
Translate this page into:
Dementia in a tribal landlocked elderly population at high altitude: What explains the lower prevalence?
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Studies across the populations have suggested that dementia is differentially distributed with a lower prevalence in developing regions than the developed ones. A comparison in the prevalence of dementia across populations may provide an insight into its risk factors. Earlier, we reported on the prevalence of dementia in elderly population in migrant, urban, rural, and tribal populations. The present study was conducted with a view to estimating the prevalence of dementia in Tribal Landlocked Elderly Population at high altitude and therefore to draw some conclusions on the differential distribution of dementia across populations.
Methods:
A cross-sectional comprehensive two-phase survey of all residents aged 60 years and older was conducted. Phase 1 involved screening of all individuals aged 60 and above with the help of a cognitive screen specifically developed for the tribal population. Phase 2 involved clinical examination of individuals who were suspected of dementia as per the developed cognitive screening test.
Results:
The results revealed that six individuals out of a total of 481 studied above 60 years of age in the studied population scored between 17 and 23, thus qualifying as suffering from mild cognitive impairment. Importantly, none of the individuals above 60 years of age scored <17.
Discussion:
The current study is in conformity with our previous study conducted on urban, rural, and migrant areas of the state of Himachal Pradesh again emphasizing on dementia being rare in tribal populations and thereby pointing to the presence of some protective factors among tribal people.
Keywords
Dementia
high altitude
prevalence
tribal

Introduction
In health and diseases research, epidemiological studies among tribal populations at high altitude open an interesting research window to understand the evolution of response of factors associated to disease causing agents.[1] Previously, we reported on the prevalence of dementia in elderly population in migrant, urban, rural, and tribal populations of Himachal Pradesh state in North India.[2] The present study was conducted with a view to estimating the prevalence of dementia in Tribal Landlocked Elderly population at high altitude and therefore to draw some conclusions on the differential distribution of dementia across populations.
The scheduled tribe population of Himachal Pradesh constitutes about 4.02% of its total population with major concentration in the districts of Kinnaur and Lahaul-Spiti and parts of the district Chamba.[3] The Kinnaur and Lahaul-Spiti districts, in their entirety, and Pangi and Bharmour (tehsil Bharmour and sub-tehsil Holi) subdivisions of Chamba district constitute the scheduled areas in the state. In our previous study, we reported on the prevalence of dementia in an elderly population Bharmour, at an altitude of 7000 feet (2134 m) with a predominant transhumant agro-pastoralist community.[4] The current study was based on a predominantly agricultural tribal population at a higher altitude.
Study area: Background
The Pangi valley is a remote, rugged, and poorly developed tribal area in Himachal Pradesh. The valley is further divided into the Saichu, Hudan Bhatori, Chasak Batori, and Sural Bhatori valleys, situated at elevations of 7000 feet (2100 m) to 12,000 feet (4000 m) above the sea level. The valley is approachable through the Saach Pass only between July end and October, which remains closed for transport by heavy snow at other times of the year.[4]
Pangi valley is distributed over 16 panchayats, 54 inhabited villages with a total population of 17,598. The villages of Pangi have seen least of in-migration and are almost entirely inhabited by local tribals.
The staple food in Pangi is barley, elo (rye), wheat, buckwheat, suil, and China (both inferior kinds of millets), most of which is locally grown. The villagers also consume wheat and rice. In addition, certain locally available grasses and roots such as kangash and chukri are also consumed. Mutton is often eaten in the winters and on special occasions.
The villagers grind barley, elo, phullan, and bres (buckwheat) and to a small extent, wheat into meal for bread which is baked into various forms. Further suil, elo, and barely are parched and then ground into flour, called Sattu, and eaten without cooking either with buttermilk, water, or tea. Locally available walnut oil and ghee are used mainly for frying vegetables and pulses. People take meals thrice a day. Villagers in Pangi use liquor extensively, which is mostly brewed locally.
Villagers also consume tea prepared from tea leaves purchased from market and Choga (tea made from local plant species).
Methods
All individuals aged 60 years and above from Pangi were the target population screened. A stratified simple random technique was used to include participants for this study. All the villages from Sural Batori valley (10,000 feet; 3048 m) and Chasak Batori valley (12,000 feet; 3658 m) were stratified to two groups of villages. Villages from each group were selected using random number table so that about 300 eligible individuals could be selected from each of the two altitude group. The aim was to screen at least 500 individuals above 60 years of age to establish a comparison with data obtained from our previous study. A higher number was chosen to account for nonwillingness of individuals to participate in the study. In the selected villages, all eligible subjects consenting to participate in the study were screened. A total of 481 individuals agreed to participate in the study, giving us a response rate of 80%. Thus, a total of 481 participants aged 60 years and above were included in this study.
Details on education, occupation, current marital status, and type of family were enquired from the all the participants. Only a full-time homemaker was regarded as a homemaker, whereas a homemaker who also worked as an agriculturist was classified as agriculturist.
Screening
In a house-to-house survey, a total of 481 individuals were identified for inclusion in this study. For the purpose of screening, a cognitive screen (Bharmouri Mental State Examination [BMSE]) was administered by a trained investigator to all 481 participants of age 60 years or above at their residence only. The cognitive screen (BMSE) has been specifically developed for screening dementia in illiterate tribal population.[5] The cutoff levels used for the purpose of classifying the severity of cognitive impairment were as follows: No cognitive impairment = 24–30; mild cognitive impairment (MCI) = 18–23; and severe cognitive impairment = 0–17.[6]
An informed written consent was obtained from each participant and next of kin was asked to provide written agreement in the event of lack of capacity to consent.
Clinical evaluation and diagnosis
The clinical evaluation was carried out by a neurologist with the help of two public health specialists. An individual was confirmed as a case of dementia only after the clinical evaluation which also included a revisit to cognitive screen scores (BMSE). The clinical team scored individuals on BMSE in a similar manner as was done by the field investigator and the score by the clinical team was taken as final.
In addition, 10% of individuals who were categorized as not having dementia on screening were also evaluated clinically. The process of selection of 10% non-demented individuals (on screening) for the clinical evaluation was similar to the process carried out for the purpose of screening for the presence of dementia.
Results
The details of the study population are provided in Table 1. The population sample consisted of 295 (61.3%) males and 185 (38.7%) females. Majority (401/485; 83%) of the participants were <75 years of age. Importantly, however a good percentage (8.3%; 40/481) of study participants was above 80 years of age pointing to a fair distribution of study participations across demographic dividend. Majority of elderly (81.4%; 392/481) participants were illiterate. Almost all (98.4%; 183/186) female participants were illiterate. Only 2 (0.7%) out of a total of 481 participants had completed graduation.
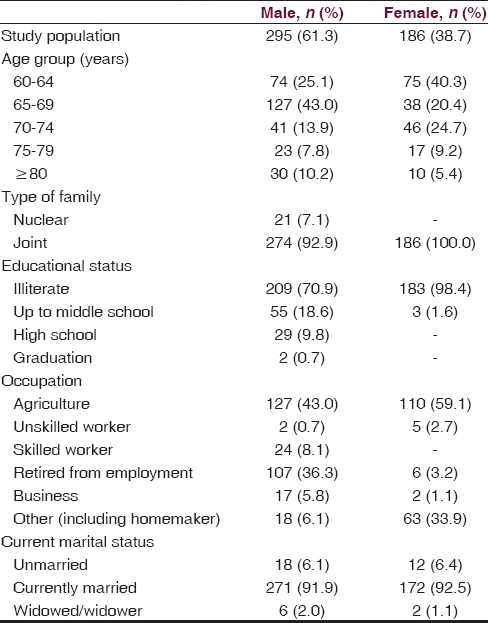
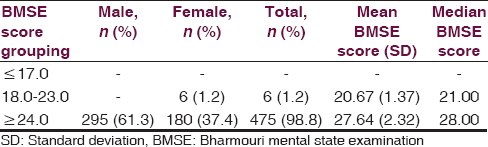
Table 2 provides a detail of the participants on Bharmouri Mental state examination (BMSE). Importantly, no individual more than 60 years of age in the population studied scored <18 on the cognitive screen. Six participants out of a total of 481 scored between 18 and 23 on cognitive screen thus were classified as cases of MCI. Two cases (2/38; 5.3%) were in the 65–69 years of age group and four cases (4/17; 23.5%) were in the 75–79 years of age group. All cases of MCI were illiterate.
Discussion
There is a scarcity of data on dementia from the least developed areas of the less developed regions of sub-Saharan Africa and South Asia. The present study based in a tribal area landlocked area of North-West India aimed the estimating prevalence of dementia in least developed areas and thereby attempt to generate a hypothesis on potential preventive factors responsible for differential distribution of dementia across populations.
A growing body of the epidemiological literature suggests that lower levels of education are associated with higher prevalence of dementia and lack of education may be a risk factor for Alzheimer's disease (AD).[7] If there is a genuine difference in risk, one would expect to find higher prevalence rates of AD in societies with lower educational levels, perhaps in pandemic proportions in populations with no formal education.[8] The present study points to the contrary. The present study population is predominantly illiterate. The present study therefore, in its findings accentuates the findings of our previous study which suggested that the differences between the prevalence rates for dementia across populations appear to be a function of a valid regional difference.
Studies in past have also suggested that societies living in isolated hilly and tribal areas seem less predisposed to dementia particularly age-related neurodegenerative and vascular dementia, which are the most common causes for dementia in elderly. This may be because some environmental risk factors are much less prevalent in these settings.
A recent study points to changes in vascular risk factors concomitant with change in prevalence of dementia without concluding on the role of education as a factor for reduction in dementia incidence, if any in recent years.[9] Another study from Switzerland suggested a link between a decline in the age-adjusted burden of amyloid deposition and changes in education levels.[10] It further reflects on the role of diet, physical activity, exposures to environmental toxins, or other unknown factors in reduction in amyloid deposition. The study is similar to the findings of data on dementia derived from Framingham Heart Study.[9]
Our studies on dementia point to similar findings. The prevalence of cardiovascular risk factors such as hypertension in this tribal area has been found to be much lower than the rural and urban areas of Himachal Pradesh thus pointing to a role of hypertension as a contributor to dementia.[1]
Importantly, the fundamental similarity between the two tribal populations studied by us and recording a lower prevalence of dementia is the presence of variety of foods such as barley, wheat, maize, and phulan as staple foods in comparison of largely wheat and rice dependent populations in rural and urban India. A similarity of our findings can be drawn with the Kashmir valley study conducted in Kuthar area of Kashmir.[11] The food habits of that population are almost similar to that of this population with an abundance of apples and walnuts. Identification of diet and environmental factors may be the key in identifying factors preventing dementia.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Prevalence of hypertension in a tribal land locked population at high altitude. Scientifica (Cairo). 2016;2016:3589720.
- [Google Scholar]
- Is dementia differentially distributed. A study on the prevalence of dementia in migrant, urban, rural, and tribal elderly population of Himalayan region in Northern India? N Am J Med Sci. 2014;6:172-7.
- [Google Scholar]
- The people and their lifestyle. In: Bharti KR, ed. Chamba Himalaya, Amazing Land, Unique Culture. New Delhi, India: Indus Publishing; 2001. p. :79-102.
- [Google Scholar]
- Identifying risk for dementia across populations: A study on the prevalence of dementia in tribal elderly population of Himalayan region in Northern India. Ann Indian Acad Neurol. 2013;16:640-4.
- [Google Scholar]
- Development of a cognitive screening instrument for tribal elderly population of Himalayan region in northern India. J Neurosci Rural Pract. 2013;4:147-53.
- [Google Scholar]
- The mini-mental state examination: A comprehensive review. J Am Geriatr Soc. 1992;40:922-35.
- [Google Scholar]
- Level of literacy and dementia: A secondary post-hoc analysis from North-West India. J Neurosci Rural Pract. 2014;5:360-2.
- [Google Scholar]
- Incidence of dementia over three decades in the Framingham Heart Study. N Engl J Med. 2016;374:523-32.
- [Google Scholar]
- Amyloid deposition is decreasing in aging brains: An autopsy study of 1,599 older people. Neurology. 2014;82:326-31.
- [Google Scholar]
- Prevalence and pattern of major neurological disorders in rural Kashmir (India) in 1986. Neuroepidemiology. 1994;13:113-9.
- [Google Scholar]




