
Translate this page into:
Knowledge, attitude, and practice of people toward epilepsy in a South Indian village
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
People living with epilepsy continue to suffer from enacted or perceived stigma that is based on myths, misconceptions, and misunderstandings that have persisted for many years. In the last decade, there has been an increase in individual literacy rate and increased access to technology in rural population. However, it is unclear if this has any effect on knowledge, attitude, and practice (KAP) attitude toward epilepsy.
Objective:
Our primary aim is to evaluate KAP toward epilepsy. In addition, we also estimated the prevalence of stroke and epilepsy in rural South India.
Materials and Methods:
Using a 14-item questionnaire, we assessed KAP toward epilepsy and identified determinants of inappropriate attitudes toward people with epilepsy and 10-item questionnaires to assess the prevalence of epilepsy and stroke among 500 randomly selected populations in a Pattaravakkam village (Tamil Nadu, India).
Results:
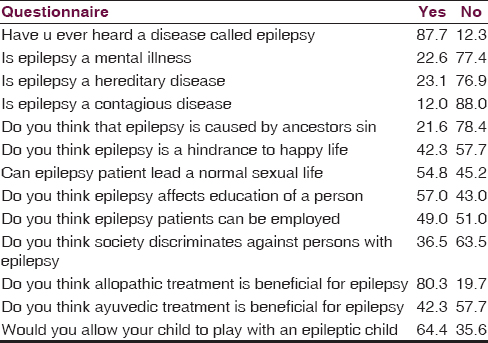
About 87.7% of the people had heard or read about epilepsy. Negative attitudes appeared to be reinforced by beliefs that epilepsy is hereditary (23.1%), kind of insanity (22.6%), or as contagious (12.0%). The knowledge about the clinical characteristics and first aid to a person during a seizure was 25.8%. About 36.5% of people think that society discriminates people with epilepsy. Moreover, our prevalence study showed that 8.7% people are suffering from epilepsy and 3.7% had stroke previously and at the day of survey, the stroke prevalence is 3.3%.
Conclusion:
Even with increased literacy, technology, and communication devices, the KAP of people toward epilepsy is relatively low. General public education campaigns and specific school education campaigns children should be encouraged to increase the KAP toward epilepsy. The prevalence and pattern of epilepsy and stroke is on the higher side in the village of Pattaravakkam. Future research regarding the value of targeted education in improving KAP will be worthwhile.
Keywords
Epilepsy
knowledge
attitude and practice
social stigma

Introduction
People with epilepsy are socially discriminated because of public attitudes, misunderstandings, and defensive behavior. Recently conducted knowledge, attitude, and practice (KAP) in developed country showed positive attitude,[123] but in developing countries, it is still highly a stigmatizing disease.[456]
In the last decade, there has been an increase in individual literacy rate and increased access to technology and communication devices in rural population. However, it is unclear if this has any effect on KAP toward epilepsy. Our primary aim is to evaluate KAP toward epilepsy. In addition, we also estimated the prevalence of stroke and epilepsy in rural South India.
Materials and Methods
This study was performed in the village of Pattaravakkam near Chennai, South India. It is comparable to any rural setting in India by having same level of literacy, health awareness, and health services. In this village, we performed a house-to-house survey for screening of cases; in addition to using uniform diagnostic criteria for epilepsy and stroke.
Area of study
The study was conducted in a village hamlet named Pattaravakkam located in Kattankulathur taluk, Kanchipuram district of Tamil Nadu in South India [Figure 1]. It is a village Panchayat comprising three villages namely Pattaravakkam, Thenur, and Ilanthoppe. It is a rural area having a population of 2500. It has one primary health center and one Government Primary School.

- Area of study: Pattaraivakkam village, Kanchipuram dist., Tamil Nadu, India. Courtesy: Google maps
Study population
The prevalence study was conducted among 500 people selected by stratified random selection from the village, whereas the KAP study was conducted only in people aged above 15 years.
Study design
The study was a two-staged door-to-door survey consisting of (a) preparatory stage and (b) survey stage.
Preparatory stage
One month before the start of survey, 20 medical students from Government Stanley Medical College under our leadership were trained at our institute on survey techniques, orientation to seizure disorders, method of interview, and recording of data. The most common false beliefs are related to mental retardation, mental illness, and emotional disturbances in patients.[7] In extreme cases, epilepsy could be perceived as possession by an evil spirit.[8] The objectives and rationale of the survey were discussed with the local villagers, responsible seniors, village chairman, and officials to enlist their cooperation and support. These measures yielded excellent public compliance ensuring high level of case ascertainment.
Survey stage
The actual survey was carried out in two phases.
Phase I (screening phase)
The first step of the investigation involved a door-to-door survey, which was carried from August through October 2008 in this survey, 20 medical students under our leadership carried out the survey and filled the questionnaire in local Tamil language by interviewing the people.
Phase II (diagnostic phase)
All of the collected data were analyzed by three neurologists experienced in epilepsy who searched for positive cases. Individuals with responses of epilepsy and stroke were requested to have an examination by the neurologists. The examinations were carried out on the day of the survey in a nearby Government Primary School.
Knowledge, attitude, and practice study
KAP studies have now become an integral part of community management of chronic illnesses associated with high level of stigma such as leprosy and epilepsy.[9] The KAP study for epilepsy was also conducted on the same day along with the prevalence study.
Questionnaire
The survey questionnaire contained 14 questions [Appendix 1]. All the questions were with simple yes or no responses. The questionnaire was also designed to cover KAP toward epilepsy. The questionnaire we used had been field tested in a pilot study.[10] The questionnaire was divided into three parts. The first part was developed to obtain the demographic characteristics of the population. The questions in the other part were developed to gather information on public understanding on attitudes toward epilepsy and to find the prevalence of epilepsy and stroke. The questionnaire was designed to ensure maximum sensitivity. The sensitivity and specificity of the questionnaire were 100% and 72%, respectively.[10]
Results
The demographic details of the study population are presented in Table 1. The responses to the questions are summarized in Table 2. The distribution of age, gender, and educational qualification is shown in Figures 2 and 3. The majority of respondents were unemployed 69.6% which include females and older people [Table 1] and was earning <1000 rupees/month (40.5%). Most of the people aged <20 years and in the third decade. The answers to the question “How would you attend a person during a seizure?” are provided in Figure 4.

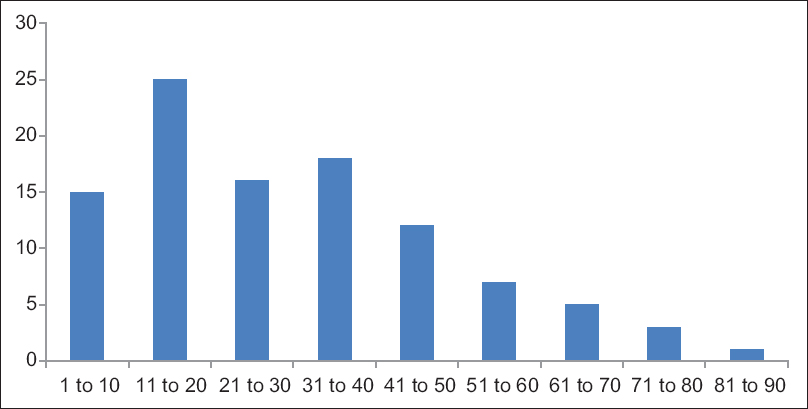
- Age Distribution of study population X axis shows age in numbers
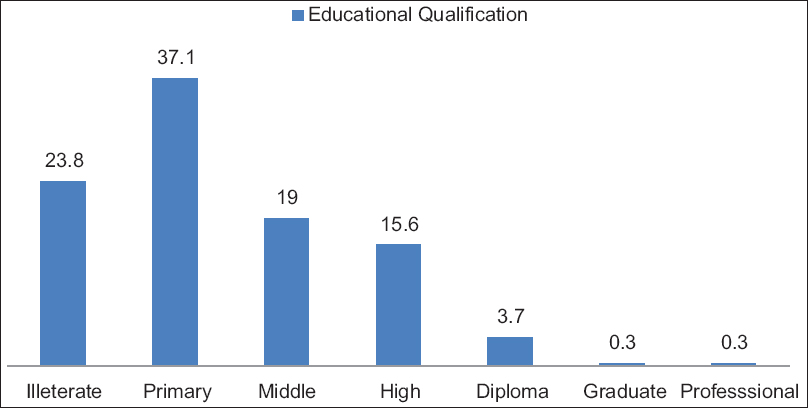
- Educational qualification of the study population
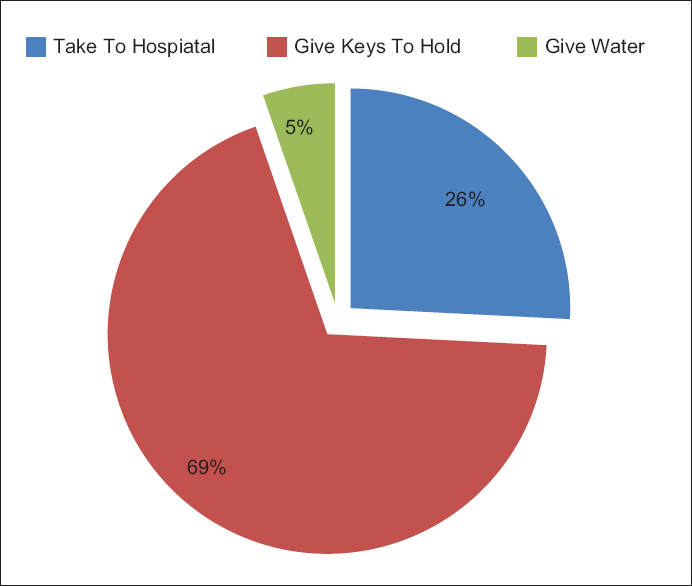
- What would you do if you happened to see a person getting an epileptic attack?
From our study, it has been found out that about 23.8% of the study population are illiterate. Majority of this group comprises females. Literacy has been described as the ability to read for knowledge and write coherently and thinks critically about the written word. Literacy can also include the ability to understand all forms of communication, be it body language, pictures, video, or sound (reading, speaking, listening, and viewing).
Knowledge, attitude, and practice study results
Knowledge: (Q1–5)
About 88.7% of people had heard about epilepsy. 68% of respondents believed correctly that epilepsy was caused by a brain disease. About 22.6% and 23.1% of the respondents thought epilepsy was a form of insanity and a hereditary disease, respectively, prevalent misconceptions were that epilepsy is hereditary 31%, is contagious 12%, and is a result of ancestor sin 21.6%. Of the 88% people who responded correctly by saying epilepsy is not a contagious disease, 93.72% are literates indicating the importance of education.
Attitude (Q6–10)
About 55% of the respondents felt that individuals with epilepsy could not be properly educated or employed. Majority of them believed that epilepsy is a hindrance to happy married (42.3%) and sexual life (54.8%). About 36% would object to their children having contact with epileptic children. Nearly half (36.5%) believed that society had discriminative attitude for epileptic patients.
Practice (Q11–14)
About 78% believed that an allopathic doctor should treat the person, and 64% believed that Ayurvedic treatment is also effective. In response to first aid measures for epileptic fits 25.8% preferred that person should be taken to a doctor, 69.9% respondents would make the person hold a bunch of keys to terminate the epileptic attack, 5.3% suggested water to be given [Figure 4]. Of the 25.8% who responded correctly, 51.5% are literates. 48.66% of educated responded incorrectly.
Prevalence study
Through a two-staged survey and analysis, we ascertained that about 8.7% of the study population had epilepsy. The highest age-specific prevalence rate of 28.6% occurred in the age group of 71–80 years. Sex-specific prevalence rates are not significantly differ (53.8% for males and 46.2% for females). About 87.7% of the KAP respondents had heard about epilepsy.
About 3.7% had a previous history of stroke. The prevalence rate for stroke on the day of survey was 3.3%. The sex distribution for people suffering from stroke is 50-50.
Discussion
Through this cross-sectional study, we investigated the KAP toward epilepsy, point prevalence of epilepsy and stroke in a geographical area in the village hamlet of Pattaravakkam near Chennai, South India. According to our stroke registry, lot of patients from this village suffered new strokes, and the reason was thought to be sedentary lifestyle of this population. This is the main reason behind selecting this village. We believe that our study achieved the three important requirements of an ideal epidemiological inquiry complete case ascertainment, well-defined population denominator, and reasonable level of diagnostic precision. Measures we undertook well in advance of the survey to enlist participation and utilization of the questionnaire with 100% sensitivity in the screening survey enhanced case ascertainment. Because of the lower specificity of the questionnaire, the number of people suspected of having an epileptic disorder was several folds more than the actual. Evaluation by a neurologist with special interest in seizure disorder and stroke ensured an average level of precision. Before a health education program can be established, the beliefs and behaviors of the target population with respect to the disease in question must first be identified. Lennox suggested that public health workers needed to be acquainted with the public perception on a given illness.[11]
The knowledge, attitude, and practice study
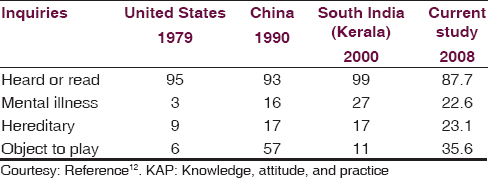
Several studies have investigated public awareness and attitudes toward epilepsy in both developed[23121314] and developing countries[45615] The results of these studies are not strictly comparable because the population studied and the questionnaires and methods used were different. The attitude toward epilepsy among the population of Pattaravakkam near Chennai was far more negative than those of developed countries [Table 3], probably due to lower literacy rate. The percentage of respondents who thought was epilepsy was a form of mental illness, who objected to their children playing with a child with epilepsy and who objected to employing a person with epilepsy were 22.6%, 33.5%, 51%, respectively, in our study compared with 3%, 0.6% and 9% in the united states.[12]
Nearly one-half of our respondents believed that persons with epilepsy could not have a healthy sexual life. This attitude in our population may be related to their belief that epilepsy is a hereditary and mental illness. Almost one-half of study population epileptics cannot be educated or employed as others. Most people in our study preferred the advice of allopathic although Ayurvedic medicines are accepted by a large segment of this South Indian population. Studies from developing countries[415] have revealed an awareness rate comparable to those from developed countries,[312] this high degree of awareness about epilepsy among the developing countries may be related to increased access to communications via telephone and television.
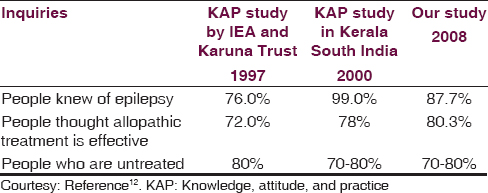
Based on our observations and review of the literature, it is evident that misconceptions about epilepsy, such as confusion between epilepsy and insanity and overemphasis of the role of heredity, are widely prevalent. Public attitudes toward epilepsy change slowly [Table 4]. Furthermore, awareness does not always equate to increased understanding or acceptance.[16] These nonscientific conceptualizations of epilepsy are responsible for the sociocultural stigma and resultant discrimination against persons with epilepsy. Persistent and effective information campaigns, therefore, are necessary to change public attitudes toward persons with epilepsy.
The prevalence study
Community-based prevalence studies have documented the crude prevalence of epilepsy from 247 to 883, for stroke 55–150/100,000 in overall population.[17] The estimated number of persons with epilepsy in India is approximately 5.5 million, among whom approximately 4.1 million reside in rural areas.[10] Prevalence of epilepsy is 2–25 times higher in developing countries on comparing developed countries.[10] This difference may be apparent (misdiagnosis, inconsistent definition, failure to take into account the disease activity) or real (illiteracy, poverty, poor sanitation, inaccessibility to medical care, cysticercosis.)[18] Hauser[16] estimated an average prevalence rate of 5.2/1000 population. Some community studies from North Central and South India have shown a prevalence rates per 1000 population of 2.5 for Kashmir,[19] 3.6 for the Parsis in Bombay,[20] and 4.4 for Bengaluru.[21]
Sridharan and Murthy[22] recently undertook a meta-analysis of the prevalence data obtained from 20 community-based studies on epilepsy in India. After correction for heterogeneity related to interstudy variation, the overall age-adjusted prevalence rate per 1000 was 5.3 (95% confidence interval [CI] 4.3–6.4). The prevalence rate for urban areas was 5.1 (95% CI, 3.5–6.7), 5.5 for rural areas (95% CI, 4.0–6.9), and men and women were 5.9 (95% CI, 3.9–7.9) and 5.5 (95% CI, 3.5–7.3), respectively. Regional causal factors such as cysticercosis and hot water epilepsy might have influenced the high prevalence rates reported in some studies from developing regions.[923]
From our study, the prevalence rate of epilepsy and stroke were was 8.7% and 3.3%, respectively. This appeared to higher than the national average. The age-specific prevalence rates in our study peaked in seventh decade similar to that of developed countries, and the prevalence seems to be increasing with the age.[24252627] However, in developing countries, the prevalence rate in elderly is lower, which may be attributed to lower life expectancy, higher seizure-related mortality.[922] It is possible that there is a sampling bias, people with medical conditions are staying at home and are available for surveys.
Limitations
Community-based survey has a lot of limitations on its part against the advantages. Some of the factors limiting the accuracy of our study are:
-
Inability of the people to interpret the questions rightly and respond to them
-
Associated stigma may result the neglect of report of seizures by individuals
-
Incidence and prevalence rates may vary if age-specific rates are not calculated, since the occurrence of epilepsy differs in different age group, sampling bias.
Conclusion
Even with increased literacy, technology, and communication devices, the KAP of people toward epilepsy is relatively low. General public education campaigns and specific school education campaigns children should be encouraged to increase the KAP toward epilepsy. The prevalence and pattern of epilepsy and stroke are on the higher side in the village of Pattaravakkam. Future research regarding the value of targeted education in improving KAP will be worthwhile.
Even with increased digitalization of the world and increased communications with television and mobile phone the KAP toward epilepsy are not up to the expected level. Literacy rates seem to have a significant effect on the KAP toward epilepsy. Solutions to this issue would be to increase literacy rates in India. In addition to increasing the overall literacy rate, there seems to be a clear need for general public education campaigns, and educating children should be encouraged to increase the KAP toward epilepsy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A survey of public attitudes toward epilepsy in 1974 with an indication of trends over the past twenty-five years. Epilepsia. 1974;15:523-36.
- [Google Scholar]
- Public attitudes toward epilepsy in Italy: Results of a survey and comparison with U.S.A. and West German data. Epilepsia. 1985;26:221-6.
- [Google Scholar]
- Survey of public awareness, understanding, and attitudes toward epilepsy in Henan province, China. Epilepsia. 1990;31:182-7.
- [Google Scholar]
- Knowledge, attitude, and practice toward epilepsy among rural Tanzanian residents. Epilepsia. 1993;34:1017-23.
- [Google Scholar]
- Public awareness, understanding & attitudes toward epilepsy. Indian J Med Res. 1995;102:34-8.
- [Google Scholar]
- Changes in public attitudes toward epilepsy in Hungary: Results of surveys conducted in 1994 and 2000. Epilepsia. 2001;42:86-93.
- [Google Scholar]
- Public awareness, attitude, and understanding of epilepsy in Hong Kong special administrative region, China. Epilepsia. 2002;43:311-6.
- [Google Scholar]
- Epidemiology of epilepsy in developing countries. Bull World Health Organ. 1993;71:247-58.
- [Google Scholar]
- Prevalence, knowledge, attitude, and practice of epilepsy in Kerala, South India. Epilepsia. 2000;41:1027-35.
- [Google Scholar]
- Effects of an educational campaign to change employer attitudes toward hiring epileptics. Epilepsia. 1972;13:87-96.
- [Google Scholar]
- A survey of public attitudes toward epilepsy in 1979 with an indication of trends over the past thirty years. Epilepsia. 1980;21:509-18.
- [Google Scholar]
- Public awareness and attitudes toward epilepsy in Finland. Epilepsia. 1980;21:413-23.
- [Google Scholar]
- Survey of public awareness, understanding, and attitudes toward epilepsy in Taiwan. Epilepsia. 1995;36:488-93.
- [Google Scholar]
- Prevalence of dementia in an urban Indian population. Int Psychogeriatr. 2001;13:439-50.
- [Google Scholar]
- Epilepsy in the tropics: II. Clinical presentations, pathophysiology, immunologic diagnosis, economics, and therapy. Epilepsia. 1996;37:1128-37.
- [Google Scholar]
- Prevalence and pattern of epilepsy (Lath/Mirgi/Laran) in rural Kashmir, India. Epilepsia. 1988;29:116-22.
- [Google Scholar]
- The Yelandur study: A community-based approach to epilepsy in rural South India – Epidemiological aspects. Seizure. 1998;7:281-8.
- [Google Scholar]
- Epilepsy in the tropics: I. Epidemiology, socioeconomic risk factors, and etiology. Epilepsia. 1996;37:1121-7.
- [Google Scholar]
- Descriptive epidemiology of epilepsy: Contributions of population-based studies from Rochester, Minnesota. Mayo Clin Proc. 1996;71:576-86.
- [Google Scholar]
- Epilepsy in a population of 6000 re-examined: Secular trends in first attendance rates, prevalence, and prognosis. J Neurol Neurosurg Psychiatry. 1995;58:570-6.
- [Google Scholar]
- Prevalence of epilepsy in rural Iceland: A population-based study. Epilepsia. 1999;40:1529-34.
- [Google Scholar]
Appendix 1: Questionnaire
Have u ever heard a disease called epilepsy? (1) Yes (2) No Is epilepsy a mental illness? (1) Yes (2) No Is epilepsy a hereditary disease? (1) Yes (2) No Is epilepsy a contagious disease? (1) Yes (2) No Do you think that epilepsy is caused by ancestors sin? (1) Yes (2) No Do you think epilepsy is a hindrance to happy life? (1) Yes (2) No Can epilepsy patient lead a normal sexual life? (1) Yes (2) No Do you think epilepsy affects education of a person? (1) Yes (2) No Do you think epilepsy patients can be employed? (1) Yes (2) No Do you think society discriminates against persons with epilepsy? (1) Yes (2) No Do you think allopathic treatment is beneficial for epilepsy? (1) Yes (2) No Do you think Ayurveda treatment is beneficial for epilepsy? (1) Yes (2) No Would you allow your child to play with an epileptic child? (1) Yes (2) No What would you do if you happened to see a person getting an epileptic attack? (a) Water (b) Keys (c) Admit to hospital
Modified WHO questionnaire for screening of epilepsy and stroke
Have you ever lost consciousness or fallen unexpectedly? (1) Yes (2) No Have you ever had episodes in which you have lost contact with your surroundings? (1) Yes (2) No Have you ever had uncontrolled shaking of hands and legs? (1) Yes (2) No Have you ever lost control of your bowel and bladder? (1) Yes (2) No Have you ever had episodes of blank spells with staring look or strange behavior? (1) Yes (2) No When awake, have you ever had very brief episodes of sudden jerking of arms and legs? (1) Yes (2) No Are speech slurred/face droopy? (1) Yes (2) No Is one side weak or numb? (1) Yes (2) No Is vision all or partly lost? (1) Yes (2) No Is headache severe? (1) Yes (2) No




