
Translate this page into:
Blunt orbital injury causing traumatic intracranial aneurysm in a child
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Traumatic intracranial aneurysms (TICAs) are rare lesions and account for <1% of all intracranial aneurysms.[1] Their management is different from that of a spontaneous intracranial aneurysm. We hereby present a case of posttraumatic distal cortical artery aneurysm of the right frontal lobe, in a girl child, and discuss its management. Our patient was a 7-year-old girl meeting with an accident and being struck with a bicycle handlebar. The patient presented to us within 15 days of injury with the complaints of drowsiness, vomiting, and swelling of the left eye. On examination, her Glasgow Coma Scale (GCS) was 14/15, the vision was normal, and left sided eyeball movements were restricted in upgaze. Her computed tomography (CT) head revealed the intracranial hematoma along with a bony chip, as shown in Figures 1 and 2. Her CT angiogram brain showed a left-sided distal cortical artery aneurysm of a size of 12 mm × 7 mm × 5 mm and a bony chip lying beside it, as shown in Figure 3. Considering the presence of an intracerebral hemorrhage, the peripheral location of aneurysm and possibility of it being a pseudoaneurysm, patient was planned for surgical exploration, evacuation of clot, and clipping of the aneurysm.

- Noncontrast computed tomography brain showing intracerebral hematoma and bony chip
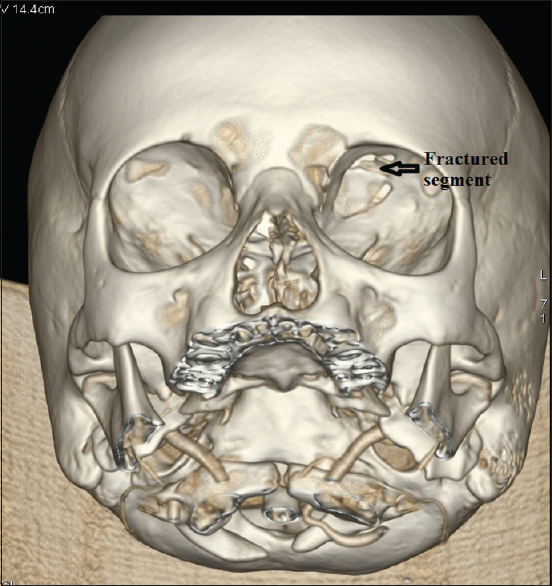
- Three-dimensional reconstruction of skull showing fractured left orbit
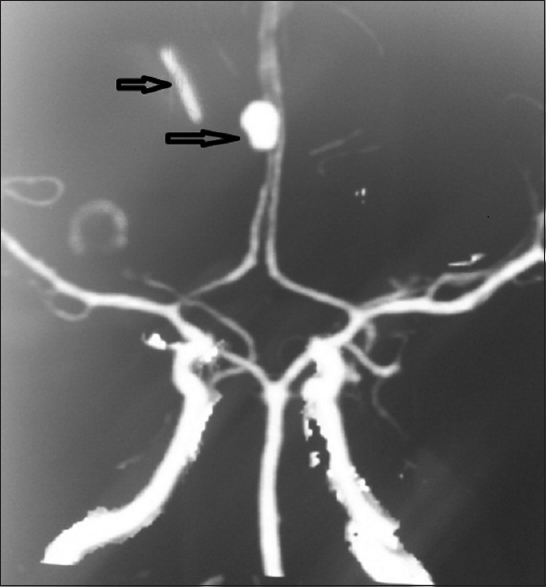
- Computed tomography angiogram brain showing aneurysm and bony chip
During surgery, we chose a right sided interhemispheric approach, evacuated the hematoma, took out the bony chip and defined the aneurysm. Intra-operatively presence of bony chip was confirmed, as shown in Figure 4. While defining, it appeared to be very thin walled and having no neck, with its origin from a big rent in the cortical branch of the left distal anterior cerebral artery. It ruptured as soon as it was handled and we had to clip the artery and excise the aneurysm. The postoperatively patient had an uneventful course, her extra-ocular movements became normal, and her 5th day CT angiogram of brain showed normal distal flow in the anterior cerebral artery. The patient was discharged with a GCS of 15/15 and no neurological deficit. Her histopathological report showed a pseudoaneurysm as shown in Figure 5.
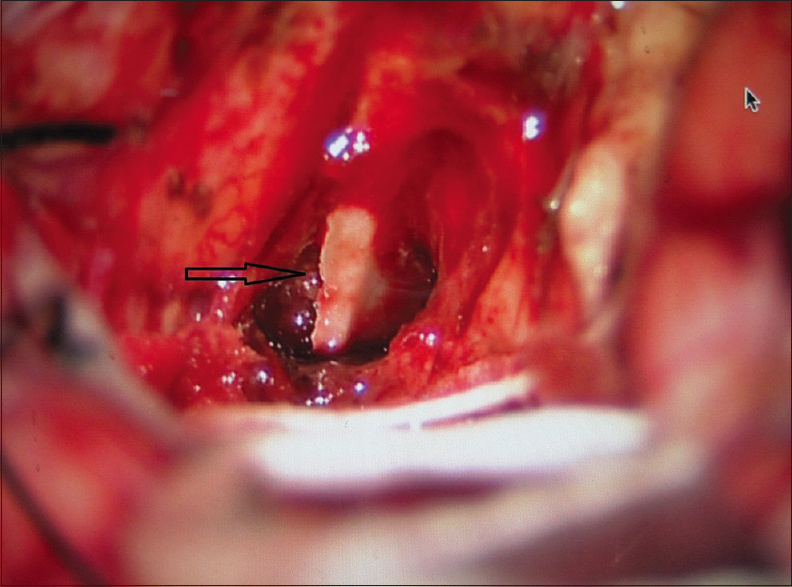
- Intra-operative picture
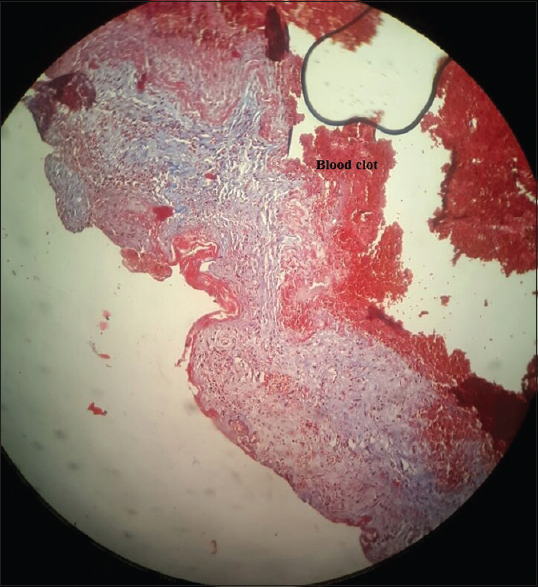
- Histopathology showing pseudoaneurysm and ruptured vessel wall
TICAs account for <1% of all intracranial aneurysms.[1] These are more common in children,[2] and may present as early as weeks to, as late as years after the injury. Classification is in many ways: Depending on mode of injury as penetrating or nonpenetrating,[2] on histology as true or false,[3] on their location in the intracranial cavity as basal or peripheral.[1] Their incidence depends on the mechanism of injury, with more risk with low velocity penetrating injuries than with high velocity penetrating injuries and blunt injuries. These aneurysms can be true, false or dissecting type with false or pseudoaneurysms being more common. Diagnosing these aneurysms require a high degree of suspicion with CT angiogram brain being a very useful screening test, and if doubt persists conventional angiography, being the gold standard, can rule out with certainty the presence or absence of any aneurysm.
In our case, the injury caused fracture of the roof of her left orbit, and the bone segment injured the distal cortical artery of left frontal lobe resulting into an aneurysm formation and intracerebral hematoma.
Angiographic features that help differentiate TICAs from congenital or spontaneous aneurysms include a poorly defined neck, irregular contour of the aneurysm, an unusual location (at a peripheral vessel rather than at a major proximal branching point), and delayed filling and emptying of the aneurysm.[45]
Treatment of these lesions depends on the signs and symptoms, location, and type of injury. All patients should undergo definitive treatment[2] since these rarely regress and have a high incidence of rupture.[2] These aneurysms generally do not have a neck[13] and thus clipping is not always possible, and excision or clipping of parent vessel should be preoperatively planned. In peripheral aneurysms their occlusion does not cause ischemia in the distal flow, and thus can be excised, however, in a basal aneurysm bypass grafting should be planned preoperatively. The presence of hematoma and friable walls favors an operative approach over an endovascular one, although reports are also available for endovascular means.[6] TICAs are rare, need a high index of suspicion to diagnose them, and good preoperative planning to treat them. All patients of traumatic subarachnoid hemorrhage either due to blunt or penetrating trauma should undergo CT angiography to complete the diagnostic workup.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Traumatic cerebral aneurysms. Clinical features and natural history. J Neurol Neurosurg Psychiatry. 1973;36:127-38.
- [Google Scholar]
- Traumatic intracranial aneurysms in childhood: Two cases and a review of the literature. Neurosurgery. 1988;22:398-408.
- [Google Scholar]
- Traumatic aneurysm of a peripheral cerebral artery. Review and case report. J Neurosurg. 1968;28:468-74.
- [Google Scholar]
- Traumatic aneurysm of the posterior inferior cerebellar artery: Case report. Neurosurgery. 1991;29:438-41.
- [Google Scholar]
- Coil embolization of intradural pseudoaneurysms caused by arterial injury during surgery: Report of two cases. AJNR Am J Neuroradiol. 2001;22:35-9.
- [Google Scholar]




