
Translate this page into:
Isolated Discitis in Melioidosis: An Unknown Presentation and a Microbiological Challenge

Chittur Viswanathan Gopalakrishnan, MCh Department of Neurosurgery, Aster Medcity, Cheranalloor Kochi, Kerala 682027 India drgopal1976@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Burkholderia pseudomallei causes Whitmore’s disease or melioidosis which is endemic in many South Asian countries including India. This gram-negative bacterium is frequently found in the moist soil and agricultural workers get infected most commonly. Most of the infections are asymptomatic and have a wide spectrum of manifestations as in tuberculosis. Melioidosis of the spine manifests as spondylodiscitis with paravertebral and prevertebral abscess and presentation as discitis alone is not reported. We report the first case of melioidosis causing isolated discitis without any obvious bony involvement. It also highlights the need for preoperative suspicion of these rare manifestations even in seemingly innocuous disc disease presenting as back pain and radiculopathy.
Keywords
spondylodiscitis
melioidosis
Burkholderia pseudomallei
infection

Case Report
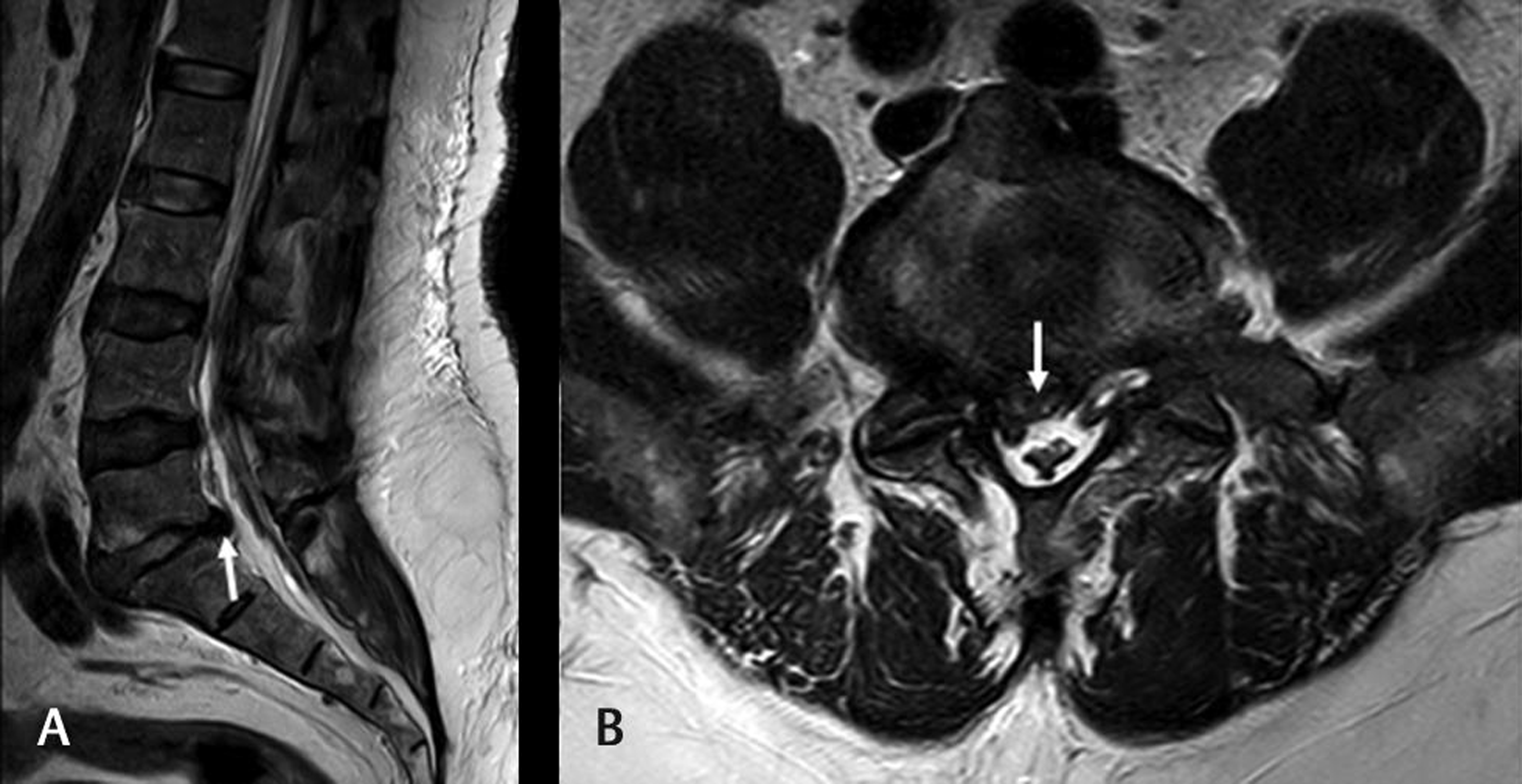
A 58-year-old obese man, known diabetic and hypertensive, presented with low back and bilateral lower limb pain of 4 weeks duration, more symptomatic on the left side. The pain did not improve with conservative measures. Neurological examination revealed bilateral positive straight leg raising test with pain radiating along S1 dermatome, more on the left side. Magnetic resonance imaging of the lumbosacral spine showed multilevel disc degeneration involving the lumbar spine with bilateral lateral recess stenosis at L5–S1. There was evidence of nerve root compression and type II Modic changes of L5 vertebral body suggesting a long-standing degenerative pathology (Fig. 1). In view of severe unrelenting radicular pain, the patient underwent minimally invasive L5–S1 discectomy thus decompressing both the nerve roots via a unilateral approach. The disc material at L5–S1 was not typical of a degenerative pathology. It was soft and mucinous in consistency and suspecting infection, and was sent for histopathology and bacterial cultures. Postsurgery he was also evaluated for sepsis which was unremarkable except for erythrocyte sedimentation rate which was above normal limits. Bacterial culture from the disc material yielded growth of gram-negative bacilli which was identified by Vitek 2-based automated microbial identification and antibiotic susceptibility testing system (BioMerieux) as Burkholderia pseudomallei (causative agent of melioidosis) and isolate was sent to the referral lab for confirmation. Referral lab confirmed the diagnosis based on molecular analysis (TTSS1 gene). He was started on intravenous ceftazidime 2 g thrice daily and cotrimoxazole was added after 2 weeks. The patient could not tolerate cotrimoxazole due to severe gastritis and hyponatremia and hence intravenous ceftazidime 2 g thrice daily was continued for a period of 3 months. On review at 6 months, the patient was asymptomatic and had normal functional status.
-
Fig. 1 T2-weighted sagittal (A) and axial (B) images of lumbosacral spine showing diffuse disc bulges with disc prolapse at L5–S1 (arrow) causing lateral recess stenosis and nerve root impingement.
Fig. 1 T2-weighted sagittal (A) and axial (B) images of lumbosacral spine showing diffuse disc bulges with disc prolapse at L5–S1 (arrow) causing lateral recess stenosis and nerve root impingement.
Discussion
Melioidosis is an infection caused by a gram-negative bacillus called B. pseudomallei which is commonly found in soil and groundwater.1 2 The bacteria enter the body through wounds, inhalation, or ingestion and percutaneous inoculation is the most common mode of spread. The risk factors predisposing to infection include diabetes, alcoholism, chronic renal, and lung diseases.3 Melioidosis can have an acute, subacute, or chronic clinical presentation and can affect any organ system in the human body thus mimicking tuberculosis. Spinal involvement is very rare and occurs by hematogenous spread via the vascular or lumbar venous plexus.4 It can present in the form of spondylitis, paravertebral, or as epidural abscesses hence resembling tuberculosis.3 Arockiaraj et al5 after analyzing a total of 1,100 patients of spondylitis documented only four cases of melioidosis, wherein all four were diabetic. Unlike our case, they presented with fever and constitutional symptoms such as loss of weight and appetite and had multiple abscesses which were aspirated thus confirming the diagnosis. Garg et al6 reported a case of melioidosis and emphasized on additional tests before labeling it as “smear-negative tuberculosis.”
Laboratory diagnosis of melioidosis includes polymerase chain reaction-based diagnostics and rapid specific identification technologies such as gene sequencing and matrix-assisted laser desorption ionization time-of-flight mass spectrometry.7 The chances of mortality following inadequate treatment are very high as the pathogen is very aggressive. All melioidosis cases are recommended for initial intensive therapy using ceftazidime or meropenem followed by a period of eradication therapy using cotrimoxazole.1
Our patient presented clinically with symptoms typical for a degenerative disc disease with radiculopathy for which he underwent lumbar discectomy. The consistency of the disc material prompted us to send for a microbiology work-up. There was no reason to suspect this disease prior to surgery in view of the absence of any systemic manifestations that has been routinely reported by other authors in this condition. The patient clinically did extremely well after the completion of antibiotic treatment.
Conclusion
Several case reports in previous literature mention predominant bony involvement with abscess formation as the spinal manifestation of melioidosis.5 6 Our case report for the first time documents isolated disc involvement without adjacent bony disease or abscess formation in melioidosis thus mimicking degenerative disc disease. Melioidosis should be thought of as an important differential diagnosis when discitis is being suspected in patients presenting with back pain.
Conflict of Interest
None declared.
Authors’ Contributions
J.E.M. was the chief operating surgeon and under whom the patient was admitted. A.V. had assisted the case and was the one who had collected the data and has written the manuscript. C.V. Gopalakrishnan was also involved in writing and editing the manuscript. A.W. was involved in microbiological diagnosis and suggesting antimicrobial management strategies for this patient.
References
- The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS Negl Trop Dis. 2010;4(11):e900.
- [Google Scholar]
- Melioidosis: a major cause of community-acquired septicemia in northeastern Thailand. J Infect Dis. 1989;159(5):890-899.
- [Google Scholar]
- Burkholderia pseudomallei causing bone and joint infections: a clinical update. Infect Dis Ther. 2016;5(1):17-29.
- [Google Scholar]
- Non-caseating granulomatous infective spondylitis: melioidotic spondylitis. Asian Spine J. 2016;10(6):1065-1071.
- [Google Scholar]
- Melioidosis: the great mimicker presenting as spondylodiscitis. BMJ Case Rep. 2018;2018:bcr-2017–223223.
- [Google Scholar]
- Matrix-assisted laser desorption ionization-time of flight mass spectrometry for rapid identification of Burkholderia pseudomallei: importance of expanding databases with pathogens endemic to different localities. J Clin Microbiol. 2012;50(9):3142-3143.
- [Google Scholar]




