
Translate this page into:
Choroid Plexectomy for Hydrocephalus Management in a Pediatric Patient with a Pilocytic Astrocytoma

Reagan A. Collins, BA Department of Pediatrics, Texas Tech University Health Sciences Center SOM, 3601 4th Street, Lubbock, TX 79415 United States reagan.collins@ttuhsc.edu
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Choroid plexectomy is a debated surgical intervention for the treatment of hydranencephaly and chronic infected hydrocephalus. We present a case of a 2-year-old with multiple shunt revisions and hydrocephalus secondary to a pilocytic astrocytoma. He presented with new somnolence, vomiting, and abdominal distension 5 months post subtotal tumor resection, with a history of shunt revisions and infections related to his chemotherapy-induced low white blood cell count. He underwent choroid plexus coagulation and resection. Three years post choroid plexectomy, the patient continues to meet neurodevelopmental milestones and is shunt independent. While ventricular shunt placement is the most common course of treatment, choroid plexectomy should be considered as an alternative treatment of hydrocephalus secondary to other neurological disorders, especially when the patient is immunocompromised, to avoid the recurrent infections seen with shunt placement.
Keywords
hydrocephalus
choroid plexectomy
hydranencephaly
shunt
cerebrospinal fluid

Introduction
Choroid plexectomy is a debated surgical intervention for treatment of hydranencephaly and chronic infected hydrocephalus. The most common surgical intervention for hydrocephalus and hydranencephaly is insertion of a ventricular shunt. However, complications associated with shunts are reported in 25.7 to 36.8% of pediatric cases within the first year of surgery.1 Choroid plexectomy was first introduced by Walter Dandy in 1918, as a way to reduce cerebrospinal fluid (CSF) overproduction and manage communicating hydrocephalus.2 Since then, choroid plexectomy has been used as an alternative to shunting, particularly in patients with multiple shunt revisions or hydranencephaly.3 4 Choroid plexectomy has varied in its success, with some suggesting the intervention leads to long-term management of hydrocephalus and eventual shunt independence, while others report poor neuropsychological outcomes and low success rates.2 3 4 5 6 Here, we present a case of a 2-year-old with multiple shunt revisions and hydrocephalus secondary to a pilocytic astrocytoma treated with choroid plexus coagulation and resection.
Case Report
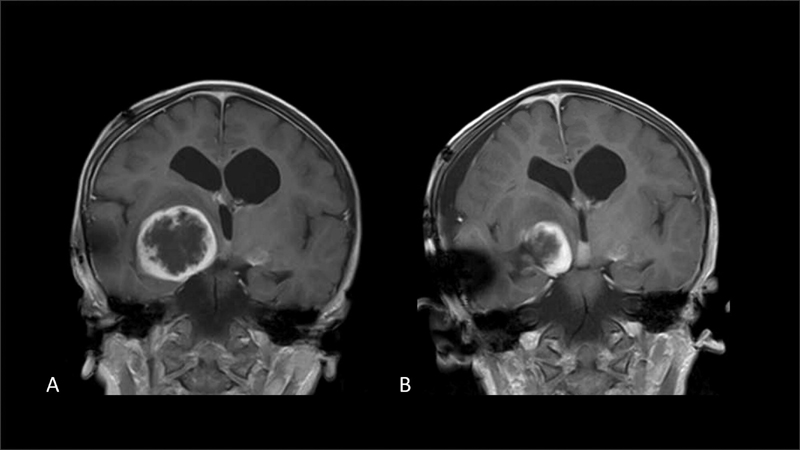
A 2-year-old boy presented to the emergency department with new somnolence, vomiting, and abdominal distension. Past medical history included macrocephaly/hydrocephalus secondary to a pilocytic astrocytoma of the right basal ganglia and optic tract. The patient underwent subtotal tumor resection five months prior and was on carboplatin and vincristine sulfate (Fig. 1A, B). He had multiple shunt revisions, each leading to ascites, pleural effusion, and infection related to his chemotherapy provoked low white blood cell (WBC) count.
-
Fig. 1 Comparison of before (A) and after (B) subtotal resection of pilocytic astrocytoma on head magnetic resonance imaging.
Fig. 1 Comparison of before (A) and after (B) subtotal resection of pilocytic astrocytoma on head magnetic resonance imaging.
On admission, the patient had abdominal ascites, and a shunt tap demonstrated shunt dysfunction with poor spontaneous flow of CSF. Later that day, the patient was taken for external ventricular drain (EVD) placement and ventriculoperitoneal (VP) shunt removal. Approximately 800 mL of ascites were drained during the surgery, and the patient was started on vancomycin and rocephin. Following surgery, the patient was at baseline, but overnight he had an increase in right frontal swelling near the EVD site. Post admission day (PAD) 2, the right temporal EVD was open to drain at 10 cm with 281 mL of clear CSF fluid over the last 24 hours and 1+ pitting edema to the forehead and scalp.
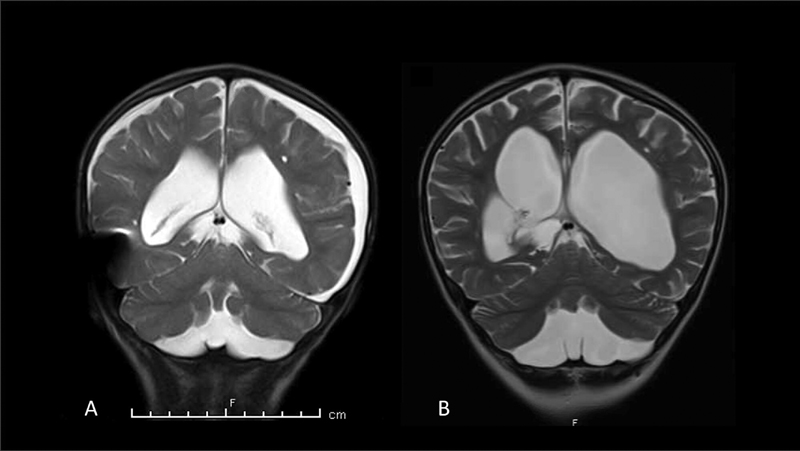
On PAD 3, he was taken for bilateral parietal craniotomy with choroid plexus coagulation and resection (Fig. 2A, B). Following coagulation surgery, he did not promptly return to baseline but remained at depressed mental status. Magnetic resonance imaging (MRI) showed stable size of the right and left temporal lesions, a slight increase in size of subdural fluid collections, and stable hydrocephalus. Post-surgical pneumocephalus was present in the frontal ventricles and subdural space. Over the next several days, his mental status improved and returned to his baseline. Repeat MRI revealed stable ventricles, and 9 days post choroid plexectomy, he was discharged home.
-
Fig. 2 Comparison of before (A) and after (B) choroid plexus coagulation on head magnetic resonance imaging.
Fig. 2 Comparison of before (A) and after (B) choroid plexus coagulation on head magnetic resonance imaging.
At his 1-week clinic follow-up, his parents reported that he seemed more alert and active, and was now walking. He was stable at his 6-week and 6-month follow-up visits. Now, 3 years post choroid plexus coagulation, he is doing well, talking, and with no major concerns. As a result of chemotherapy, the patient is currently in remission from an oncology standpoint and does not need a shunt.
Discussion
Since its introduction in 1918 for the treatment of communicating hydrocephalus,2 choroid plexectomy lost its appeal with the advent of the first ventricular shunts in the 1950s.4 Plexectomy was subject to criticism into the late 20th century. Despite literature demonstrating that experimental extirpation of the choroid plexus reduces the rate of CSF formation by up to 40%, failure was common and attributed to continued formation of CSF at extrachoroidal sites.6 Milhorat et al reported a case of a 3-week-old baby with severe communicating hydrocephalus, who underwent resection of the lateral ventricle choroid plexuses, followed by a VP shunt for progressive hydrocephalus 4 months later.6 Five years postoperation, the patient had comparable CSF production to patients without obstructed CSF pathways, which could explain the failure of choroid plexectomy in treating hydrocephalus.6
More recently, choroid plexectomy has been referenced for possible treatment of hydranencephaly and chronic hydrocephalus. However, the literature mainly consists of case reports and very few large, clinical cohort studies.4 In a chart review of nine pediatric patients with hydranencephaly, seven had complications following shunt placement which could be attributed to skin breakdown over hardware, CSF infection, CSF collection along the shunt tract, or disconnection of shunt. Four of the patients underwent choroid plexectomy to address the complications with shunting, with none requiring further neurosurgical operative intervention or readmission due to neurological issues.4 In a larger case series of 85 pediatric patients with shunt placement for hydrocephalus management, further operation was necessary on 27 occasions in 14 patients due to catheter obstruction. Choroid plexectomy was performed in seven cases, all of which left the shunt intact, and the patients experienced no further shunt obstruction.7 This is further supported by a case series at Kijabe Hospital Kenya, where the open choroid plexectomy cohort had the lowest 1 year mortality rate when compared to VP shunt, endoscopic choroid plexus coagulation, and palliative care patients, due to better visualization of the plexus and less hardware that could be infected or eroded.5 Additionally, recent studies have proposed the use of choroid plexus coagulation combined with third ventriculostomy to decrease the rate of shunt dependence in infants with hydrocephalus.8 9
In our case, the patient's hydrocephalus was secondary to a pilocytic astrocytoma. In addition to hydrocephalus, he was immunocompromised and undergoing chemotherapy. We suggest the consideration of choroid plexectomy as a viable alternative to shunt placement in patients with hydrocephalus secondary to other neurological diagnoses, including brain tumors. It can relieve the patient from the higher risk of shunt infections during the burden of chemotherapy, lead to shunt independence, and long-term positive outcomes. We recommend future studies focus on a larger cohort of patients with documentation of long-term outcomes.
Conflict of Interest
None declared.
References
- Have we made progress in preventing shunt failure? A critical analysis. J Neurosurg Pediatr. 2008;1(1):40-47.
- [Google Scholar]
- Extirpation of the choroid plexus of the lateral ventricles in communicating hydrocephalus. Ann Surg. 1918;68(6):569-579.
- [Google Scholar]
- Choroid plexectomy for the treatment of chronic infected hydrocephalus. Childs Nerv Syst. 1988;4(3):139-143.
- [Google Scholar]
- Choroid plexectomy reduces neurosurgical intervention in patients with hydranencephaly. Pediatr Neurosurg. 2002;36(3):148-152.
- [Google Scholar]
- Hydranencephaly treatments: retrospective case series and review of the literature. J Neurosurg Pediatr. 2020;26(3):228-231.
- [Google Scholar]
- Normal rate of cerebrospinal fluid formation five years after bilateral choroid plexectomy. Case report. J Neurosurg. 1976;44(6):735-739.
- [Google Scholar]
- Plexectomy as an aid in blocked ventriculo-venous shunts. Neurochirurgia (Stuttg). 1966;9(2):61-65.
- [Google Scholar]
- The importance of extent of choroid plexus cauterization in addition to endoscopic third ventriculostomy for infantile hydrocephalus: a retrospective North American observational study using propensity score-adjusted analysis. J Neurosurg Pediatr. 2017;20(6):503-510.
- [Google Scholar]
- Combined endoscopic third ventriculostomy and choroid plexus cauterization as primary treatment of hydrocephalus for infants with myelomeningocele: long-term results of a prospective intent-to-treat study in 115 East African infants. J Neurosurg Pediatr. 2008;2(5):310-316.
- [Google Scholar]




