
Translate this page into:
Intraventricular Bleed following Surgery for Giant Cystic Vestibular Schwannoma: A Rare Complication
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Surgery for large vestibular schwannomas is associated with a small risk of postoperative local or remote hematomas. We describe a rare location of postoperative bleed into the ventricular system following surgery for a cystic vestibular schwannoma, from which the patient could not be salvaged.
A 40-year-old woman presented with left hearing loss, left cerebellar signs, and lower cranial nerve involvement. Magnetic resonance imaging demonstrated a giant (longest length >4.5 cm) cystic left vestibular schwannoma [Figure 1]. She underwent left retromastoid suboccipital craniectomy and excision of the lesion. Facial nerve could not be preserved. Surgery was uneventful, and the brain was lax, after achieving meticulous hemostasis dura and wounds were closed. However, the patient was in altered sensorium and flexing to pain postreversal from anesthesia. Immediate computed tomography scan head revealed a postoperative hematoma which was seen in the cerebellopontine angle; surprisingly, the hematoma had tracked into the 4th ventricle resulting in a large 4th ventricle bleed extending into the lateral and third ventricles [Figure 2]. She underwent a midline suboccipital craniectomy and evacuation of the 4th ventricle bleed along with external frontal ventricular drain. She was ventilated in the Intensive Care Unit but unfortunately her sensorium did not improve, and over 5 days, her condition further worsened and she expired.
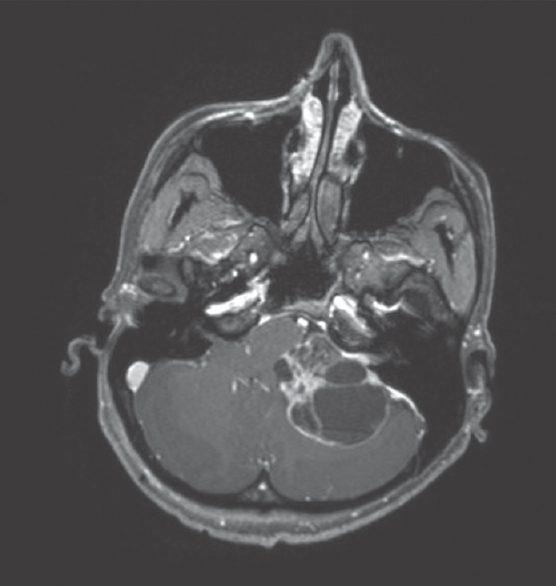
- Magnetic resonance imaging brain axial T1-weighted contrast images showing a left cystic vestibular schwannoma
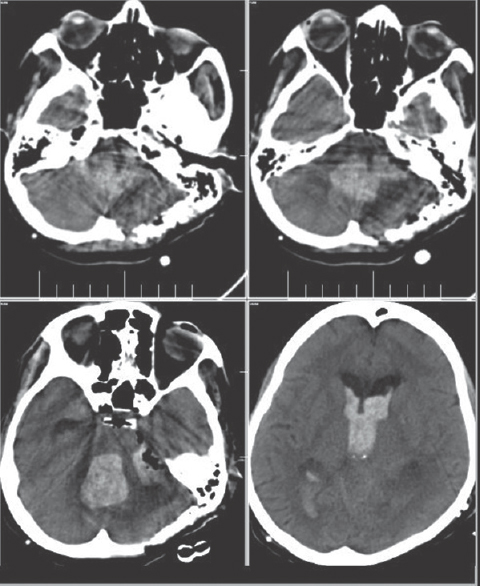
- Postoperative computed tomography scan showing blood predominantly in the ventricles with a small operative-site hematoma
Postoperative hematomas after surgery for vestibular schwannomas are uncommon but well known. Sade et al. reported a 2% (7 out of 338 cases) incidence of hematoma following suboccipital retrosigmoid approach for these tumors.[1] They are associated with significant mortality and morbidity. They may be more common with cystic vestibular schwannoma as in our case.[2] The reported sites of hematomas include operative site, cerebellar parenchyma, brainstem hematomas, operative-site extradural hematomas, and remote supratentorial hematomas such as supratentorial extra- and sub-dural hematomas.[134] The causes may be due to inadequate hemostasis, retraction injury, venous infarction, excess drain of cerebrospinal fluid, or vascular injury during surgery. In our case, blood was predominantly in the ventricular system and this location of hematoma has not yet been described in literature. On retrospective analysis of the surgical video, it was found that there was a small arterial vessel which was bleeding from the choroid plexus at the foramen of Luschka, it was controlled with cottonoid pressure. This vessel could have retracted and continued to bleed, causing the blood to track through the Luschka enter the 4th ventricle and ascend to involve the supratentorial ventricles.
This case illustrates that the 4th ventricular bleed can occur following retrosigmoid surgery and bleeding may not be evident at the operative site. As the blood tracks into the ventricular system, immediate brain bulge may not occur and the surgeon may not suspect an ongoing bleed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Vascular complications of vestibular schwannoma surgery: A comparison of the suboccipital retrosigmoid and translabyrinthine approaches. J Neurosurg. 2006;105:200-4.
- [Google Scholar]
- Management of 1000 vestibular schwannomas (acoustic neuromas): Surgical management and results with an emphasis on complications and how to avoid them. Neurosurgery. 1997;40:11-21.
- [Google Scholar]
- Current results of the retrosigmoid approach to acoustic neurinoma. J Neurosurg. 1992;76:901-9.
- [Google Scholar]
- Removal of large acoustic neurinomas (vestibular schwannomas) by the retrosigmoid approach with no mortality and minimal morbidity. J Neurol Neurosurg Psychiatry. 2004;75:453-8.
- [Google Scholar]




