
Translate this page into:
Fixed distance based determination of normative range of median nerve electro-diagnostic parameters

*Corresponding author: Manjusha Ashlesh Shinde, Department of Neurophysiology, All India Institute of Medical Sciences, Kalyani, West Bengal, India. manjusha.physiol@aiimskalyani.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Shaikh A, Shinde MA, Ghosh T, Patel S. Fixed distance based determination of normative range of median nerve electro-diagnostic parameters. J Neurosci Rural Pract. doi: 10.25259/JNRP_310_2024
Abstract
Objectives
Nerve conduction study is important diagnostic tool for exploring the median nerve neuropathy. This study aims to explore reference electrophysiological values for the median nerve in a sample of the East Indian population for normative data based on various anthropometric parameters and fixed distance recording among healthy adult subjects.
Materials and Methods
The study was cross-sectional at the All India Institute of Medical Sciences, Kalyani, West Bengal. After a thorough clinical evaluation, 128 hands of 64 healthy volunteers, aged between 18 and 60 years, were chosen for screening for systemic diseases or any major conditions affecting the nerves and muscles. The lengths of the arm, forearm, and wrist circumference were measured at specific reference distances. Nerve conduction studies (NCS) were carried out following standardized protocols. Motor nerve conduction data collection included median nerve distal latency, distal amplitude (DAmp), proximal latency, proximal amplitude, and conduction velocity (CV). Sensory nerve conduction data included onset latency, DAmp, and CV at 120 mm, 140 mm, and 160 mm distances from the site of stimulation. Data analysis was performed using the Statistical Package for the Social Sciences version 22.
Results
The mean and standard deviation of all parameters were calculated. NCS parameters were also determined at various percentiles. Linear regression models showed a negative link between sensory median nerve latency and increased distance from the point of stimulation. The models also provided coefficients indicating changes in NCS parameters for unit changes in body mass index (kg/m2), arm length, forearm length, and wrist circumference, individually for males and females.
Conclusion
The study identified variations in median nerve electrophysiological values, with regression models demonstrating different associations with various parameters.
Keywords
Compound motor action potential
Fixed distance recording
Median nerve
Sensory nerve action potential

INTRODUCTION
Background
The median nerve is a mixed nerve originating from the C5 to T1 roots through the medial and lateral cords of the brachial plexus. Entrapment of the median nerve can result in conditions such as carpal tunnel syndrome (CTS), anterior interosseous syndrome, and pronator teres syndrome.[1] Studies have revealed that there are almost 10 million reported cases of CTS in India, making it the most common type of neuropathy in the country.[2]
Nerve conduction studies (NCSs) are important tests used to diagnose various neuronal disorders, such as polyneuropathies, mononeuropathies, radicular lesions, tunnel syndromes, and nerve damage caused by trauma and compression. The significance of NCS in evaluating median peripheral nerve abnormalities is established, as it helps to quantify the severity of median neuropathies. Anthropometric parameters such as body mass index (BMI), arm length, and forearm length have been shown to impact nerve conduction.[3,4] These factors must be considered in clinical assessments to interpret NCSs to delineate very early accurately and with minimal change. However, there is a lack of normative data that includes analysis of electrodiagnostic parameters of the median nerve on these aspects. In this study, we aim to explore the effect of fixed distance recordings and arm length, forearm length, and wrist girth measurements on median nerve conduction parameters.
Objective
The objective of this study is to establish normative values for motor and sensory nerve conduction of the median nerve among healthy adults, utilizing fixed-distance recording for sensory nerve and to study the effect of anthropometric parameters such as BMI, arm length, forearm length, and wrist diameter on nerve conduction.
MATERIALS AND METHODS
Study design
This study was an observational analytical study.
Setting
This study was conducted at the neurophysiology laboratory of the tertiary care center in Nadia district. The study was conducted after approval from the Institutional Ethical Committee and informed written consent was obtained from all participants.
Participants and eligibility criteria
Data were collected from healthy volunteers using a convenience sample of 128 hands of 64 participants (34 males and 30 females), aged 18–60 years.
Sample size
As there are no published data on fixed distance reference normative values for the median NCS, we have taken a convenience sample size of 128 hands of 64 participants depending on the availability of healthy volunteers after necessary screening as a preliminary approach. Healthy volunteers were recruited from the general population of the Nadia district, West Bengal, using a convenience sampling technique. The participants underwent a rigorous screening process that included detailed medical histories and physical examinations to exclude any systemic, neuromuscular, or orthopedic conditions that could affect nerve conduction.
Exclusion criteria
We explicitly excluded individuals with a history of diabetes mellitus, hypothyroidism, peripheral neuropathy, CTS, or other neuromuscular disorders. In addition, participants with upper limb injuries, prior surgeries on the median nerve, or abnormal BMI values (BMI >30 kg/m2) were excluded to maintain the homogeneity of the study population.
Procedure
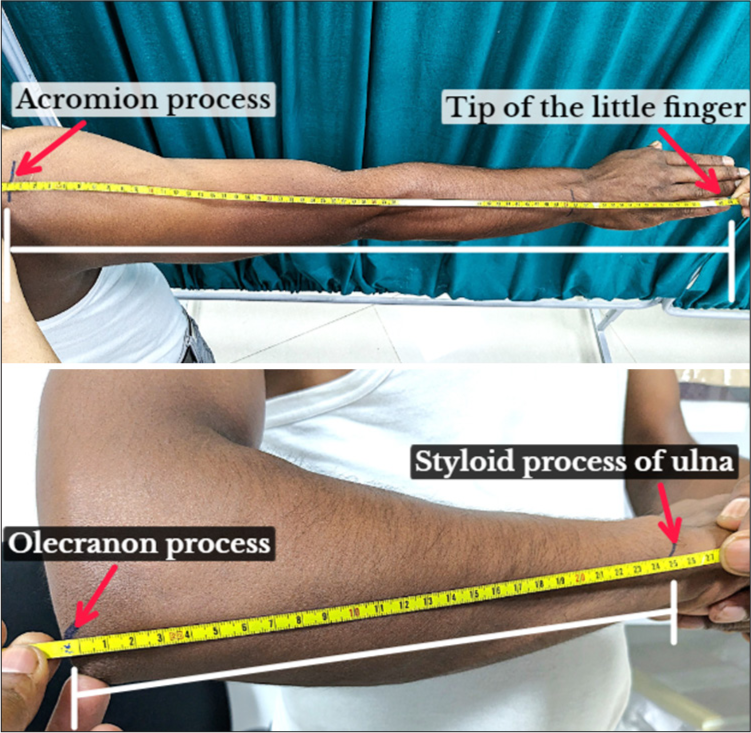
Participants underwent a thorough clinical evaluation to exclude any systemic or neuromuscular disorders. Anthropometric measurements were taken while participants stood in light clothing without shoes. Arm length and forearm length were measured following the standard anthropometric protocol. Arm length is the distance taken from the tip of the shoulder (acromion process) to the tip of the little finger in an outstretched arm, whereas forearm length is the distance taken from the proximal aspect of the olecranon process to the distal aspect of the ulnar styloid process while the hand is in a prone position with the elbow flexed at 90°, as shown in Figures 1 and 2.[3,4] Wrist diameter was measured at 120 mm,140 mm and 160 mm from the active electrode.
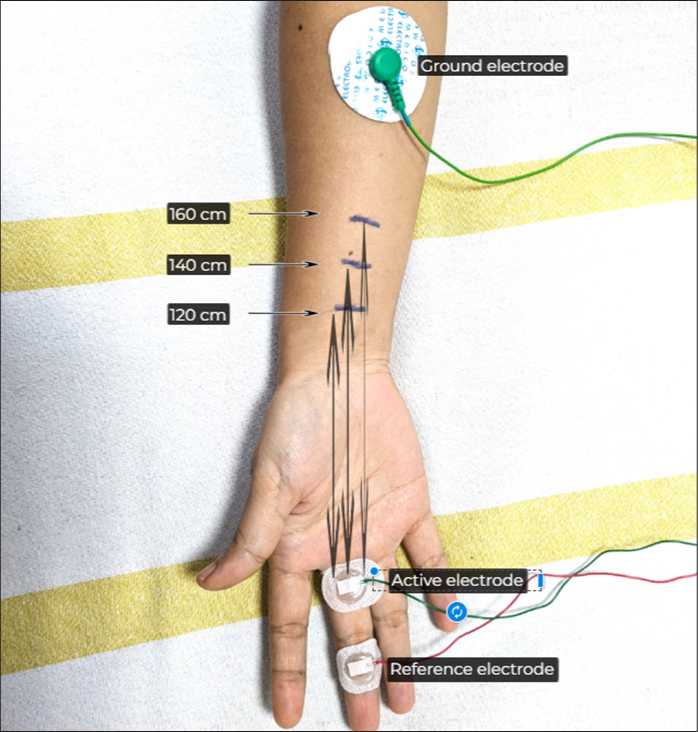
- Fixed distance for sensory nerve conduction studies stimulation taken as 120 mm, 140 mm, and 160 mm from the active electrode.
- Arm length and forearm length.
Fixed-distance measurements and arm length variability
To address variability in arm lengths, fixed distances of 120 mm, 140 mm, and 160 mm were uniformly used for sensory nerve conduction recordings. For participants with significantly different arm lengths, the elbow-to-wrist distance was proportionately adjusted, ensuring consistent electrode placement. This standardization minimizes measurement discrepancies and enhances reproducibility.
NCS procedure
The NCS was performed using a Neurosoft-MEP8 nerve conduction system in a room maintained at a constant temperature of 32°C. All tests adhered to a standardized protocol, with filters set at 10 kHz–5 Hz and a sweep speed of 4 ms per division, sensitivity at 4 mV for motor studies, and filters set at 5 Hz–2 kHz with a sweep speed of 2 ms per division, sensitivity at 10 μV for sensory studies. An average of at least 20 stimuli was used for sensory studies. The standard protocol followed the guidelines of the NCS and electromyography, Division of the Neurological Society of India Normative Data Task Force (NDTF), recommending a fixed distance between the stimulator and recording electrodes for all subjects.[5,6]
NCS parameters
Motor NCS: The distal latency (DL) and distal amplitude (DAmp) (peak to peak) were recorded following stimulation at the wrist. The proximal latency (PL) and proximal amplitude (PAmp) (peak to peak) were recorded at the elbow, and the conduction velocity (CV) was recorded between these two reference points. The Abductor Pollicis Brevis muscle was used to measure the parameters.[7,8]
Sensory NCS: Onset latency, Amplitude (peak to peak), and CV at fixed distances of 120 mm, 140 mm, and 160 mm from the stimulating electrode.[4]
The conduction was antidromic for sensory NCSs and orthodromic for motor NCSs.
Statistical analysis
All the data obtained was subjected to statistical analysis using the Statistical Package for the Social Sciences version 22 (IBM Corp., Armonk, NY, USA). All descriptive data were presented as mean and standard deviation (SD) along with the various percentile ranges. Linear regression models were used to demonstrate the association of BMI, arm length, and forearm length with NCS motor parameters and NCS sensory parameters, along with the association of BMI, arm length, forearm length, and wrist girth was also used.
RESULTS
Descriptive data
The study consisted of 64 individuals, including 34 males and 30 females. The mean age was 27.76 ± 8.6 years for males and 27.87 ± 7.13 years for females, with ages ranging from 18 to 52 years for males and 18–42 years for females. The average height was 1.67 ± 0.06 meters for males and 1.54 ± 0.06 meters for females, while the weight averaged 72.26 ± 14.22 kg for males and 58.2 ± 9.3 kg for females. The mean BMI was 25.91 ± 4.55 kg/m2 for males and 24.46 ± 3.71 kg/m2 for females, as mentioned in Table 1.
| Variable | Gender | Mean±SD | Minimum | Maximum |
|---|---|---|---|---|
| Age (years) | Male n=34 |
27.76±8.6 | 18 | 52 |
| Female n=30 |
27.87±7.13 | 18 | 42 | |
| Height (Centimeter) | Male n=34 |
1.67±0.06 | 1.52 | 1.78 |
| Female n=30 |
1.54±0.06 | 1.44 | 1.70 | |
| Weight (Kilogram) | Male n=34 |
72.26±14.22 | 43 | 104 |
| Female n=30 |
58.2±9.3 | 41 | 81 | |
| BMI (kg/m2) | Male n=34 |
25.91±4.55 | 16.38 | 36.2 |
| Female n=30 |
24.46±3.71 | 18 | 32.43 |
SD: Standard deviation, n: Sample size, BMI: Body mass index
Outcome data
Table 2 summarizes the median motor NCS parameters. For DL at the wrist, the mean was 2.58 ± 0.44 ms for females and 2.85 ± 0.45 ms for males. The DAmp was 19.7 ± 4.02 mV for females and 19.37 ± 4.23 mV for males. PL at the elbow was 6.3 ± 0.67 ms for females and 6.99 ± 0.81 ms for males. The PAmp was 18.23 ± 3.70 mV for females and 18.18 ± 4.53 mV for males. CV was 62.1 ± 4.18 m/s for females and 59.96 ± 3.49 m/s for males. The values for each parameter were compared to establish the upper and lower limits of normal, defined as the Mean ± 2 SDs (Mean ± SD).
| Motor NCS parameters | Sex# | Mean±SD | Minimum | Median | Maximum | Percentiles | ||
|---|---|---|---|---|---|---|---|---|
| 25% | 50% | 75% | ||||||
| Distal latency (Wrist) (ms) | F | 2.58±0.44 | 2.1 | 2.5 | 3.8 | 2.2 | 2.5 | 2.82 |
| M | 2.85±0.45 | 2.2 | 2.8 | 4.8 | 2.5 | 2.8 | 3.02 | |
| Distal amplitude (mV) | F | 19.7±4.02 | 12.4 | 19.7 | 30 | 16.9 | 19.3 | 21.97 |
| M | 19.37±4.23 | 10.7 | 19.37 | 30.6 | 16.08 | 19.25 | 22 | |
| Proximal latency (Elbow) (ms) | F | 6.3±0.67 | 5.1 | 6.3 | 7.9 | 5.7 | 6.15 | 6.82 |
| M | 6.99±0.81 | 3.2 | 6.99 | 9.7 | 6.6 | 7.05 | 7.5 | |
| Proximal amplitude (mV) | F | 18.23±3.70 | 10.5 | 18.23 | 28.1 | 15.5 | 17.85 | 20.52 |
| M | 18.18±4.53 | 9.2 | 18.18 | 30.5 | 15.02 | 18.15 | 20.6 | |
| Conduction velocity (m/s) | F | 62.1±4.18 | 53.50 | 62.1 | 70.8 | 59.35 | 62 | 65.4 |
| M | 59.96±3.49 | 50.8 | 59.96 | 69.7 | 57.68 | 59.5 | 61.82 | |
NCS: Nerve conduction studies, F: Female, M: Male, SD: Standard deviation, ms: Millisecond, mV: Millivolt, m/s: Meter/second, #: Female -60 hands and Male -68 hands
Table 3 presents the median sensory NCS parameters at various fixed distances from the active electrode. At 120 mm, the onset latency was 2.01 ± 0.26 ms for females and 2.02 ± 0.27 ms for males. The peak-to-peak (Amp) was 63.36 ± 19.69 μV for females and 41.19 ± 20.33 μV for males, with CV values of 61.66 ± 8.43 m/s for females and 60.88 ± 8.87 m/s for males. At 140 mm, the onset latency was 2.31 ± 0.26 ms for females and 2.33 ± 0.24 ms for males. The Amp was 74.24 ± 26.91 μV for females and 48.97 ± 23.43 μV for males, with CVs of 62.18 ± 7.2 m/s for females and 61.21 ± 5.8 m/s for males. At 160 mm, the onset latency was 2.56 ± 0.30 ms for females and 2.59 ± 0.28 ms for males. The amplitude was 57.07 ± 24.26 μV for females and 38.06 ± 18.41 μV for males, with CVs of 63.72 ± 7.41 m/s for females and 62.52 ± 6.21 m/s for males.
| Fixed distance from active electrode | Sensory NCS Parameters | Sex# | Mean±SD | Minimum | Median | Maximum | Percentiles | ||
|---|---|---|---|---|---|---|---|---|---|
| 25% | 50% | 75% | |||||||
| Distance - 120 mm | L (ms) | F | 2.01±0.26 | 1.5 | 2.0 | 2.8 | 1.8 | 2.0 | 2.13 |
| M | 2.02±0.27 | 1.3 | 2 | 3.1 | 1.9 | 2 | 2.2 | ||
| Amp (µV) | F | 63.36±19.69 | 16 | 63.7 | 96 | 49.27 | 63.7 | 77.17 | |
| M | 41.19±20.33 | 14.1 | 40.25 | 90 | 23.03 | 40.25 | 56.23 | ||
| CV (m/s) | F | 61.66±8.43 | 43.6 | 61.5 | 82.8 | 56.78 | 61.5 | 66.70 | |
| M | 60.88±8.87 | 38.7 | 60 | 96 | 55.8 | 60 | 64.9 | ||
| Distance - 140 mm | L (ms) | F | 2.31±0.26 | 1.8 | 2.25 | 2.9 | 2.1 | 2.25 | 2.5 |
| M | 2.33±0.24 | 1.8 | 2.3 | 3.2 | 2.2 | 2.3 | 2.5 | ||
| Amp (µV) | F | 74.24±26.91 | 18.7 | 72.9 | 123 | 55.03 | 72.9 | 101 | |
| M | 48.97±23.43 | 15.9 | 44.8 | 107 | 32.18 | 44.8 | 58.35 | ||
| CV (m/s) | F | 62.18±7.2 | 48.3 | 61.55 | 80 | 56.83 | 61.55 | 67.1 | |
| M | 61.21±5.8 | 43.1 | 60.9 | 77 | 57.1 | 60.9 | 65.1 | ||
| Distance- 160 mm | L (ms) | F | 2.56±0.3 | 1.9 | 2.6 | 3.2 | 2.4 | 2.6 | 2.7 |
| M | 2.59±0.28 | 1.9 | 2.5 | 3.7 | 2.4 | 2.5 | 2.7 | ||
| Amp (µV) | F | 57.07±24.26 | 15 | 54.3 | 104 | 41.95 | 54.3 | 74.25 | |
| M | 38.06±18.41 | 10.4 | 34.2 | 86 | 23.1 | 34.2 | 52.33 | ||
| CV (m/s) | F | 63.72±7.41 | 50 | 62.7 | 86.5 | 59.3 | 62.7 | 68.1 | |
| M | 62.52±6.21 | 43.2 | 64 | 74.4 | 59.3 | 64 | 66.7 | ||
NCS: Nerve conduction studies, L: Latency, AMP: Amplitude and CV: Conduction velocity, F: Female, M: Male, SD: Standard deviation, ms: Millisecond, mV: Millivolt, m/s: Meter/second, #: Female -60 hands and Male -68 hands
The Table 4 shows the results of linear regression analyses assessing the correlation between BMI, arm length, and forearm length with motor NCS parameters. For DL, a significant positive correlation was observed with arm length in males (coef. = 0.361, P = 0.002) and forearm length in females (coef. = 0.261, P = 0.04). DAmp did not show significant associations with BMI or body measurements. PL was positively correlated with arm length in both males (coef. = 0.522, P = 0.001) and females (coef. = 0.56, P = 0.001) and forearm length in both genders (males coef. = 0.317, P = 0.009; females coef. = 0.47, P = 0.001). PAmp and CV did not exhibit significant associations with BMI or body measurements.
| Motor NCS | Males (68 hands) | Female (60 hands) | ||
|---|---|---|---|---|
| Coef. (95% CI) r score | P-value | Coef. (95% CI) r score | P-value | |
| Distal latency (ms) | ||||
| BMI | 0.055 | 0.658 | 0.124 | 0.34 |
| Arm length | 0.361 | 0.002* | 0.295 | 0.022* |
| Forearm length | 0.244 | 0.045* | 0.261 | 0.04* |
| Distal amplitude (mV) | ||||
| BMI | −0.148 | 0.228 | −0.107 | 0.41 |
| Arm length | 0.094 | 0.448 | 0.059 | 0.655 |
| Forearm length | 0.057 | 0.647 | −0.009 | 0.948 |
| Proximal latency (ms) | ||||
| BMI | 0.003 | 0.979 | 0.09 | 0.45 |
| Arm length | 0.522 | 0.001* | 0.56 | 0.001* |
| Forearm length | 0.317 | 0.009* | 0.47 | 0.001* |
| Proximal amplitude (mV) | ||||
| BMI | −0.214 | 0.08 | −0.054 | 0.682 |
| Arm length | 0.069 | 0.576 | 0.018 | 0.892 |
| Forearm length | 0.106 | 0.389 | −0.067 | 0.612 |
| Conduction velocity (m/s) | ||||
| BMI | −0.201 | 0.101 | −0.071 | 0.592 |
| Arm length | −0.114 | 0.354 | −0.088 | 0.504 |
| Forearm length | −0.127 | 0.301 | −0.104 | 0.427 |
CMAP: Compound motor action potential, BMI: Body mass index, ms: Millisecond, mV: Millivolt, m/s: Meter/second, r: Correlation coefficient, P-value, P<0.05: Significant*, CI: Confidence interval, NCS: Nerve conduction studies
Table 5 presents linear regression analysis for sensory NCS parameters, including BMI, arm length, forearm length, and wrist girth. At 120 mm distance, BMI was negatively correlated with Amp in males (coef. = −0.139, P = 0.25), and wrist girth showed a significant negative correlation with Amp in males (coef. = −0.46, P = 0.001). At 140 mm, BMI was negatively correlated with Amp in both males (coef. = −0.32, P = 0.007) and females (coef. = −0.28, P = 0.03). Wrist girth also showed a significant negative correlation with Amp in males (coef. = −0.42, P = 0.001) and a non-significant correlation in females (coef. = −0.133, P = 0.313). At 160 mm, BMI was negatively correlated with Amp in males (coef. = −0.21, P = 0.07). CV showed significant associations with arm length and forearm length at different distances, but no consistent pattern was observed across distances and genders.
| Sensory NCS | Males (68 hands) | Female (60 hands) | ||
|---|---|---|---|---|
| Coef. (95% CI) r score | P-value | Coef. (95% CI) r score | P-value | |
| 120 mm | ||||
| L (ms) | ||||
| BMI | 0.184 | 0.13 | −0.07 | 0.596 |
| Arm length | −0.14 | 0.24 | 0.22 | 0.088 |
| Forearm length | −0.14 | 0.24 | 0.178 | 0.174 |
| Wrist girth | 0.08 | 0.5 | −0.196 | 0.133 |
| Amp (µV) | ||||
| BMI | −0.139 | 0.25 | 0.078 | 0.55 |
| Arm length | −0.14 | 0.228 | −0.009 | 0.94 |
| Forearm length | −0.19 | 0.119 | −0.06 | 0.65 |
| Wrist girth | −0.46 | 0.001* | −0.017 | 0.89 |
| CV (m/s) | ||||
| BMI | −0.18 | 0.12 | 0.042 | 0.74 |
| Arm length | 0.112 | 0.36 | −0.181 | 0.166 |
| Forearm length | 0.138 | 0.026* | −0.165 | 0.209 |
| Wrist girth | 0.05 | 0.67 | 0.209 | 0.115 |
| 140 mm | ||||
| L (ms) | ||||
| BMI | 0.128 | 0.29 | 0.052 | 0.694 |
| Arm length | −0.06 | 0.62 | 0.242 | 0.062 |
| Forearm length | −0.06 | 0.61 | 0.23 | 0.077 |
| Wrist girth | 0.22 | 0.06 | −0.226 | 0.082 |
| Amp (µV) | ||||
| BMI | −0.32 | 0.007* | −0.28 | 0.03* |
| Arm length | −0.08 | 0.48 | 0.303 | 0.019* |
| Forearm length | −0.15 | 0.2 | 0.175 | 0.182 |
| Wrist girth | −0.42 | 0.001* | −0.133 | 0.313 |
| CV (m/s) | ||||
| BMI | −0.09 | 0.43 | −0.078 | 0.553 |
| Arm length | 0.012 | 0.92 | −0.146 | 0.264 |
| Forearm length | −0.01 | 0.93 | −0.19 | 0.147 |
| Wrist girth | −0.09 | 0.42 | 0.183 | 0.161 |
| 160 mm | ||||
| L (ms) | ||||
| BMI | 0.10 | 0.38 | 0.075 | 0.56 |
| Arm length | −0.30 | 0.01* | 0.16 | 0.20 |
| Forearm length | −0.32 | 0.006* | 0.20 | 0.11 |
| Wrist girth | −0.07 | 0.53 | −0.14 | 0.26 |
| Amp (µV) | ||||
| BMI | −0.21 | 0.07 | −0.24 | 0.05* |
| Arm length | −0.16 | 0.17 | 0.16 | 0.22 |
| Forearm length | −0.18 | 0.13 | 0.07 | 0.58 |
| Wrist girth | −0.24 | 0.04* | −0.11 | 0.37 |
| CV (m/s) | ||||
| BMI | −0.16 | 0.17 | −0.05 | 0.69 |
| Arm length | 0.27 | 0.02* | −0.175 | 0.18 |
| Forearm length | 0.38 | 0.001* | −0.21 | 0.105 |
| Wrist girth | 0.09 | 0.45 | 0.21 | 0.102 |
L: Latency, AMP: Amplitude, CV: Conduction velocity, SNAP: Sensory nerve action potential, ms: Millisecond, µV: Microvolt, m/s: Meter/second, r: Correlation coefficient, P-value, P<0.05: Significant *, CI: Confidence interval, NCS: Nerve conduction studies, BMI: Body mass index
In summary of our Supplementary data provided, the study gives detailed data on median nerve conduction parameters, highlighting gender differences and the impact of anthropometric factors such as BMI and arm and forearm length and fixed distance for sensory study. The findings underscore the importance of considering these variables in the clinical interpretation of NCSs.
DISCUSSION
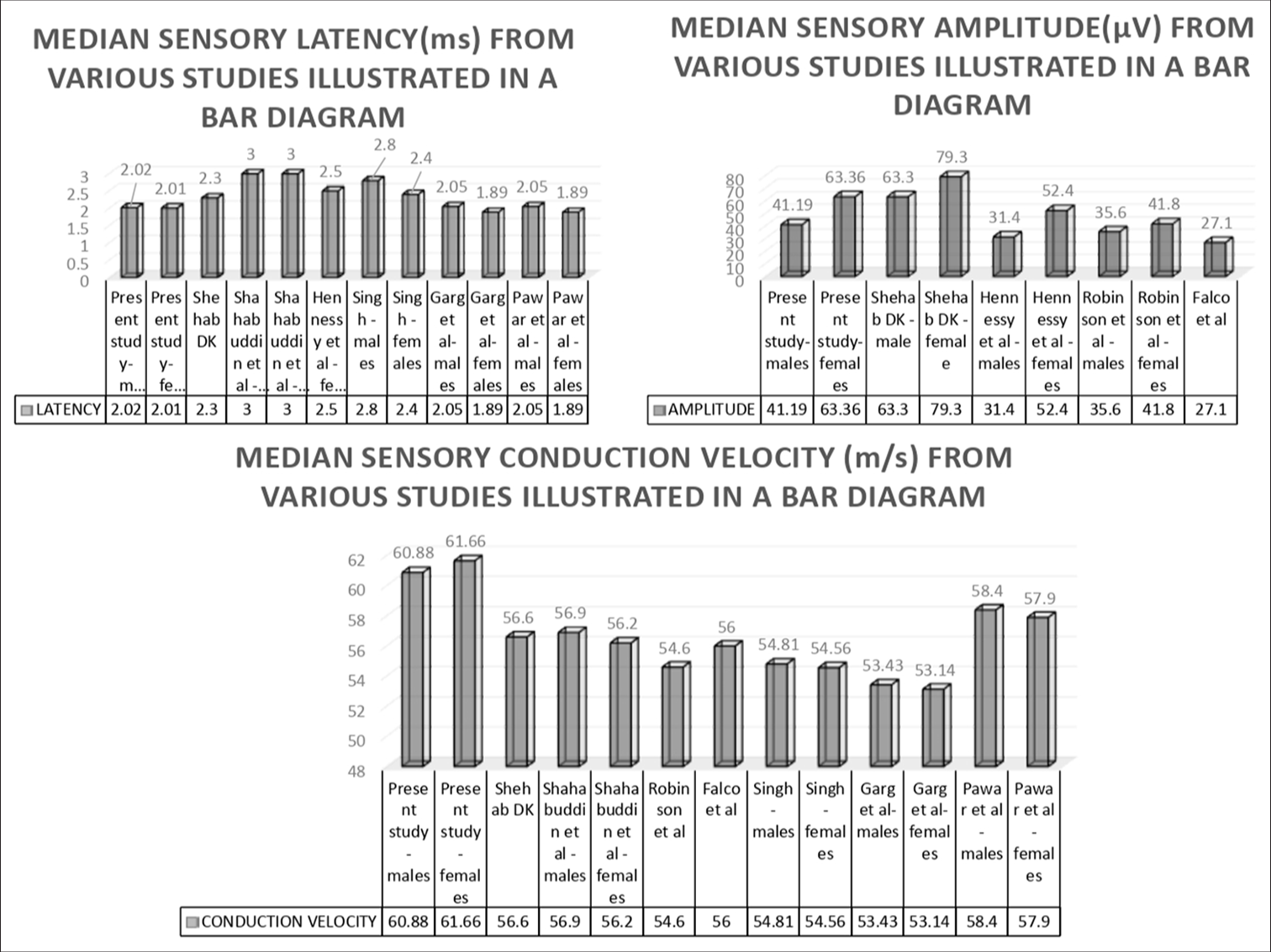
In this comprehensive discussion as mentioned in Tables 6 and 7, also represented in Figures 3 and 4, we compare the sensory and motor median nerve conduction parameters of our study with those reported in various other studies. We have focused on our objective of obtaining latency, peak-to-peak amplitude, and CV to elucidate the similarities and differences observed across different research efforts with similar variables used for measurement of NCS such as onset latency for sensory, peak-to-peak amplitude for sensory, as well as motor NCS. Our study reports mean sensory median nerve at 120 mm distance the onset latencies of 2.01 ± 0.26 ms for females and 2.02 ± 0.27 ms for males and motor median nerve DLs of 2.82 ± 2.1 ms for females and 3.02 ± 2.2 ms for males. These values are relatively low compared to those reported by Singh et al., who observed sensory latencies of 2.8 ± 0.56 ms for males and 2.4 ± 0.33 ms for females in a younger cohort.[9] In our study, the lower latencies for sensory conduction might reflect either faster conduction or differences in sample demographics. For motor latencies, our results are consistent with the higher end of the PLs reported by Kimura, Mishra, and Kalita, which were around 7.39 ± 0.69 ms and 7.62 ± 0.65 ms, respectively, compared to our findings of 6.3 ± 0.67 ms for females and 6.99 ± 0.81 ms for males.[10,11] The variations could be attributed to differences in participant age and BMI. Our study reports distal sensory nerve amplitudes of 63.36 ± 19.69 μV for females and 41.19 ± 20.33 μV for males, which are notably lower compared to those reported by Shehab, found sensory amplitudes of 63.3 ± 18.9 μV for males and 79.3 ± 28.8 μV for females.[12]
| Studies (Parameter) | Sex | Distal latency (Wrist) (ms) (Mean±SD) | Distal amplitude (mV) (Mean±SD) | Proximal latency (Elbow) (ms) (Mean±SD) | Proximal amplitude (mV) (Mean±SD) | Conduction velocity (m/s) (Mean±SD) |
|---|---|---|---|---|---|---|
| Present Study Eastern population 18–52 years of age |
F (60 hands) | 2.58±0.44 | 19.7±4.02 | 6.3±0.67 | 18.23±3.70 | 62.1±4.18 |
| M (68 hands) | 2.85±0.45 | 19.37±4.23 | 6.99±0.81 | 18.18±4.53 | 59.96±3.49 | |
| Kimura (n=61) 11–74 years of age. |
3.49±0.34 | 7.0±3.0 | 7.39±0.69 | 7.0±2.7 | 57.7±4.9 | |
| Shahabuddin et al. Aurangabad, India 27–73 years |
M (n=45) | 3.5±0.5 | - | - | - | 53.6±0.5 |
| F (n=45) | 2.8±0.7 | 53.6±0.7 | ||||
| Mishra and Kalita (n=26) 16–65 years of age. |
- | 3.77±0.40 | 8.10±2.62 | 7.62±0.65 | 7.84±2.25 | 58.52±3.76 |
| AANEM (Mean) Age 19–49 years for males and 19–39 years for female |
M | 4.6 | 5.9 | - | - | 49 |
| F | 4.4 | 4.2 | 51 | |||
| Singh et al. n=290 Punjab, India 17–21 years |
M (n=150) | 2.9±0.16 | - | - | - | 60.25±2.99 |
| F (n=140) | 2.6±0.43 | 59.83±2.82 | ||||
| Garg et al. Malwa region, India 20–60 years |
M (n=50) | 3.45±0.21 | - | - | - | 55.62±2.52 |
| F (n=40) | 3.48±0.26 | - | - | - | 55.94±2.94 | |
| Pawar et al. Central India 18–66 years |
M (n=144) | 3.3±0.48 | - | 56.3±4.6 | ||
| F (n=144) | 3.0±0.48 | - | 56.3±4.7 | |||
| Shehab Kuwait 16–56 years |
n=50 | 3.1±0.3 | 11.1±2.8 | - | - | 56.5±3.5 |
| Hennessy et al. | n=44 | 3.2±0.4 | 12.1±3.8 | - | - | 59.5±4.40 |
| Wong et al. | n=44 | 3.6±0.4 | 9.5±2.9 | - | - | 54.4±3.8 |
| Falco et al. (n=51) |
n=51 | 3.5±0.5 | 9.2±3.1 | - | - | 54.4±5.4 |
| Magladery and McDouga | n=21 | 3.2±0.4 | 12.10±3.8 | - | - | 45.1–54.4 |
| Buschbacher | n=249 | 3.7±0.5 | 10.2±3.6 | - | - | 57±5 |
ms: Millisecond, mV: Millivolt, m/s: Meter/second, SD: Standard deviation, AANEM: American association of neuromuscular and electrodiagnostic medicine, F: Female, M: Male, n: Sample size.
| Studies (Parameter) | Sex | Onset latency (ms) (Mean±SD) | Amplitude (µV) (Mean±SD) | Conduction velocity (m/s) (Mean±SD) |
|---|---|---|---|---|
| Present Study (120 mm distance) Eastern population 18–52 years of age |
M (n=34) | 2.02±0.27 | 41.19±20.33 | 60.88±8.87 |
| F (n=30) | 2.01±0.26 | 63.36±19.69 | 61.66±8.43 | |
| Shehab Kuwait 16–56 years |
M (n=50) | 2.3±0.3 | 63.3±18.9 | 56.6±7.6 |
| F (n=50) | - | 79.3±28.8 | - | |
| Shahabuddin et al. Aurangabad, India 27–73 years |
M (n=45) | 3±0.6 | - | 56.9±3.5 |
| F (n=45) | 3±0.3 | 56.2±3.4 | ||
| Hennessy et al. | M (n=44) | 2.5±0.2 | 31.4±8.2 | |
| F (n=44) | - | 52.4±14.3 | ||
| Wong et al. | M (n=44) | - | 35.6±11.8 | 54.6±3.7 |
| F (n=44) | - | 41.8±15.4 | ||
| Falco et al. (n=51) |
- | - | 27.1±11.2 | 56.0±4.5 |
| Singh et al. (2017) n=290 (17–21 years) Punjab, India |
M (n=150) | 2.8±0.56 | 54.81±3.70 | |
| F (n=140 | 2.4±0.33 | 54.56±3.65 | ||
| Garg et al. Malwa region, India 20–60 years |
M (n=50) | 2.05±0.35 | - | 53.43±3.56 |
| F (n=40) | 1.89±0.25 | - | 53.14±3.80 | |
| Pawar et al. Central India 18–66 years |
M (n=144) | 2.05±0.35 | - | 58.4±7.3 |
| F (n=144) | 1.89±0.25 | - | 57.9±6.3 |
ms: Millisecond, µV: Microvolt, m/s: Meter/second, SD: Standard deviation, F: Female, M: Male, n: Sample size.

- Median motor comparison with similar studies.
- Median sensory comparison with similar studies.
For motor nerve conduction, our study’s DAmps of 19.7 ± 4.02 mV for females and 19.37 ± 4.23 mV for males are higher than those reported by Kimura[10] (7.0 ± 2.7 mV) and Mishra and Kalita (8.10 ± 2.62).[11] However, our results are more consistent with Hennessy et al. (12.1 ± 3.8 mV) and Magladery and McDougal (12.1 ± 3.8 mV), indicating some alignment in DAmp measurements. In our study, the sensory median nerve CVs are 61.66 ± 8.43 m/s for females and 60.88 ± 8.87 m/s for males.[13,14] These values are relatively high compared to those reported by Wong et al. (54.6 ± 3.7 m/s for males) and Falco et al. (56.0 ± 4.5 m/s).[15,16] Similarly, the motor CVs reported in our study (65.4 ± 53.5 m/s for females and 61.8 ± 50.8 m/s for males) are higher than those reported by Kimura[10] (57.7 ± 4.9 m/s) and Mishra and Kalita (58.52 ± 3.76 m/s).[11] Buschbacher found PLs and CVs that are similar to our study, further supporting the validity of our findings.[17] Differences in CV measurements may reflect the importance of profiling the normative data for specific demographic areas along with consideration of participant’s age, health status, and gender. Singh et al. reported sensory CVs of 54.81 ± 3.70 m/s for males and 54.56 ± 3.65 m/s for females, which are close to our findings.[9]
In comparison with other studies like Shehab, the reported amplitude values relatively match ours. However, as latency data are not specified, direct comparisons are challenging.[12] Sensory amplitude values reported in the present study are higher than those reported by Hennessy et al.[13] Furthermore, the reported CVs are consistent with our findings, but latencies are notably different. The PLs and amplitudes reported by Wong et al. and Falco et al. and Falco et al. align closely with our results.[15,16]
The results in the present study align with findings from various demographic regions in India. Furthermore, our study delineates gender-specific differences in median nerve NCS parameters by analyzing data separately for males and females, offering a more precise application of these variations. This is especially to be taken into consideration as some disease gender difference is widely reported and accepted like CTS is more prevalent in females. Hence, gender-specific parameters will be very helpful for accurate and early diagnosis. Also selective fascicular involvement of median nerve trunk has highlighted the importance of fixed distance measurement for electro-diagnostic evaluation of median nerve neuropathy.[18] Thanakiatpinyo and Srisawasdi investigated the impact of hand size on the stimulation intensities required for median and ulnar sensory NCSs.[19] Their findings indicated that individuals with larger hand sizes necessitated higher stimulation intensities than those with smaller hands. Our study corroborates these findings, emphasizing the need to account for body measurements such as arm length, forearm length, and wrist girth when conducting NCSs.
While analyzing the fixed distance effect on sensory nerve action potential [Table 3], we found that the lowest mean onset latency was observed at 120 mm distance of recording, the highest mean amplitude was monitored at 140 mm distance of recording, and the highest CV was monitored at 160 mm distance of recording for both genders. On further regression analysis along with arm length, forearm length, and wrist girth [Table 5], we found that anthropometric parameters like wrist girth have a significant correlation with amplitude in males at 120 mm, 140 mm, and 160 mm distance recordings, while there was no significant correlation on amplitude of wrist girth in female at any distance. This may be due to thick skin and subcutaneous tissue in males compared to females, which negatively affect sensory nerve action potential. BMI has a significant negative correlation with amplitude at 140 mm distance recording in both males and females. This corroborates the fact that higher fat negatively affects sensory nerve conduction. Sensory latency was found to be negatively affected by arm length and forearm length in the case of males at 160 mm distance recording. In the case of motor nerve conduction, arm length and forearm length affect distal and PL. Further study on gender and age-wise fixed-distance recording approaches is needed to ensure accurate and consistent measurements.
Buschbacher examined the relationship between BMI and NCS results, identifying a significant correlation between BMI and sensory and mixed nerve amplitudes.[6] Their study reported that individuals with higher BMIs tended to exhibit lower nerve amplitudes compared to those with lower BMIs. Our analysis also considered BMI in relation to the standard available data, highlighting the importance of adjusting reference values for individuals with varying levels of subcutaneous body fat. The observed association between higher BMI and reduced sensory/mixed nerve amplitudes underscores the necessity of incorporating BMI considerations when interpreting NCS findings. In addition, the study suggested that increased finger thickness might correlate with lower digital sensory amplitudes, indicating the potential need for distinct NCS reference values based on body fat levels.[19] A study done by Pawar et al. in central India showed the nerve conduction parameters greater in males compared to females. Age, height, and BMI had negative effects on nerve conduction.[20] There is demographic variation in the results.[21-23] Jena and Acharya reported the onset latency prolonged in the older age group for median and ulnar nerves. The CV and Amp are less in the older age group for both nerves.[24] The American Association of Neuromuscular and Electrodiagnostic Medicine standardized data were also compared for a better understanding of confounding factors.[7] Our study confirms the presence of significant gender differences in median nerve NCS parameters, consistent with previous research documenting anatomical and physiological variations between genders and demographic areas.[25] These differences are critical for accurate diagnosis and treatment planning, emphasizing the importance of gender-specific reference values in clinical practice.
Our study provides essential insights into normative reference values for median nerve conduction in the Eastern Indian population. Anthropometric factors such as BMI, wrist girth, arm length, and forearm length significantly influence nerve conduction parameters. The negative correlation between sensory median nerve latency and increasing distance from the stimulation point underscores the value of fixed-distance recording techniques. Using distances of 120 mm, 140 mm, and 160 mm ensures consistency and comparability across individuals. BMI impacts sensory nerve action potential amplitude, with higher BMI associated with reduced amplitude due to increased subcutaneous tissue. This finding is crucial for accurate diagnosis, especially in populations with higher BMI prevalence. Wrist girth significantly influences sensory amplitude in males, likely due to differences in skin thickness and tissue composition, emphasizing the need for gender-specific reference values. In addition, limb length affects CV, with longer limbs linked to prolonged latencies. Our study offers region-specific normative data that can improve the diagnosis of peripheral neuropathies such as CTS and enhance diagnostic accuracy across diverse patient groups.
Limitations
There was a limitation of sample size. Future research should continue to explore variables to refine and standardize reference values across diverse populations, thereby improving diagnostic accuracy and clinical outcomes. As the study focused on regional reference normative value, the inclusion of different demographic areas was out of our study scope. Future studies will aim to include a larger cohort to give the normative reference data according to specific age groups and demographic variables to validate these results further.
Interpretation
Our study offers essential normative values for median nerve conduction parameters in the eastern Indian population, emphasizing using fixed distances (120 mm, 140 mm, and 160 mm) for sensory nerve conduction assessments. This approach standardizes measurements and reduces variability, enhancing consistency across studies. Our findings reveal both alignments and deviations from existing benchmarks, especially in DAmp and CV. These differences highlight the need for standardized methods and reinforce the importance of fixed distances to minimize measurement inconsistencies. The study underscores the importance of wrist girth and fixed distances in sensory NCSs for achieving accurate and reliable normative data. Laboratories should adopt standardized protocols to improve diagnostic accuracy and patient care in peripheral nerve disorders. Future research should continue using fixed distances and diverse populations to address discrepancies and advance our understanding of nerve conduction parameters.
CONCLUSION
In this study, we have explored the effect of normal anthropometric variation and fixed distance recording on median nerve conduction. We found that wrist girth, arm length, forearm length, and BMI have variable effects on sensory and motor nerve action potential. The degree of significance of the effect varies gender-wise. The findings reveal a negative correlation between sensory median nerve latency and increased distance from the stimulation point, alongside distinct regression models for males and females that highlight the impact of body measurements such as BMI, arm length, forearm length, and wrist circumference on nerve conduction parameters. These established reference values are crucial for accurate diagnosis and assessment of median nerve function in clinical practice, enhancing the ability to identify neuropathies and other related conditions in diverse populations. Such tailored normative data can improve patient outcomes by providing a more precise context for NCSs.
Generability
The establishment of normative data for the median nerve using fixed-distance recordings provides a reliable baseline for diagnosing peripheral nerve injuries and abnormalities in the Indian population. By considering factors such as gender, arm length, forearm length, wrist girth, and BMI, clinicians can achieve more accurate and individualized diagnoses. This study emphasizes the importance of developing region-specific normative data to enhance the diagnostic precision of NCS and improve patient outcomes.
Ethical approval
The research/study approved by the Institutional Review Board at All India Institute of Medical Sciences (AIIMS) Kalyani, West Bengal, number IEC/AIIMS/Kalyani/Meeting/2023/002, dated March 20, 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Nerve conduction study in healthy elderly subjects in central India: A cross-sectional study. Cureus. 2022;14:e28242.
- [CrossRef] [Google Scholar]
- Knowledge, prevalence and risk factors of carpal tunnel syndrome in young, adult and middle-aged information technology professionals. Int J Res Pharm Sci. 2020;11:1179-86.
- [CrossRef] [Google Scholar]
- Arm length measurement. 2008. Topend sports website. Available from: httpswww.topendsports.com/testing/tests/arm-length.htm [Last accessed on 2008 Jul 30]
- [Google Scholar]
- Estimation of stature from arm span, arm length, and tibial length among adolescents aged 15-18 in Addis Ababa, Ethiopia. Ethiop J Health Sci. 2021;31:1053-60.
- [CrossRef] [PubMed] [Google Scholar]
- Nerve conduction studies through landmark based recording and effects of hand length. Sci Rep. 2023;13:9962.
- [CrossRef] [PubMed] [Google Scholar]
- Body mass index effect on common nerve conduction study measurements. Muscle Nerve. 1998;21:1398-404.
- [CrossRef] [Google Scholar]
- Establishing high-quality reference values for nerve conduction studies: A report from the normative data task force of the American association of neuromuscular & electrodiagnostic medicine. Muscle Nerve. 2016;54:366-70.
- [CrossRef] [PubMed] [Google Scholar]
- Nerve conduction studies: Basic concepts. Handb Clin Neurol. 2019;160:217-24.
- [CrossRef] [PubMed] [Google Scholar]
- Normative data for median nerve conduction in healthy young adults from Punjab, India. J Neurosci Rural Pract. 2017;8:S83-8.
- [Google Scholar]
- Principles and pitfalls of nerve conduction studies. Ann Neurol. 1984;16:415-28.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical neuophysiology (2nd ed). New Delhi: B.I. Churchill Livingstone Pvt Ltd.; 1999. p. :24-9.
- [Google Scholar]
- Normative data of nerve conduction studies in the upper limb in Kuwait: Are they different from the Western data? Med Princ Pract. 1998;7:203-8.
- [CrossRef] [Google Scholar]
- Median and ulnar nerve conduction studies: Normative data for young adults. Arch Phys Med Rehabil. 1994;75:259-64.
- [CrossRef] [PubMed] [Google Scholar]
- Electrophysiological studies of nerve and reflex activity in normal man. I. Identification of certain reflexes in the electromyogram and the conduction velocity of peripheral nerve fibers. Bull Johns Hopkins Hosp. 1950;86:265-90.
- [Google Scholar]
- Comparison of assessment tools to score recovery of function after repair of traumatic lesions of the median nerve. Scand J Plast Reconstr Surg Hand Surg. 2006;40:219-24.
- [CrossRef] [PubMed] [Google Scholar]
- Standardized nerve conduction studies in the lower limb of the healthy elderly. Am J Phys Med Rehabil. 1994;73:168-74.
- [CrossRef] [PubMed] [Google Scholar]
- Mixed nerve conduction studies of the median and ulnar nerves. Am J Phys Med Rehabil. 1999;78:S69-74.
- [CrossRef] [PubMed] [Google Scholar]
- Fascicular involvement of the median nerve trunk in the upper arm: Manifestation as anterior interosseous nerve syndrome with unique imaging features. Korean J Radiol. 2024;25:449-58.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of hand size on the stimulation intensities required for median and ulnar sensory nerve conduction studies. Arch Phys Med Rehabil. 2013;94:925-9.
- [CrossRef] [PubMed] [Google Scholar]
- Normative data of upper limb nerve conduction in Central India. Indian J Physiol Pharmacol. 2011;55:241-5.
- [Google Scholar]
- Reference values for nerve function assessments among a study population in northern India-III: Sensory and motor nerve conduction. Neurol Asia. 2010;15:39-54.
- [Google Scholar]
- Effects of age, sex, and anthropometric factors on nerve conduction measures. Muscle Nerve. 1992;15:1095-104.
- [CrossRef] [PubMed] [Google Scholar]
- Normative values for nerve conduction study among healthy subjects from Aurangabad, India. Int J Recent Trends Sci Technol. 2013;8:56-61.
- [Google Scholar]
- Normative value of sensory nerve action potential of median and ulnar nerves: A cross-sectional study among healthy adults. Muller J Med Sci Res. 2022;13:40-3.
- [CrossRef] [Google Scholar]
- Nerve conduction studies in the upper limb in the Malwa region-normative data. J Clin Diagn Res. 2013;7:201-4.
- [CrossRef] [PubMed] [Google Scholar]




