
Translate this page into:
Fully endoscopic supraorbital keyhole approach to the anterior cranial base: A cadaveric study
Address for correspondence: Dr. Mehmet Osman Akçakaya, Taksim Training and Research Hospital, Department of Neurosurgery, Osman Bey Street, No. 120, Gaziosmanpasa, Istanbul - 34255, Turkey. E-mail: moakcakaya@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
The supraorbital keyhole approach for anterior cranial base lesions has been increasingly used in clinical practice. Anatomical studies focusing on the endoscopic anatomy via this approach are few, although the microscopic anatomy has been well studied. The aim of this study is to describe the anatomical features and surgical exposure provided by the endoscopic supraorbital keyhole approach using quantitative measurements.
Materials and Methods:
Nine formalin-fixed human cadavers from the inventory of the Anatomy department were used. A total of 18 supraorbital keyhole cranitomies were conducted. The distances between the target anatomical structures and the dura mater at the craniotomy site, and the distances between deep anatomical structures were measured with purpose-designed hooks.
Results:
The distance between the dura mater and optic canal was measured as 69.5 ± 6.7 mm (62–83 mm); optic chiasm as 76.2 ± 5.4 mm (67–86 mm); anterior communicating artery as 82.6 ± 6.1 mm (71–93 mm); internal carotid artery (ICA) bifurcation as 74.7 ± 6.0 mm (66–84 mm) and the basilar tip as 94.9 ± 7.0 mm (87–111 mm). The mean diameter of the optic canal was 7.4 ± 1.3 mm (6–11 mm), whereas the mean diameter of diaphragma sellae was measured as 8.4 ± 1.1 mm (7–10 mm).
Conclusions:
The results of this study showed that the anterior and medial aspects of the anterior cranial fossa can be visualized properly. Dissection of the ipsilateral arteries of Circle of Willis can be performed easily using an endoscopic supraorbital keyhole approach.
Keywords
Anterior cranial base
full-endoscopic
neuroendoscopy
skull base
supraorbital keyhole approach

Introduction
The supraorbital ridge resection was first used by Frazier in 1913 to operate on a pituitary tumor.[1] In 1982, Jane et al. described a supraorbital approach suitable for the resection of sellar–parasellar tumors, anterior communicating aneurysms, craniophryngiomas and olfactor groove meningiomas.[2] The supraorbital keyhole craniotomy technique through a ciliary incision was very well defined with technical refinements by Perneczky and co-workers in various publications.[345]
Today, various microsurgical approaches are being defined to access the anterior cranial base.[6] Pterional, uni- or bilateral subfrontal, orbitofrontal and orbitozygomatic approaches have been used with considerably low-complication rates. However, there is a recent trend in neurosurgery with the development of neuroimaging, neuroendoscopy and neuronavigation techniques that has lead surgeons to tailor a less invasive surgical approach for patients with minimal exposure.[7] Classical approaches with wide exposures were claimed to have some disadvantages: A significant degree of brain retraction, unnecessarily wide surgical dissection, some degree of temporal muscle dissection even if there is no need for temporal bone resection and bad cosmetic results.[46891011121314]
In the last two decades, with the evolution of endoscopes with improved optical and illumination quality and the development of new endoscopic instruments, endoscopic approaches to the anterior skull base have become increasingly popular. The endoscopic endonasal transphenoidal approach has become a significant alternative to the microsurgical transseptal transsphenoidal approach and is even replacing it nowadays.[1516] The endoscope provides better illumination, much wider operative view, higher magnification and the ability to “see around the corner.”[1516] With the modifications to the endoscopic endonasal transsphenoidal approach, extensive surgery for anterior cranial base pathologies has become possible.[16] However, these “extended” approaches are related to some serious complications such as cerebrospinal fluid (CSF) fistulas or diffuculties on secondary surgery, due to severely disturbed anatomy.[16] Therefore, the supraorbital keyhole approach has become an alternative in the management of anterior skull base lesions and anterior circulation aneurysms, due to its minimal invasive nature and relatively low complication rates.[513141617]
Recently, there have been a significant number of clinical studies published related to endoscopic, microscopic or endoscopy-assisted microscopic supraorbital keyhole approach for anterior and middle skull base lesions. Also, the microsurgical anatomy via supraorbital keyhole approach was well studied.[456789101314161718192021222324] However, there are few cadaveric studies related to the endoscopic anatomy of the anterior skull base.[15252627] The aim of this study is to define the endoscopic anatomy of the anterior skull base, with measurements of distances between target anatomical structures and the dura mater at the craniotomy site and distances between deep anatomical structures.
Materials and Methods
Nine formalin-fixed cadaver heads from the inventory of the Anatomy Department of Istanbul, School of Medicine were used. All anatomical dissections were performed at the Microneurosurgery Laboratory of the Neurosurgery Department of Istanbul Medical School. A total number of 18 supraorbital keyhole craniotomies through eyebrow incisions were performed. A rigid endoscope 2 mm in diameter and 26 cm in length with 0- and 30-degree lenses (Karl Storz Gmbh and Co, Tutlingen, Germany) was used. The endoscopic dissection procedures were recorded with a video camera, which was connected to a flat screen monitor and pictures were taken with the “snapshot” feature (Karl Storz Gmbh and Co, Tutlingen, Germany). The length of the eyebrow incision, the size of the craniotomy and (in case) the opening of frontal sinus were recorded. The measurements were made from the dura mater at craniotomy site with the help of constant bony landmarks to the target structures. The target structures were the internal carotid artery (ICA) bifurcation, anterior communicating artery (ACommA), optic chiasm, optic canal and the basilary tip. The distances were measured with the use of endoscope itself. Zero-degree endoscope lens was hold against the target structure under direct visualization, and then the endsocope shaft was marked with a highlighter surgical pen. The endoscope was removed and the distance between the mark and lens was measured. All the measurements were made from the dura at the anterior border of the orbital roof. Also, distances between deep-seated anatomical structures were measured with the help of purpose-designed hooks. Two special hooks of 22 cm in length were designed for the measurements (MEG medikal, Istanbul, Turkey). One hook has a 2 cm, 45-degree end on one side with a (15 mm) milimetric scale and a 2 cm, 90-degree end on the other side with a (10 mm) millimetric scale. The other hook has a 2 cm, 30-degree end on one side with a (8 mm) milimetric scale and a 2 cm, 90-degree end on the other side with a (8 mm) milimetric scale. Both of the hooks were made from a bendable material in order to adapt to different surfaces [Figure 1]. The distances between ICA bifurcation and optic chiasm, the two optic canals, the vertical distance between the diaphragma sellae and optic chiasm, the diameter of the optic canal and diaphragma sellae were measured with the use of these purpose-designed hooks.
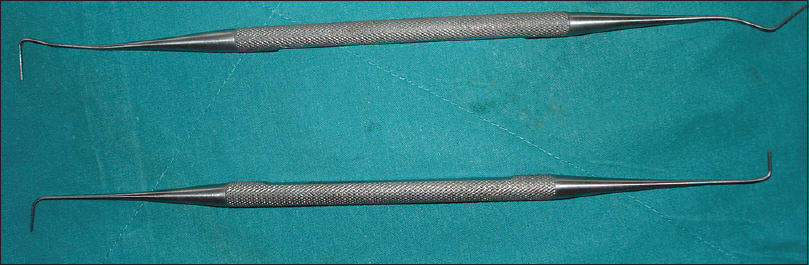
- Two special hooks 22 cm in length were designed for the measurements between deep-seated anatomical structures. (MEG medikal, Istanbul,Turkey) One hook has a 2cm, 45-degree end on one side with a (15 mm) milimetric scale and a 2 cm, 90-degree end on the other side with a (10 mm) millimetric scale. The other hook has a 2 cm, 30-degree end on one side with a (8 mm) milimetric scale and a 2 cm, 90-degree end on the other side with a (8 mm) milimetric scale. Both of the hooks were made from a bendable material in order to adopt to different surfaces
Endoscopic supraorbital keyhole approach
The head was positioned with 15 degrees mild extension and rotated 20 degrees away from the side of the approach to simulate the real surgical position. The supraorbital notch was found with palpation and marked. A skin incision starting from the lateral aspect of the supraorbital notch reaching to the pterion was made within the eyebrow [Figure 2]. The orbicularis oculi, temporal and frontal muscles were exposed. The frontal muscle was sharply dissected with an 11-blade knife parallel to the supraorbital margin and temporal muscle was bluntly dissected with a periostal elevator vertically to the temporal line. The frontal and orbicularis oculi muscles were bluntly dissected. A burr hole was opened at the pterion below the temporal line using a high-speed drill with a 5 mm diameter ball fluted bit (Midas Rex Legend, Medtronic Inc., Minneapolis, MN, USA). The craniotomy 2.2–3.0 cm wide and 1.3–1.7 cm high was performed [Figure 3]. The dura was opened in a C-shaped fashion based on the orbital roof [Figure 4]. The orbital roof and interior margins of the craniotomy were thinned using the drill to provide wider working angles for the endoscope. The frontal pole was retracted with a 9 mm brain retractor and the 2 mm 0-degree endoscope was inserted into the anterior cranial fossa intradurally. The following structures were all visualized with 0 degree lens endoscopes: Olfactory bulb, olfactory tract, both optic nerves at the optic canal, optic chiasm, liliequist membrane, A1 and A2 segments of both anterior cerebral arteries (ACA), ACommA, ICA bifurcation, middle cerebral artery (MCA), posterior communicating artery (PCommA) and anterior choroidal artery [Figure 5]. The infundibulum and diaphragma sellae were visualized with the 30-degree lens endoscopes [Figure 6]. The MCA was followed distally and M2 segment superior and inferior trunks of MCA were exposed. Between the ICA bifurcation and oculomotor nerve the endoscope was advanced into the interpedincular cistern. The basilary artery (BA), basilary tip, both posterior cerebral arteries (PCA) and PCommA were exposed.

- Skin incision and frontal nerve within the supraorbital notch

- Supraorbital keyhole craniotomy

- C-shaped dural opening with its base on the orbital roof

- View of the internal carotid artery (ICA), M1 segment of the middle cerebral artery (MCA), A1 segment of the anterior cerebral artery (ACA) and the liliequist membrane (LM) after the opening of the carotid cistern

- Following the opening of the chiasmatic cistern, diaphragma sellae and infundibulum were exposed with the use 30 degree lense endoscope
Results
The mean length of the skin incision was 3.68 ± 0.19 cm (range, 3.4–4 cm). The mean width of the craniotomy was 2.65 ± 0.23 cm (range, 2.2–3 cm), whereas the mean height was 1.43 ± 0.12 cm (range, 1.3–1.7 cm). In 5 of 18 craniotomies, the frontal sinus was opened reluctantly. In three of these craniotomies the frontal sinus opening was less than 1 cm, in one craniotomy between 1 and 2 cm and in one it was greater than 2 cm. The data involving skin incision length, craniotomy size and the frontal sinus opening are summarized in Table 1.

Severe cerebral atrophy and collapse in vascular structures were observed in all of the formalin-fixed cadaver heads. Despite the identification of the olfactory bulb at lamina cribrosa level, the olfactory tract was proximally detached in most of the cadavers and the olfactory nerve was found seperated on the surface of the straight gyrus, probably due to frontal lobe retraction. There was easy visualization of the bilateral orbital rooves, ethmoid bone, sphenoid planum and tuberculum sellae. The distances between the dura at the craniotomy site and target structures are summarized in Table 2. In all cadavers, the M1 segment of MCA was followed and the MCA bifurcation was identified. The temporal poles, both on the ipsi- and contralateral side, were easily visualized. We observed that all anatomic structures located anteriorly and superiorly to these landmarks could be well visualized.

For the measurements of deep-seated structures, a 30-degree endoscope provided more direct visualization, especially for the diaphragma sellae and infundibulum. The diameters of the target structures and distances between different deep-seated structures are summarized in Table 3.

After the opening of the interpedincular cistern, the basilary tip and proximal parts of the bilateral PCA were well visualized and bilaterally, the posterior communicating arteries (PCommA) were identified. It was observed that for an effective working space to make dissections within this cistern, orbital roof drilling provides an adequate maneuverability.
Discussion
The supraorbital keyhole approach drew attention due to its limited surgical exposure, minimal brain retraction due to CSF drainage from the chiasmatic, carotid cisterns and frontal lobe relaxation with gravity related to surgical positioning.[26142021] Good cosmetic results, better surgical view, shorter hospital stay and lower general costs are other advantages.[62021] The main concerns related to this approach are limited surgical maneuverability and difficulties in changing surgical strategy if needed.[14]
The vast majority of clinical series related to the supraorbital keyhole approach include only microsurgical or endoscopy-assisted microsurgical techniques.[3459121416192224] Today, with advances of the endoscope technology, full-endoscopic supraorbital keyhole approach is also used for the surgical resection of various pathologies, including anterior circulation aneurysms, most of the anterior cranial base lesions and with additional bone resection and drilling, middle cranial base lesions.[6172021] It was stated that this approach carries a lesser risk of CSF fistula compared with extended endonasal trans-sphenoidal approaches.[16] Although there is a significant number of clinical studies related to the supraorbital keyhole approach, the number of anatomical studies are relatively few.[101518252627] Recent studies are more focused on the working space provided by the supraorbital keyhole approach and its comprasion with conventional craniotomies.
Figueiredo et al. compared the surgical working area provided by three different craniotomies, namely supraorbital keyhole, pterional and orbitozygomatic craniotomies in a cadaveric study.[10] They used a frameless stereotactic device to calculate the working area in mm2 and found that there was no statistically significant difference among these three craniotomies. However, the working corridor, angular exposure in the vertical and horizontal axes for supraorbital approach was found lesser compared with the other approaches. Another cadaveric study by Cavalcanti et al. compared the surgical freedom, working area for specific targets and working angles provided by supraorbital keyhole craniotomy alone or with an additional orbital osteotomy.[18] They concluded that the application of an additional orbital osteotomy provided greater vertical and horizontal angles of attack, wider surgical working area, and increased surgical freedom. Both of these studies contain valuable quantitative and qualitative data for the supraorbital keyhole approach; however, both studies were conducted with the use of microscopes. Therefore, most of their conclusions are valid for microscopic surgery.
Cadaveric studies related to endoscopic supraorbital keyhole craniotomy contain less quantitative data compared with microscopic studies. Komatsu et al. described the endoscopic supraorbital keyhole approach to the cavernous sinus[15] and technique for the extradural anterior clinoidectomy with drilling.[27] Both of these studies are focused on the surgical technique and descriptive anatomy and contain no measurements or quantitative data. Ciporen et al. presented an excellent comprasion of five different endoscopic approaches to the central cranial base, which included the supraorbital keyhole approach[25] and suggested that instead of using one of these approaches alone, a combined multiportal approach would provide more detailed visualization and greater surgical working area. To our knowledge, this the only cadaveric study for the endoscopic supraorbital keyhole approach that gives measurements between target structures such as the pituitary gland, optic chiasm and the dura at the craniotomy site. Another cadaveric study by Filipce et al. compared the working area for supraorbital, pterional and orbitozygomatic approaches.[26] Unlike Figuieredo, they found statistically significant differences regarding the working area provided by these three craniotomies. The orbitozygomatic craniotomy provided the greatest working space and area, followed by pterional and supraorbital craniotomies. But they concluded that the surgical view and working area for supraorbital approach with the use of an endoscope were similar to that of an orbitozygomatic approach and greater than that of a conventional pterional cranitomy.
In most of the anatomic studies in the literature, fresh cadavers with/without color-injected arterial/venous systems were used. The disadvantage of our study is the use of formalin-fixed cadaver heads. Because these specimens have some level of stiffness, cortical atrophy, collapse of the vascular structures and the lack of cisterns filled with CSF, they cannot simulate real surgical experience. Because of the stiffness of the specimen, regular surgical maneuvers like using gravity instead of frontal lobe retraction or drainage of CSF from carotid and chiamatic cisterns for frontal lobe relaxation did not work in our model. In addition to that, retraction of brain tissue resulted in injuries of important neural structures like the olfactory nerve despite meticulous attention being paid to the technique. Another complication related to the supraorbital keyhole approach is anosmia related to olfactory nerve injury. Ipsi- or bilateral olfactory nerve damage rate has been reported to be between 2% and 29%.[4914] However, it is not clear when the olfactory nerve injury has occured in a surgery like this, whether during the retraction or resection stage. As mentioned above, the fragile nature of our formalin-fixed cadavers is the reason for the olfactory nerve damage in all of our cases. The use of fresh cadavers could be made for real-life observations regarding the risk of olfactory nerve injury due to retraction.
Berhouma et al. described the size of the frontal sinus in one individual as the greatest limitation of the supraorbital keyhole approach.[17] They suggested conventional surgery for those individuals with a frontal sinus that reaches the medial half of the orbit. In our study, the frontal sinus was opened in 5 of the 18 craniotomies (28%). This rate seems significantly higher than those of the former clinical studies (1.7–15%).[914] However, it should be remembered that a frontal sinus opening is not equal to CSF leakage if it is properly repaired. Telera et al. reported 15% of frontal sinus opening but no CSF leakage.[14] Reisch and Perneczky reported 2.6% CSF fistulas in their series of 450 patients.[4] Our study was not designed in a way to prevent frontal sinus opening. In most of the studies in the literature, the size and extension of the frontal sinus was evaluated pre-operatively with radiological investigations to modify the craniotomies.
The measurements between target structures like ACommA, ICA bifurcation, basilary tip and the dura at craniotomy site in our study could not be compared with the literature, because to our knowledge, there is no such data for the supraorbital keyhole approach. As mentioned above, only Ciporen et al. provided these measurements for the pituitary gland (76.9 mm) and optic chiasm (70.3 mm).[25] We found the measurement for optic chiasm as 76.2 mm. The distances between deep-seated structures were compared with previously published data. Diaphragma sellae diameter was reported as 10.76 mm previously[28] and it was found 8.4 mm in our study. The distance between the two optic canals was found 13.0 mm in the current study and 14.0 mm in the previously published literature.[29] The diameter of the optic canal was found 7.4 mm in our study and 9.2 mm in the previous data.[30] Although there were some minor differences between our study and the previous data, we think the differences mostly relate to the different measuring techniques or anatomic differences due to racial characteristics.
Our study showed that the ipsilateral arteries of the Circle of Willis could be easily dissected with the endoscopic supraorbital keyhole approach. Ipsilateral ICA, A1 and A2 segments of ACA, M1 segment of MCA, PCommA and ophthalmic artery, also the ACommA could be well visualized and easily manipulated. On the contralateral side, the medial surface of the ICA, M1 segment of MCA, A1 and A2 segments of ACA could be relatively well visualized and manipulated. A clinical study related to aneurysm surgery by Van Lindert et al. indicated similar results to our study for surgical accessibility of vascular structures.[5] In addition to that, they suggested safe contralateral clipping for ICA ophthalmic segment aneurysm unless they are in the medial surface. They also noted that aneurysms within the interpedicular cistern, namely P1 segment of PCA, PCommA, BA tip and the superior cerebellar artery, whether on the ipsi- or contralateral side, could be clipped with the supraorbital keyhole approach.
However, despite the good visualization of these structures with the endoscope, we think that working below the level of basilary tip is challenging. The shaft of the endoscope may cause injuries to vital structures and there could be difficulties providing proximal control, due to the narrow surgical corridor. Therefore, we think only selected and well-documented cases would be appropriate for this surgical approach. Otherwise, almost all vascular structures within the carotid, chiasmatic, suprasellar cisterns and cistern of lamina terminalis could be targets for this approach.
There was good visualization of both orbital rooves, orbital surfaces of the frontal lobes, cribriform plate, sphenoid planum, tuberculum sellae, anterior clinoid process, both optic canals, pituitary gland and infundibulum. Berhouma et al. stated that tumors could be resected using the supraorbital approach if they originated from the anterior and middle cranial base like sphenoid plane, tuberculum sellae and olfactory groove meningiomas, prechiasmatic craniopharyngiomas, pituitary adenomas with suprasellar extension, or were smaller than 4–5 cm in size.[17] Wiedemayer et al. suggested that tumors sized 3 cm should be the limit for resection using the supraorbital keyhole approach.[7] Our study does not provide data regarding the size of the tumors that could be operable via this approach. However, lesions of the central parts of the anterior cranial base would be more appropriate to be resected with this approach.
Conclusions
We believe the current work provides some valuable measurements for anterior cranial base surgery via the endoscopic supraorbital keyhole approach. The surgical working area and dissection were described in detail. The results of this study showed that the anterior and medial aspects of the anterior cranial fossa could be visualized properly. The dissection of the arteries of the Circle of Willis, which are on the same side of the craniotomy, can be performed easily using the endoscopic “supraorbital keyhole” approach. Anterior circulation aneurysms and anterior skull base lesions, especially midline lesions, are easily operable. With the current data and further studies on fresh cadavers, surgical instruments could be modified for the endoscopic supraorbital approach.
Source of Support: Nil.
Conflict of Interest: None declared.
References
- I. An approach to the hypophysis through the anterior cranial fossa. Ann Surg. 1913;57:145-50.
- [Google Scholar]
- Ten-year experience with the supraorbital subfrontal aprroach through an eyebrow skin incision. Neurosurgery. 2005;57(Suppl):242-55.
- [Google Scholar]
- The supraorbital keyhole approach to supratentorial aneuryms: Concept and technique. Surg Neurol. 1998;49:481-90.
- [Google Scholar]
- Application of the supraorbital endoscopic approach to tumors of the anterior cranial base. J Craniofac Surg. 2005;16:1070-5.
- [Google Scholar]
- The supraorbital keyhole approach via an eyebrow incision for resection of tumors around the sella and the anterior skull base. Minim Invasive Neurosurg. 2004;47:221-5.
- [Google Scholar]
- The microsurgical nuances of resecting tuberculum sellae meningiomas. Neurosurgery. 2005;56(Suppl):411-7.
- [Google Scholar]
- Surgical experince with frontolateral keyhole craniotomy through a superciliary skin incision. Neurosurgery. 2001;48:145-50.
- [Google Scholar]
- An anatomical evaluation of the mini-supraorbital approach and comprasion with standard craniotomies. Neurosurgery. 2006;59(Suppl 2):ONS212-20.
- [Google Scholar]
- Fronto-basal interhemispheric approach for tuberculum sella meningiomas; long term visual outcome. Br J Neurosurg. 2009;23:422-30.
- [Google Scholar]
- Tuberculum sellae meningiomas: Microsurgical anatomy and surgical technique. Neurosurgery. 2002;51:1432-40.
- [Google Scholar]
- The keyhole concept in aneurysm surgery--a comparative study: Keyhole versus standart craniotomy. Minim Invas Neurosurg. 2005;48:251-8.
- [Google Scholar]
- Supraorbital keyhole approach for removal of midline anterior cranial fossa meningiomas: A series of 20 consecutive cases. Neurosurg Rev. 2012;35:67-83.
- [Google Scholar]
- Endoscopic supraorbital extradural approach to the cavernous sinus: A cadaver study. J Neurosurg. 2011;114:1331-7.
- [Google Scholar]
- The combined supraorbital keyhole-endoscopic endonasal transsphenoidal approach to sellar, perisellar and frontal skull base tumors: Surgical technique. Minim Invasive Neurosurg. 2009;52:281-6.
- [Google Scholar]
- The fully endoscopic supraorbital trans-eyebrow keyhole approach to the anterior and middle skull base. Acta Neurochir (Wien). 2011;153:1949-54.
- [Google Scholar]
- Quantitative anatomic study of the transciliary supraorbital approach: Benefits of additional orbital osteotomy? Neurosurgery. 2010;66(Suppl Operative):205-10.
- [Google Scholar]
- Endoscope-assisted brain surgery: Part 2--analysis of 380 procedures. Neurosurgery. 1998;42:226-32.
- [Google Scholar]
- The endoscopic supraorbital approach to tumors of the middle cranial base. Surg Neurol. 2006;66:396-401.
- [Google Scholar]
- Fully endoscopic supraorbital resection of congenital middle cranial fossa arachnoid cysts: Report of 2 cases. Pediatr Neurosurg. 2007;43:316-22.
- [Google Scholar]
- Endoscope-assisted supraorbital craniotomy for lesions of the interpeduncular fossa. Neurosurgery. 1999;44:106-12.
- [Google Scholar]
- Surgical management of tuberculum sellae meningioma: Role of selective extradural anterior clinoidectomy. Br J Neurosurg. 2006;20:129-38.
- [Google Scholar]
- Endoscopy-assisted brain surgery: Part 1--evolution, basic concept, and current technique. Neurosurgery. 1998;42:219-25.
- [Google Scholar]
- Multiportal endoscopic approaches to the central skull base: A cadaveric study. World Neurosurg. 2010;73:705-12.
- [Google Scholar]
- Quantitative and qualitative analysis of the working area obtained by endoscope and microscope in various approaches to the anterior communicating artery complex using computed tomography based frameless stereotaxy: A cadaver study. Neurosurgery. 2009;65:1147-53.
- [Google Scholar]
- Endoscopic extradural anterior clinoidectomy via supraorbital keyhole: A cadaveric study. Neurosurgery. 2011;68(Suppl Operative):334-8.
- [Google Scholar]
- Hypophyseal region. In: Lang J, ed. Skull Base and Related Structures: Atlas of Clinical Anatomy. Stuggart, Germany: Schattauer Verlag; 1995. p. :172-6.
- [Google Scholar]
- Incisura tentorii and mesencephalon. In: Lang J, ed. Skull Base and Related Structures: Atlas of Clinical Anatomy. Stuggart, Germany: Schattauer Verlag; 1995. p. :235-8.
- [Google Scholar]
- Cavernous sinus. In: Lang J, ed. Skull Base and Related Structures: Atlas of Clinical Anatomy. Stuggart, Germany: Schattauer Verlag; 1995. p. :177-98.
- [Google Scholar]




