
Translate this page into:
Double C1 Posterior Arches
Address for correspondence: Dr. Pralaya Kishore Nayak, Department of Neurosurgery, Sparsh Hospital, Saheed Nagar, Bhubaneswar - 751 007, Odisha, India. E-mail: drmichaelpn@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Congenital anomalies of the posterior arch of the atlas (C1) are relatively common anomalies. They may range from partial defects presenting as clefts to complete absence of the posterior arch. However, presenting as double posterior C1 arch is extremely rare.
A 22-year-old male presented to us with head injury. Routine X-ray screening of the cervical spine revealed two posterior arches of the atlas [Figure 1]. However, the patient was asymptomatic apart from mild neck pain. Computed tomography (CT) scan of the cervical spine showed, both anterior and posterior splitting of the arch of atlas along with fusion of the dens to right side of the anterior arch [Figure 2]. Then with three-dimensional reconstruction in the CT scan, the posterior splitting of arches was at different level in the axial plane, which was seen as a double posterior component in lateral X-ray film. Furthermore, it was noted that the bodies of C1 and C2 were fused on the right side [Figures 3 and 4]. No further investigation like magnetic resonance imaging of cervical spine was ordered, as there was no neurological deficit. He was advised to wear a cervical collar and to have regular follow-up.
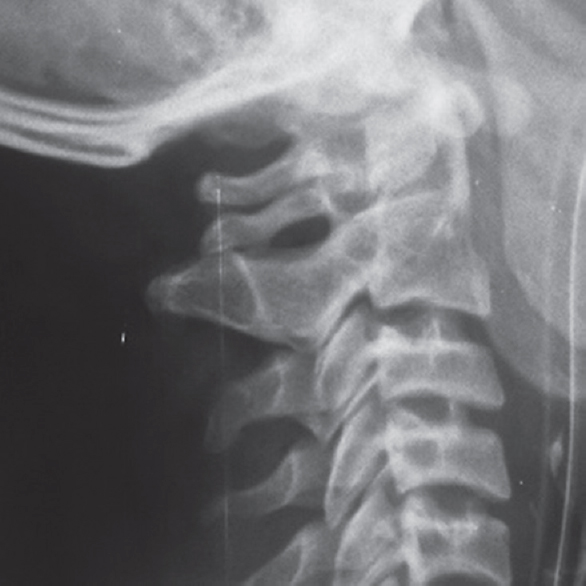
- X-ray cervical spine showing two C1 posterior arches
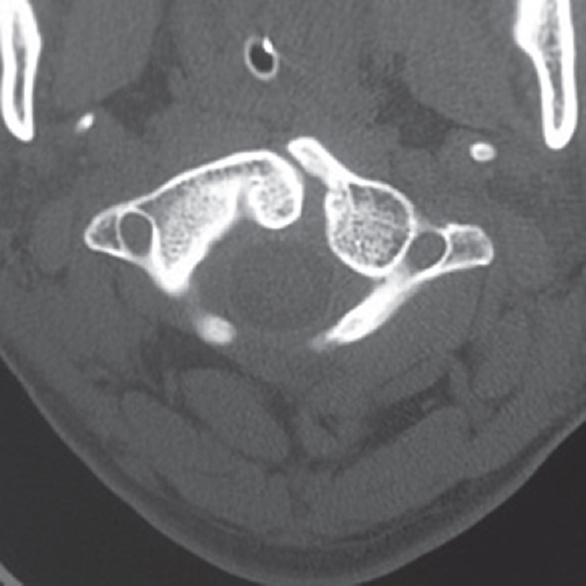
- Spinal computed tomography showing congenital anomaly of C1

- Three-dimensional computed tomography reconstruction of C1/C2 complex

- Dens fused to right half of C1 arch
The reported incidence in a large study of 1613 autopsies with regard to the presence of congenital aplasia in the C1 vertebra is approximately 4% for the posterior arch and 0.1% for the anterior arch.[1] However, the incidence would be higher as many cases do not go routine screening. The congenital defects of the posterior arch of the atlas may be discovered as incidental asymptomatic findings, but symptoms occurring after trauma to the head and neck or spontaneously also may be encountered.[2]
Three primary ossification centers have been described in the C1 vertebra: Anterior center, which forms the anterior tubercle; and two lateral centers, which form the lateral masses and the posterior arch. Defects of the posterior arch are thought to develop because of a failure of local chondrogenesis rather than subsequent ossification.[3] The possibility of wide splitting of posterior arch and level of difference in axial plane in our case may be due to defective chondrogenesis.
In case of trivial neck trauma, one should investigate further to look for any fracture or and associated other congenital anomalies. It is important to be familiar with the differences between a congenital anomaly of the atlas and a Jefferson fracture and to exclude instability of the upper cervical spine before treatment is started.[4] The developmental cleft margins are smooth with an intact cortical edge and no soft-tissue swelling. Conversely, fractures have jagged edges or are comminuted and generally are associated with soft-tissue swelling.[5] No definitive guidelines exist for the management of this type of congenital anomaly. This is purely an incidental finding in an asymptomatic patient, and he only needs regular follow-up. In conclusion, C1 anomalies can present in various ways, and their management differs accordingly depending on the instability they produce. High degree of suspicion is required to diagnose such anomalies and appropriate treatment can be instituted whenever required.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Congenital posterior atlas defect associated with anterior rachischisis and early cervical degenerative disc disease: A case study and review of the literature. Acta Orthop Belg. 2007;73:282-5.
- [Google Scholar]
- Congenital defects of the posterior arch of the atlas: A report of seven cases including an affected mother and son. AJNR Am J Neuroradiol. 1994;15:249-54.
- [Google Scholar]
- Congenital C1 arch deficiency: Grand Round presentation. Eur Spine J. 2013;22:1223-6.
- [Google Scholar]
- A congenital anomaly of the atlas as a diagnostic dilemma: A case report. J Manipulative Physiol Ther. 2007;30:62-4.
- [Google Scholar]
- CT recognition of anomalies of the posterior arch of the atlas vertebra: Differentiation from fracture. AJNR Am J Neuroradiol. 1986;7:176-7.
- [Google Scholar]




