
Translate this page into:
Cognitive Impairment in Rural Elderly Population in Ecuador
Address for correspondence: Dr. Xavier Wong-Achi, MSP, Ingapirca's healthcare center, Ingapirca, Cañar, Ecuador E-mail: xavierwongachi@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
The Mini-Cog is a simple and short test that identifies cognitive impairment. Its detection helps provide an early dementia diagnosis, rapid access to treatments, and even delay or reversion.
Materials and Methods:
This multicenter, observational, descriptive, and cross-sectional study included 214 patients. Patients enrolled in this study were community dwellers aged ≥55-year-old, without prior diagnosis of cognitive impairment or dementia, with adequate hearing and vision functions. It was conducted in primary care health centers localized in rural communities of Ecuador.
Results:
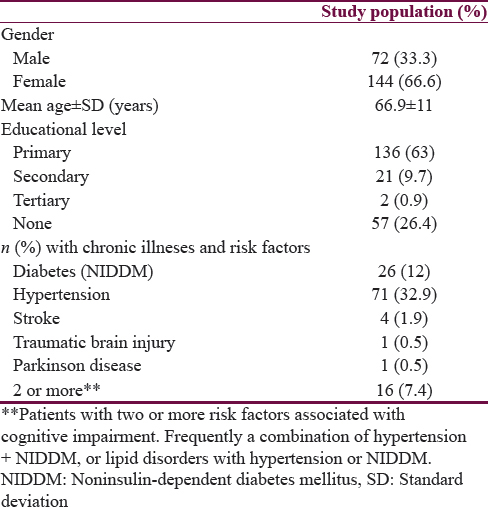
Ages ranged from 50 to 98 years and there was predominance of female gender: 66% versus 33%. The percentage of illiteracy was 26.4% (CI: 25.32–27.48), and 63% (CI: 62.1–63.94) of patients had complete primary educational level. The overall prevalence of cognitive impairment was 50.9% (95% CI: 48.5–53.3) and 47.2% (95% CI: 45.2–49.2) in patients with risk factors. We found several established risk factors associated with cognitive impairment onset, including social factors, physiological factors, and comorbidities.
Conclusion:
This is the first epidemiological research of CI in rural populations in this country using the Mini-Cog as a screening tool. Adopting public health measures for the prevention and control of those modifiable risk factors could reduce the prevalence of cognitive impairment and even its progression to dementia.
Keywords
Dementia
Ecuador
primary health care

INTRODUCTION
One of the clinical conditions that precede dementia is the cognitive impairment (CI).[1] In fact, it is considered that one-third of patients with CI develop dementia.[2] Thus, an early detection of CI could produce several benefits including early dementia diagnosis, access to treatments, and delay or even reversion of CI. Nowadays, the application of a simple and short test helps optimize the detection of CI in primary care. The Mini-Cog test meets the criteria above; however, some studies have shown influence of level of education in its performance.[3] The present study was designed to show the usefulness of the test in primary care in rural areas.
MATERIALS AND METHODS
Study design and participants
This was a 5-month, multicenter, observational, descriptive, and cross-sectional study conducted in three rural communities of the coast and highlands of Ecuador. The setting of the study was primary care health centers. Patients enrolled in this study were community dwellers aged ≥55-year-old, any gender, without prior diagnosis of cognitive impairment or dementia, with adequate hearing and vision and able to communicate in Spanish. Verbal consent was obtained from each participant before their inclusion. Other patient information collected at baseline included sociodemographics (level of education) and comorbidities related with cognitive impairment development (hypertension, diabetes mellitus, stroke, traumatic brain injury). This information was collected by the authors and registered in an Excel 2010 data sheet.
Cognitive function assessment
The Mini-Cog test is a 3-min instrument to screen cognitive impairment in older adults in primary care setting. This test uses a 3-item recall for memory and a simple scored clock-drawing test. In comparative tests, the Mini-Cog was at least twice as fast as the Mini–Mental State Examination. According to many studies, the Mini-Cog is less affected by subject ethnicity, language, and education. Furthermore, this test detects many people with mild cognitive impairment.[4] A standard algorithm is used to score the Mini-Cog (number of word recalled plus two points for the clock drawing) with a score <3 defining cognitive impairment.
Analysis
A descriptive analysis was performed using frequencies and percentages or medians with standard deviation as appropriate. Fisher's exact test was considered for categorical variables. The primary outcome was to show the influence of educational level in the test application and as a factor for CI development. Secondary outcome includes associated factors, its prevalence, and relation with positive screenings. Odds ratios and 95% confidence intervals (CIs) were calculated for significant associations. A P < 0.05 was considered statistically significant. The tabulation of the data, its analysis, and the elaboration of tables and graphs was done with assistance of Microsoft Excel 2010 and 2015 Rcmdr: R Commander. R package version 3.2.3
RESULTS
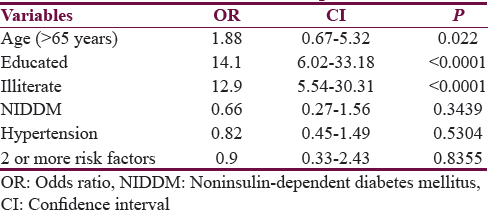
From this sample, 214 patients were suitable for analysis. Two patients were excluded because of a diagnosis of Alzheimer's disease and visual deficit. No patient took longer than 5 min to complete the test. Ages ranged from 50 to 98 years and there was predominance of female gender: 142 (66%) versus 72 (33%). The percentage of illiteracy was 26.4% (CI: 25.32–27.48), and 63% (CI: 62.1–63.94) of patients had complete primary educational level. Other participant's data are showed in Table 1. Patients with a positive screening were older than those with a negative test (mean age 70 ± 10.6 years vs. 63 ± 10.5 years) and also had a lesser educational level. The overall prevalence of cognitive impairment in these rural areas was 50.9% (95% CI: 48.5–53.3) and 47.2% (95% CI: 45.2–49.2) in patients with risk factors. Analysis showed that illiterates without risk factors had higher prevalence of positive screening compared with those patients with at least elementary educational level: 35 (16.4%) versus 25 (11.7%). Figure 1 shows the distribution of screening results by educational level in the studied population. Furthermore, we found several established risk factors associated with cognitive impairment onset, including social factors (education), physiological factors (age), and comorbidities, mentioned in Table 1. However, there was no significance in some factors’ analysis perhaps due to the low number of cases in comparison to healthy patients. Negative-associated factors included aging (odds = 1.88, P = 0.022), illiterate (odds = 12.9, P ≤ 0.0001), NIDDM (odds = 0.66, P = 0.344), hypertension (odds = 0.82, P = 0.530), and two or more risk factors (odds = 0.9, P = 0.836). A positive-associated factor identified was higher education or at least lower educational level (odds = 14.1, P ≤ 0.0001). Table 2 and Figure 2 summarize the findings in the analysis of associated factors.
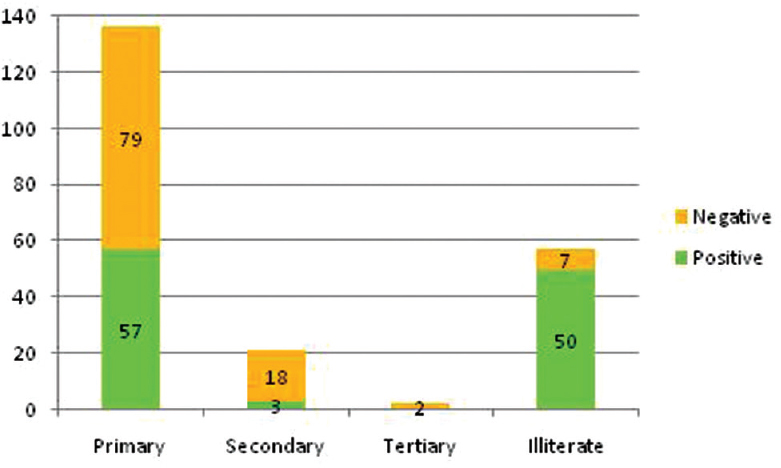
- Distribution of screening results by educational level
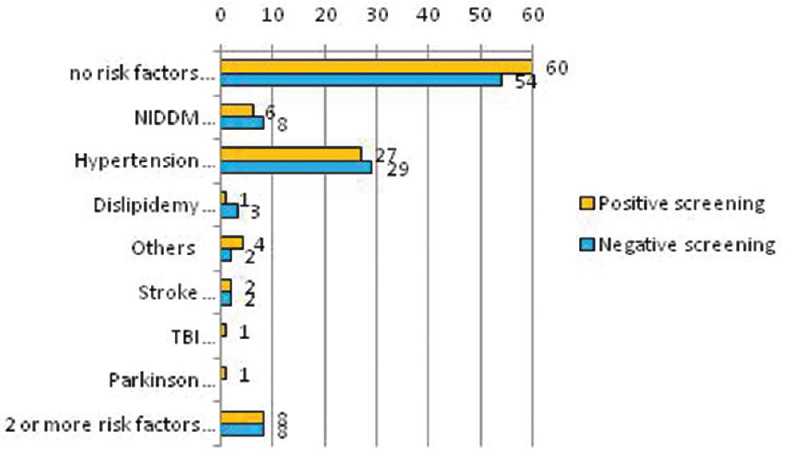
- Distribution of screening results by associated risk factors
CONCLUSION
In Ecuador, statistics on cognitive impairment and risk factors had been reported in urban areas;[567] however, this study is the first epidemiological research of CI in rural populations in this country using the Mini-Cog as a screening tool. From the present study, it was demonstrated that the Mini-Cog test is an easy-to-use tool in primary care centers; furthermore, it has a high acceptability by the patients. The results showed that the 50.9% of individuals enrolled in this study had a positive screen for CI. The prevalence was higher with age >65 years and low levels of education. Significant risk factors as hypertension, diabetes mellitus, and illiteracy – being the most prevalent – were found. On the other hand, protective factors identified had at least low educational level. This correlates with the data reported in other studies.[8910] The prevalence of CI increases exponentially with age and in those with comorbid conditions; but in accordance with previous studies, cognitive impairment is also higher in people with low levels of education or illiterate, and in addition, higher levels of education independently reduced the risk.[11] We can conclude that Mini-Cog is a simple screening tool that is well accepted and quickly to apply during the routine visit, with a sensitivity and specificity that reaches up to 99% and 93%, respectively,[121314] especially when the health practicers are trained to apply the test correctly. In terms of associated risk factors, advanced age, low educational level, and comorbidities such as hypertension and diabetes mellitus were the main factors associated with CI, which suggests that adopting public health measures for the prevention and control of those modifiable risk factors can reduce the prevalence of this condition and even its progression to dementia. We recommend to carry out studies with greater population of rural areas. Likewise, this information can be used as an object of the future research that support its widespread use in primary care centers, allowing prevention, early diagnosis and treatment, and even reversion of cognitive impairment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 2016. Dementia. WHO Library Cataloguing-in-Publication Data. Available from: https://www.goo.gl/GxsTI0
- 2016. Alzheimerxs Disease International. World Alzheimer Report: Improving Healthcare for People Living with Dementia. Alzheimerxs Disease International (ADI). Available from: https://www.goo.gl/Ldv1Wr
- Utility of the Mini-Cog for detection of cognitive impairment in primary care: Data from two spanish studies. Int J Alzheimers Dis. 2013;2013:285462.
- [Google Scholar]
- The Mini-Cog: A cognitive ’vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry. 2000;15:1021-7.
- [Google Scholar]
- Cognitive impairment and risk of dementia, a reality for Ecuador. Study of risk factors in a group of retired IESS patients in 2013. Rev Ecuat Neurol. 2014;23:12-17.
- [Google Scholar]
- Risk factors and prevalence of dementia and Alzheimer's disease in Pichincha-Ecuador (FARYPDEA study) Rev Fac Cien Med. 2012;37:49-54.
- [Google Scholar]
- Concept of dementia as a disease in a population group of Guayaquil. Rev Ecuat Neurol. 2014;23:29-33.
- [Google Scholar]
- Prevalence of cognitive impairment no dementia in a rural area of Northern China. Neuroepidemiology. 2014;42:197-203.
- [Google Scholar]
- Incidence and risk factors for cognitive impairment in rural elderly populations in Costa Rica. Rev Biol Trop. 2014;62:869-76.
- [Google Scholar]
- Risk factors for dementia in a rural area of Northeastern Brazil. Arq Neuropsiquiatr. 2008;66:157-62.
- [Google Scholar]
- The Mini-Cog as a screen for dementia: Validation in a population-based sample. J Am Geriatr Soc. 2003;51:1451-4.
- [Google Scholar]
- Prevalence and pattern of cognitive impairment in rural and urban populations from Northern Portugal. BMC Neurol. 2010;10:42.
- [Google Scholar]
- The Mini Cog had high sensitivity and specificity for diagnosing dementia in community dwelling older adults. 2001. Evid Based Med. 6:159. Available from: http://www.ebm.bmj.com/content/6/5/159.full.pdf+html
- [Google Scholar]




