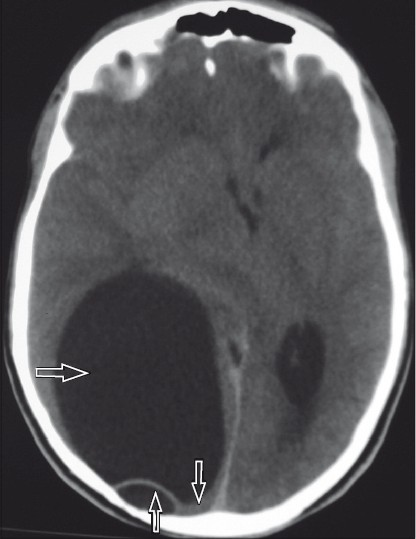
- A large (9 × 8 cm) spherical homogenous fluid attenuation mass with thin smooth wall around it in the right occipital lobe of brain (rightward arrow). Brain parenchyma is seen all around the cyst and is effaced more posteriorly (downward arrow). Significant mass effect is seen on the right lateral ventricle with midline shift to left; no perilesional edema is seen. Thin septation representing daughter cyst is seen posteriorly adjacent to wall (upward arrow); sagittal reformat CT image
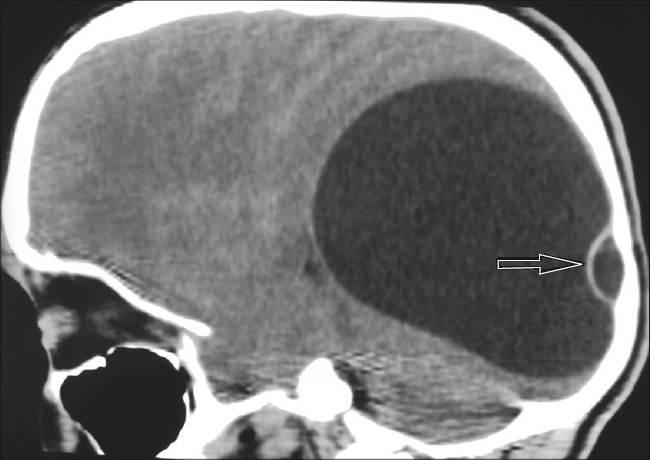
- A thin nonenhancing septation (daughter cyst) posteriorly within the cyst (arrow)
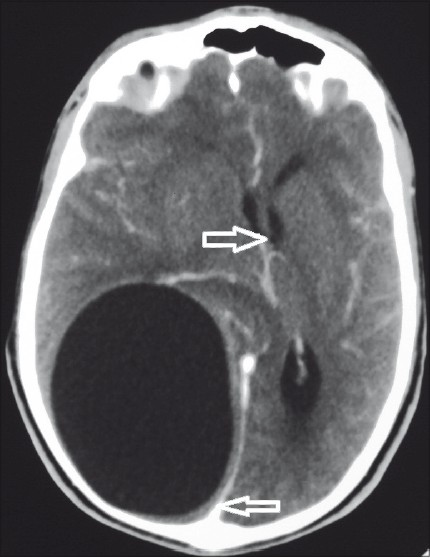
- Cyst surrounded by brain tissue all around (leftward arrow) with midline shift toward left (rightward arrow)
Discussion
Hydatid cyst of brain comprises about 2% of intracranial space occupying lesions and is more commonly seen in children. It is usually caused by E. granulosus and rarely by E. multilocularis larvae that after seeding the systemic circulation, lodge and develop in the brain.[14] More commonly intraaxial and supratentorial in location, hydatid cysts preferentially involve the middle cerebral artery distribution; however, sometimes a cyst may be extra-axial.[15] Hydatid cyst grows slowly at a rate of 1–10 cm/year and when well formed has an inner endocyst that forms daughter cysts and a whitish ectocyst through which it gets nourishment; pericyst is formed by the adjacent compressed brain parenchyma. Patients with cerebral hydatid cyst may also have hydatid in other organs, such as the liver and the lung.[1] Intracranial hydatid cysts are usually solitary and multiple cysts are uncommon. Multiple hydatid cysts may arise as a primary event or develop secondary to hydatid cyst rupture within the brain or elsewhere due to trauma or surgery (secondary). Such secondary cysts lack brood capsules and scolices and are infertile.[12]
Patients, usually children, with intracranial hydatid cyst present with features of raised intracranial tension due to mass effect of a large-sized cyst. Focal neurologic deficits, such as hemiparesis, visual disturbances, ataxia, and seizures, are other manifestations depending on the location of the cyst. Headache and vomiting are almost universally present along with bilateral papilledema.[123]
Imaging findings of the cerebral hydatid cyst are characteristic when a large intraaxial cyst filled with a fluid of cerebrospinal fluid (CSF)-like appearance is seen in the parietal lobe of the brain without any contrast enhancement and perilesional edema.[345] On CT, the hydatid cyst in the brain is seen a spherical cyst with homogenous fluid attenuation surrounded by a smooth, thin wall with the same density as the adjacent brain; septations and daughter cyst may be seen. Calcification of wall is present in about 1% of the cysts.[456] No edema is usually seen in the white matter surrounding the cyst. No wall enhancement is seen after injection of contrast. Wall enhancement and edema may be present in complicated cysts.[789] This aforementioned appearance is seen in hydatid cyst due to E. granulosus whereas those due to E. multilocularis have a more solid appearance and show enhancement.[7] Cerebral hydatid cysts (cystic echinococcosis [CE]) have been classified on the lines of WHO classification of hepatic hydatid cysts into five types.[10] CE 1 is a unilocular cyst with or without a wall containing no visible daughter cysts. CE 2 is a unilocular cyst with peripheral daughter cysts along the wall, the case under discussion belonged to this type. CE 3 type cyst shows multiple daughter cysts completely filling the parent cyst. Type CE 4 is characterized by the presence of detached membranes and CE 5 is a calcified cyst.
Differential diagnosis of cerebral hydatid cyst on CT is with arachnoid cyst, porencephalic cyst, neurocysticercosis (NCC), abscess, and pilocytic astrocytoma.[3579] MDCT helps in the preoperative diagnosis of cerebral hydatid cyst when characteristic findings are demonstrated, which include intraaxial location (in contrast to arachnoid cyst), spherical shape (in contrast to porencephalic cyst), without contrast enhancement (in contrast to abscess, astrocytoma, and NCC), and without adjacent gliosis/edema (as in porencephalic cyst, abscess).[679]
CT with both routine conventional CT and MDCT identifies calcification better than MRI. MDCT allows quite faster scanning than routine CT and is useful in the case of an irritable patient. It also helps in determining the exact size in all the three dimensions from the multiplanar reformations of high quality that are possible with modern MDCT. Mass effect and transtentorial and subfalcine herniation are depicted well by MDCT reconstructions in coronal and sagittal planes. Relationship of the cystic mass with important structures of the brain is also well shown by MDCT. Thus MDCT allows comprehensive preoperative evaluation of cerebral hydatid cyst and similar to MRI, it helps in the planning of surgical procedure. This usefulness of MDCT has a practical significance in situations when MRI is not available.
Treatment of cerebral hydatid cyst is surgery, which may be in the form of aspiration or more commonly separation of the cyst from adjacent brain with saline irrigation followed by the removal of the cyst in toto avoiding rupture.[12] Preoperative diagnosis of hydatid cyst with CT should alert the operating surgeon for exercising extreme care to avoid rupture of the cyst and hence recurrence.
Conclusion
Large spherical supratentorial intraaxial cyst without any perilesional edema and enhancement on CT in the brain of a child in an endemic area should suggest a diagnosis of cerebral hydatid cyst, which demands extra care to avoid any rupture during surgery. MDCT may help in comprehensive preoperative evaluation for surgical planning.
Source of Support: Nil,
Conflict of Interest: None declared.
References
- A large cerebral hydatid cyst associated with liver cyst. Ann Trop Paediatr. 2003;23:313-7.
- [Google Scholar]
- Intracranial hydatid cyst: A report of five cases and review of literature. Neurol India. 1999;47:214-7.
- [Google Scholar]
- Computed tomography of intracerebral echinococcal cysts in children. J Comput Assist Tomogr. 1985;9:514-8.
- [Google Scholar]
- Hydatid disease of the CNS: Imaging features. AJR Am J Roentgenol. 1998;171:1497-500.
- [Google Scholar]
- Magnetic resonance imaging of simple and infected hydatid cysts of the brain. Magn Reson Imaging. 2001;19:965-74.
- [Google Scholar]
- Cerebral hydatid disease: CT and MR imaging findings. Swiss Med Wkly. 2004;134:459-67.
- [Google Scholar]
- Magnetic resonance appearance of cerebral cystic echinococcosis: World Health Organization (WHO) classification. Acta Radiol. 2009;50:549-54.
- [Google Scholar]




