
Translate this page into:
Community Screening of Probable Dementia at Primary Care Center in Western India: A Pilot Project
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Introduction Timely detecting dementia is an important goal of clinicians and public health professionals alike for better management and prevention of complications. Community screening of dementia could be a powerful strategy. Facilities for dementia screening at primary care level are virtually nonexistent and are a prominent implementation gap. Hence, a study was done to assess the feasibility of dementia screening at primary care using General Practitioner Assessment of Cognition (GPCoG) scale among older adults with subjective memory complaints. It was further aimed to assess the frequency of cardiovascular risk factors in those who met screening criteria for cognitive impairment.
Materials and Methods Older adults coming to three urban primary care centers in western India for screening of noncommunicable diseases such as diabetes and hypertension (opportunistic screening) with subjective memory complaints were enrolled and screened for dementia using GPCoG. A Mini-Mental State Examination (MMSE) was done in patients who came alone for referral purpose in case the score levels in GPCoG examination met cutoff limits for informant interview. Written medical records were examined to assess status of comorbid vascular risk factors such as diabetes, hypertension, coronary artery disease, and cerebrovascular accidents.
Results A total of 350 older adults (M:F = 276: 74; mean age ± 68 ± 6.7 years) were screened out of 3,000 older adults who reported during the study period. There were 161 older adults with GPCoG score less than or equal to 5 (56.14%) and 149 subjects with MMSE less than or equal to 24 indicating significant cognitive impairment (42.5%). There were very few (n = 11, 3.14%) out of 350 people who came with caregivers; hence, MMSE was done along with for referral to healthcare providers. A total of 142 had comorbid diabetes/and or hypertension (40.5%). A total of 86 had diabetes alone (24.5%) and a total of 128 had hypertension (36.5%).
Conclusion Current study results indicate that using a simple screening tool such as GPCoG, community screening of probable dementia, is feasible in primary care settings, as is indicated by significant yield of probable dementia cases (42.5%). These cases can be referred to appropriate centers for further workup, confirmation of diagnosis, and treatment. Also, detection of comorbid cardiovascular conditions, for example, diabetes and hypertension, that can be managed along with cognitive impairment/dementia for potential prevention/further deterioration, which can strengthen noncommunicable disease screening.
Keywords
dementia
community screening
risk
cardiovascular risk factors

Introduction
Community screening of probable dementia has been suggested to be an important strategy to detect patients in their early stages, so that their treatment and later rehabilitation could be planned better.1 Also, screening patients in their early stages also leaves a window for secondary prevention of dementias at later stage as well. Since families in India take up responsibilities of treatment of patients with dementia, it is important to screen them on time.1 2 3 Major implementation gap is that the clinical options for early diagnosis are limited especially in primary care. Adding to the problem is the additional issue that patients hardly go for routine checkup related to early symptoms of dementias. Hence, early screening could be useful option for picking up in their early stages when patients come for screening of non-communicable diseases.2
Among all the ailments among older adults, cognitive impairment/dementia has an adverse effect on quality of life and imposes high caregiver burden. It is now increasingly been noted that noncommunicable diseases like diabetes, hypertension, or both occurring either individually or as comorbid illnesses may increase the risk of dementia.4
It is well known that even after decades of National Mental Health Program, implementation of the same is problematic and facilities for dementia screening at primary care level are deficient in India. Main problems are lack of trained manpower, poor understanding of dementias, and impression of dementias a topic that is dealt at a super-specialty level. It has been seen that prevalence of undetected dementia in community is high5 6 7 even at global levels, especially in India and China, as shown by a meta-analysis of 23 studies.
Hence, a study was done to assess the feasibility of dementia screening at primary care using General Practitioner Assessment of Cognition (GPCoG). A Mini-Mental State Examination (MMSE) was done in patients who came alone and did not have an informant for referral purpose in case the score levels met cutoff limits. It was further aimed to assess the frequency of cardiovascular risk factors if those who met screening criteria for cognitive impairment using GPCoG.
Materials and Methods
Study Setting
Study was done in three urban primary healthcare centers (PHCs) in Jodhpur district of western Rajasthan. Patients who came to PHCs for screening and management of non-communicable diseases, for example, diabetes and/or hypertension or both, were assessed by medical/paramedical staff for subjective memory complaints (SMCs). They were instructed to undergo “dementia screening” if they accepted having SMCs for the last 1 month.
Design of Study
It was a cross-sectional study done among people over the age of 60 or more who attended primary care centers for screening of noncommunicable diseases as a part of National Program for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke program or visited PHCs for some other indications.
Inclusion and Exclusion Criteria
Study enrolled people aged 60 or more who attended primary care centers for screening of noncommunicable diseases and had SMCs.
Scales Used in the Current Study
Mini Mental State Examination
MMSE8 is the usual clinical scale to assess mental state of an individual. This has 30 questions, each with the domains that can assess various abilities such as listening, speaking, drawing, and writing and can give scores. A score of 24 or more rules out diagnosis of dementia but patients may have mild cognitive impairment (MCI) that can progress to development of dementia later. As per studies done elsewhere, it has been shown that approximately 13% of the people get converted into dementia on yearly basis.
General Practitioner Assessment of Cognition
GPCoG scale has six questions, and nine marks for the assessment and is administered both to patients and informants depending upon the scores. Dementia can be suspected when the score is below 8 and detailed evaluation by informant is needed. GPCoG has been designed as a tool that can be used by general practitioners for screening of dementia, especially in primary care. There are two components of GPCoG: a cognitive assessment conducted with the patient and an informant questionnaire (done only if score is between 5 and 8 or is inclusive). For patients, result more than 8 is interpreted as normal or in fact cognition and score below 5 is considered to be impaired cognition. A score of 3 or less out of 6 indicates the need for informant interview, that is, significant cognitive impairment indicating the probability of early dementia.
Subject Selection
Those older adults coming to primary care getting their blood pressure/sugar checked or seeking treatment for either or both of the diseases (e.g., diabetes and/or hypertension) were asked by healthcare workers (e.g., staff nurses) to undergo detailed memory evaluation.
Ethics
The study was done in accordance with the Indian Council of Medical Research (ICMR) Guidelines for Biomedical and Health Research (2017). Written and informed consent was taken from all the study participants and those unwilling to undergo the dementia screening were excluded. The study protocol was approved by institute ethics committee, Indian Council of Medical Research-National Institute for Implementation Research on Non Communicable Diseases (ICMR-NIIRNCD), Jodhpur (Rajasthan).
Results
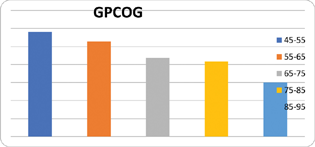
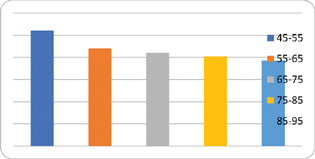
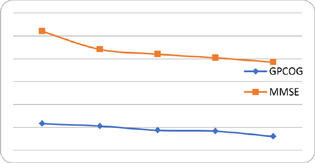
A total of 350 older adults (M:F = 276: 74; mean age ± 68 ± 6.7 years) coming to three urban primary care centers in western India were screened out of 3,000 older adults who visited during study period (February–August 2021). There were 161 older adults with GPCoG score less than or equal to 5 (56.14%) (Fig. 1) and 149 subjects with MMSE less than or equal to 24 (Fig. 2) indicating significant cognitive impairment (42.5%). There were very few (n = 11) out of 350 people who came with caregivers; hence, MMSE was done along with for referral via healthcare providers. A total of 142 had comorbid diabetes and/or hypertension (40.5%). A total of 86 had diabetes alone (24.5%) and a total of 128 had hypertension (36.5%). There was a good agreement between the values of GPCoG and MMSE (Fig. 3).
-
Fig. 1 General Practitioner Assessment of Cognition (GPCoG) scores of the study participants in the current study.
Fig. 1 General Practitioner Assessment of Cognition (GPCoG) scores of the study participants in the current study.
-
Fig. 2 Mini-Mental State Examination (MMSE) scores of the participants in the current study.
Fig. 2 Mini-Mental State Examination (MMSE) scores of the participants in the current study.
-
Fig. 3 Comparative trajectories of General Practitioner Assessment of Cognition (GPCoG) and Mini-Mental State Examination (MMSE) in the current study.
Fig. 3 Comparative trajectories of General Practitioner Assessment of Cognition (GPCoG) and Mini-Mental State Examination (MMSE) in the current study.
There was a high positive correlation between GPCoG and MMSE scores indicating good deal of agreement between the two (Pearson correlation coefficient = 0.62; p-value ≤ 0.05). There were a total of 151 subjects with GPCoG score less than or equal to 4 indicative of cognitive impairment. There was a complete agreement among raters (Dr BJ & PG) for screening cognitive impairment using GPCoG and MMSE (Cohen Kappa = 1).
Discussion
Dementia is common disease of the older adults and is most common and most dreaded neurodegenerative illness. Though dementia is not a life-threatening disease, it is expensive to treat with significant cost and disease burden to the caregivers. Therefore, it goes without saying that dementia is one of most stigmatized illnesses as well.
Screening for MCI and/or early dementia is a dream of public health professionals and clinicians alike. However, there are no uniformly agreed methods for screening the patients. Screening the older adults as a whole may not feasible on the one hand, while missing out cases could have its own consequence as well. Hence, the ideal situation would be perhaps door-to-door screening but that may not be practical. Adding to the difficulties that in the existing public healthcare system, there are no screening programs ongoing for dementia at all.
MMSE9 could be a screening tool but then it needs trained manpower, and is relatively more time consuming compared with a simple screening tool like GPCoG. Hence, it is important to detect dementia early as worldwide data shows that the prevalence of undetected dementia is high globally.5 To be able to cover this gap, nonspecialists are being proposed to be trained using newly developed instruments applicable in community.10 11 12
Since dementia is incurable at present, therefore, primary and secondary prevention of dementia by treating risk factors and promotion of protective lifestyle factors appears to be a feasible option. It goes without saying that for effective handling of dementia crises, we need to empower the primary healthcare workers (e.g., doctors and nurses) in screening and management of dementia.6 7 Therefore, the implementation research in dementia should be considered as priority.13 14 15 16 17 This may not only increase yield of undetected dementia but may also help address the vascular risk factors, addressing which may potentially prevent cognitive decline. Though screening of healthy older adults may be evolving, there is no doubt that those with SMCs need to be screened.18
This study highlights a significant burden of cognitive impairment as is shown by high proportion of cognitive impairment among those who came for screening/treatment of diabetes, hypertension, etc. in primary care. Also, the study suggests a significant burden of undiagnosed cases of cognitive impairment with comorbidities, for example, hypertension, diabetes, depression, and coronary artery disease all of which are important risk factors for dementia. There is a need to identify large number of undiagnosed cases in the community along with morbidities, for example, diabetes/hypertension by screening, and offer early management to avoid development of complications.4 Poor awareness about is a key implementation barrier in patients of dementia/cognitive impairment preventing them reaching to the primary care. There could be societal assumptions about aging in general in Indian society preventing seeking of consultation among demented patients. For example, there could be withdrawal of the elderly from the previous societal roles and withdrawal from all types of interactions after retirement adding to stress of aging.5 6 7
One of the most important questions in preventive geriatrics is: what is the importance of diagnosing dementia early? Early diagnosis of cognitive decline has many advantages, for example, addressing modifiable risk factors and hence halting the disease process, preparing the family to address the consequences. Early intervention also enhances the quality of life of the demented patient and caregiver and is known to cause less severe behavioral and psychological symptoms of dementia.
The major challenge in secondary prevention is the diagnosis of preclinical stage as it is difficult to diagnose in the absence of brain abnormalities and clinical symptoms. The continuum of preclinical stage, MCI, and Alzheimer's dementia is not established clearly in all cases, more so not all MCIs progress to Alzheimer's dementia and overt disease can occur even in the absence of MCI. Community screening of dementia is a powerful tool to detect patients early and test interventions that can be useful for prevention. Facilities for dementia screening at primary care level are deficient. Hence, a study was done to see the feasibility of dementia screening at primary care using simple screening tools, for example, GPCoG and MMSE. It was further aimed to assess the frequency of cardiovascular risk factors of those who met screening criteria for cognitive impairment using GPCoG.
Programs to raise awareness to reduce stigma and wide screening using a reliable tool need to be considered for dementia screening. Controlling vascular risk factors could prevent or delay progression of dementia.9 Addressing comorbid psychiatric illness, for example, depression in cognitive impairment/dementia, improves functional well-being.5
To screen the patients with cognitive impairment, MMSE8 9 has been suggested. However, there are several drawbacks of MMSE, for example, time consuming, needs training, required healthcare-dedicated professionals, and cannot be administered by community health workers/volunteers. GPCoG, on the other hand, is free from these drawbacks, hence was used primarily in the current study. Screening of patients reporting to primary care for dementias is not only desirable but an early diagnosis16 and referral can reduce the disease burden.
A recent systematic review and meta-analysis showed the pooled rate of undetected dementia as 62% globally,5 calling for application of tools that can be used to increase detection rates. Not just cognitive related issues, but lower cognition scores have been associated with functional impairment and disability. Acceptability of dementia screening among older adults in community is good19 20 if implemented well.
Current study involves an innovative model of dementia screening in primary care using the existing healthcare facilities as per National Health Policy Guidelines (2014) which states that “mental health should be integrated with primary care services,” especially in rural areas. Study reports feasibility and acceptability of dementia screening among primary care attendees using GPCoG.
Conflict of Interest
None declared.
References
- An epidemiological study of dementia in a rural community in Kerala, India. Br J Psychiatry. 1996;168(6):745-749.
- [Google Scholar]
- Lifestyle modifications and nutritional interventions in aging-associated cognitive decline and Alzheimer's disease. Front Aging Neurosci. 2020;11:369.
- [Google Scholar]
- Prevalence of cognitive dysfunction, psychological morbidity and abuse in the community-based elderly population in India. Gen Psychiatr. 2020;33(5):e100207.
- [Google Scholar]
- Cardiovascular risk factors among older adults with cognitive impairment in primary care. Int Psychogeriatr. 2021;33(8):837-838.
- [Google Scholar]
- Prevalence and determinants of undetected dementia in the community: a systematic literature review and a meta-analysis. BMJ Open. 2017;7(2):e011146.
- [Google Scholar]
- Are vascular factors linked to the development of hippocampal atrophy in Alzheimer's disease? J Alzheimers Dis. 2012;32(3):711-718.
- [Google Scholar]
- Potential predictors of hippocampal atrophy in Alzheimer's disease. Drugs Aging. 2011;28(1):1-11.
- [Google Scholar]
- Is hypertension a predictor of hippocampal atrophy in Alzheimer's disease? Int Psychogeriatr. 2009;21(4):795-796.
- [Google Scholar]
- Screening for dementia: fluidity and the Mini Mental State Examination in India. Transcult Psychiatry. 2011;48(5):604-623.
- [Google Scholar]
- 10/66 Dementia Group. A brief dementia screener suitable for use by non-specialists in resource poor settings–the cross-cultural derivation and validation of the brief Community Screening Instrument for Dementia. Int J Geriatr Psychiatry. 2011;26(9):899-907.
- [Google Scholar]
- The PHC-cog: a brief cognitive function screening test for the elderly. Neurol India. 2005;53(1):60-64. , discussion 65
- [Google Scholar]
- Diagnostic accuracy of 10/66 dementia protocol in Fijian-Indian elders living in New Zealand. Int J Environ Res Public Health. 2021;18:4870.
- [Google Scholar]
- Closing the treatment gap for dementia in India. Indian J Psychiatry. 2009;51(01):S93-S97.
- [Google Scholar]
- Status of cognitive testing of adults in India. Ann Indian Acad Neurol. 2017;20(4):334-340.
- [Google Scholar]
- Associations between midlife vascular risk factors and 25-year incident dementia in the Atherosclerosis Risk in Communities (ARIC) Cohort. JAMA Neurol.. 2017;74(10):1246-1254.
- [Google Scholar]
- Ageing and mental health in a developing country: who cares? Qualitative studies from Goa, India. Psychol Med. 2001;31(1):29-38.
- [Google Scholar]
- Prevalence study of cognitive impairment and its associated sociodemographic variables using Mini-Mental Status Examination among elderly population residing in field practice areas of a medical college. Indian J Community Med. 2018;43(2):113-116.
- [Google Scholar]
- Screening for Cognitive Impairment in Older Adults: An Evidence Update for the U.S. Preventive Services Task Force [Internet] Rockville (MD): Agency for Healthcare Research and Quality (US); 2020 Feb. Report No.: 19–05257-EF-1. PMID: 32129963
- [Google Scholar]
- Cardiovascular risk factors among older adults with cognitive impairment in primary care. Int Psychogeriatr. 2021;33(8):837-838.
- [Google Scholar]
- Intention to undergo dementia screening in primary care settings among community-dwelling older people. Int J Geriatr Psychiatry. 2020;35(9):1036-1042.
- [Google Scholar]




