
Translate this page into:
“Sun Burst” Appearance and “Wagon Wheel” Signs—Classical Imaging in Calvarial Hemangioma
Prasad Krishnan, MS, MCh Department of Neurosurgery, National Neurosciences Centre, Peerless Hospital Campus 360, Panchasayar, Garia–700094, Calcutta, West Bengal India prasad.krishnan@rediffmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
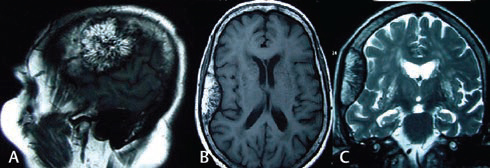
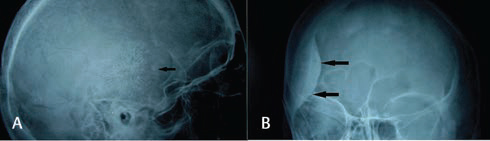
A 75-year-old lady with progressive memory loss underwent a MRI study of the brain and an incidental right temporoparietal expansile calvarial lesion was discovered. The lesion was not invading the dura or brain. The inner table of the bone was intact. The lesion was hyperintense on T1 sequences, with hypointense lines radiating outward–a typical “wagon wheel” appearance (Fig. 1A B). It was less hyperintense on T2 sequences but with the same architectural pattern. Lateral X-rays of skull showed the characteristic “sun-burst” pattern in the temporal bone (Fig. 2A) while AP X-rays showed expansion of the skull and sclerosis of the inner table (Fig. 2B). Calvarial hemangioma was diagnosed, but due to the patient’s age and lack of correlation with her symptoms, no surgical treatment was offered.
-
Fig. 1 Sagittal T1 image (A) showing hyperintense lesion with hypointense lines (trabeculae) radiating outward like the spokes of a wheel. Axial T1 image (B) showing similar findings with an intact inner table and coronal T2 image (C) showing the lesion is well-demarcated and less hypointense than in the T1 sequences.
Fig. 1 Sagittal T1 image (A) showing hyperintense lesion with hypointense lines (trabeculae) radiating outward like the spokes of a wheel. Axial T1 image (B) showing similar findings with an intact inner table and coronal T2 image (C) showing the lesion is well-demarcated and less hypointense than in the T1 sequences.
-
Fig. 2 Lateral X-ray of the skull (A) showing sunburst appearance in the temporal bone (arrow) and AP view (B) showing increased skull thickness and sclerotic inner table (arrows).
Fig. 2 Lateral X-ray of the skull (A) showing sunburst appearance in the temporal bone (arrow) and AP view (B) showing increased skull thickness and sclerotic inner table (arrows).
After the vertebrae, skull bones are the second most common site of hemangiomas.1 They account for 0.2% of all bony tumors1 2 and 10% of all benign calvarial tumors.1 2 3 The frontal and temporal bones are usually affected.2 Women are affected more commonly than men.2 3 Two variants have been described–a globular type arising from the skull base and a sessile type causing expansion of the diploic space.2 3 These benign, slow-growing lesions are mostly asymptomatic4 but may rarely present with mass effect on the brain,1 headache,3 4 cranial nerve palsies,3 seizures,3 or cosmetic disfigurement.1 3 In the majority, though, the inner table remains intact4 and may be sclerotic. Hyperintensity on T1 sequences has been described as a characteristic of this tumor2 3 and is related to the amount of “yellow marrow” (fat) in the lesion.1 3
For the greater part, they do not require any treatment, but if surgery is required, en bloc resection with cranioplasty is the treatment of choice.1 3 4 Simple curettage of the lesion is associated with a greater chance of recurrence1 and profuse hemorrhage.1 3 Radiotherapy may be used as an adjunct in cases where subtotal resection is done.1
Awareness of these typical imaging features may help in differentiating these benign lesions from other sinister pathologies such as metastases, myeloma and osteosarcoma.
Conflict of Interest
None declared.
References
- Hemangiomas in the calvaria: imaging findings. AJR Am J Roentgenol. 1995;164(3):683-687.
- [Google Scholar]
- Giant primary intraosseous calvarial hemangioma of the occipital bone. Neurol India. 2011;59(5):775-776.
- [Google Scholar]
- Cavernous hemangioma of the frontal bone: a case report. J Med Case Reports. 2014;8:121.
- [Google Scholar]




