
Translate this page into:
Craniomapper for accurate localization of lesion during craniotomy: How much benefit does it have over anatomical marking? Report of two cases
Address for correspondence: Dr. Pralaya Kishore Nayak, Department of Neurosurgery, NeotiaGetwel Healthcare Centre, Siliguri - 734 010, West Bengal, India. E-mail: drmichaelpn@rediffmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Localizing smaller lesions in the brain while marking for craniotomy is, sometimes, a difficult and cumbersome task. At times we miss the margin by a few millimeters, which lead to the use of brain retraction and/or bone resection. This is particularly true in high convexity areas where the landmarks are obscured and reference bony points are far. Further, the use of a stereotactic frame or Neuronavigation is not available widely in India. This is particularly applied where precise craniotomy is required, may it be routine or emergency surgery where wide craniotomy is not desired. The author used a special frame designed to surface mark the lesion during computed tomography (CT) scanning of the brain, particularly in lesions located near the eloquent area. The more precise localization provided thereby facilitated planning and performance of surgery.[1]
Craniomapper (Surgiwear, India) is an external plastic frame embedded with radio opaque markers placed around the patient head during CT scanning. The vertical and horizontal lines of the frame serve as a guide to a particular site. A CT topogram is superimposed over the frame. The radioopaque markers are visible on an axial plane, from the anterior to the posterior direction. Any particular axial section of interest is marked by laser light inside the gantry, and the distance from the midline is counted following the markers. Then, the most target part is outlined by a permanent marker pen [Figure 1]. It accurately provides a 2D plane, whereas a 3D plane cannot be exactly defined as in the image guidance system.
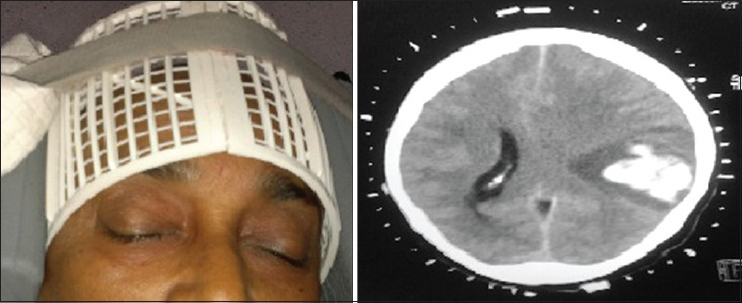
- Craniomapper with axial marker computed tomography
The author tried the use of Craniomapper in two patients with high parietal convexity spontaneous bleed. The patients were properly investigated prior to emergency surgery. Both were conscious with neurologically mild motor deficit. CT brain showed localized superficial bleed with less brain edema. To locate the bleed precisely and to avoid brain retraction, we decided to use the external frame as wide craniotomy was not indicated in these patients.
The difficulty of localization of the small intracranial lesion on CT has been widely recognized by neurosurgeons. Experience may minimize the error, but the precise localization of high-convexity lesion still poses a considerable challenge.[2] CT, with its inherent accuracy in identifying and localizing intracranial lesions, has been adapted by several groups for use in stereotactic neurosurgical procedures.[3] Frame-based stereotactic systems provide valuable localization information for the performance of neurosurgical procedures.[4]
Marking of the skull prior to craniotomy on the basis of CT images can prove to be a difficult problem.[5] Conventional methods of preoperative localization include measurement and calculation from the baseline, such as orbito–meatal line, or obtaining a CT scan with a marker on the scalp.[6] However, easy and less-technical localization is mandatory in emergency surgery and small lesion in routine surgery, where such facilities are not available. A similar rapid, simple and inexpensive CT technique has been developed for marking the scalp and lateral skull radiograph of patients with small cerebral convexity lesions.[1] It is safe to use the frame and needs no special training. It is also not costly and can address the issue, where image guidance/stereotactic systems are not available. We need to try it with other small lesions like brain tumor and in a number of cases prior to judging its efficacy. It is helpful in localization of brain lesions in developing countries without high technical facilities.
References
- Scalp markers for precise craniotomy siting, using computed tomography. J Comput Assist Tomogr. 1979;3:701-2.
- [Google Scholar]
- Intracranial lesion localisation: A simple method using CT scanning. J Neurol Neurosurg Psychiatry. 1982;45:752-3.
- [Google Scholar]
- An overview of CT based stereotactic systems for the localization of intracranial lesions. Comput Radiol. 1984;8:193-6.
- [Google Scholar]
- Computer-assisted preoperative planning, interactive surgery, and frameless stereotaxy. Clin Neurosurg. 1992;38:112-31.
- [Google Scholar]
- Computed tomography-guided scalp marking of cerebral surface lesions; an alternative to stereotaxis for small convexity lesions. Eur J Radiol. 1990;11:143-4.
- [Google Scholar]
- Craniotomy for lesions in the cerebral convexity; how to precisely localize the lesions with conventional CT slices. No Shinkei Geka. Neurological surgery. 1992;20:875-81.
- [Google Scholar]




