
Translate this page into:
Clinico-etiological profile of childhood stroke in a Tertiary Care Hospital in Eastern India
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
The clinical pattern and etiology of stroke may vary over time or with geographical location. In Asian countries, specific etiology and outcome of childhood stroke have been rarely reported.
Objective:
To determine the clinical and etiological pattern of childhood stroke and their outcome in a Tertiary Care Center.
Materials and Methods:
This study was conducted in a Tertiary Care Hospital of Kolkata over a period of 3 years. All children from 6 months to 12 years, diagnosed as childhood stroke by radio-imaging were included in our study. Children presenting with paraplegia/paraparesis were excluded. Etiologies were determined on the basis of clinical examination, related blood investigations and radio-imaging findings. Data gathered from the stroke patients were entered into a preformed proforma and appropriate statistical analyses were done.
Result:
Most commonly found clinical presentation was hemiparesis (70.6%). Next in place was a seizure (61.8%) and alteration of consciousness (58.8%). The most common etiology of childhood stroke in our hospital was found to be an intracranial infection (41.2%), followed by vascular etiology. Stroke was ischemic in nature in 91.2% of cases. Among the clinical features, vomiting, alteration of sensorium, and fever were significantly (P < 0.01) more in infectious cases of stroke, but hemiparesis was significantly (P < 0.05) more common in noninfectious etiology. Most of the cases of noninfectious etiology (95%) completely recovered without any persistent neurodeficit or mortality.
Conclusion:
Intracranial infection is the commonest etiology of stroke in pediatric patients presenting at our hospital. Commonest type is an ischemic stroke. The most of the patients completely recovered from the acute neurological insult after proper and timely management.
Keywords
Hemiplegia
infections
outcome
stroke

Introduction
Stroke is defined as the sudden occlusion or rupture of cerebral arteries or veins resulting in focal cerebral damage or neurological deficits.[1] Stroke in pediatric age group is not as common as in adults. Common etiologies of stroke are also different in this age group. Pediatric stroke is now recognized as an important cause of morbidity and mortality in children. The incidence of the stroke exceeds 8/100,000/year.[2] In children, the presentation of stoke is often subtle and nonspecific that can also be attributed to other neurological disorders. The rarity of the condition and paucity of signs and symptoms can cause a delay in diagnosis and initiation of treatment.[13] However, diagnosing the cause of stroke helps in providing curative treatment and appropriate preventive measures. Specific etiology and outcome of childhood stroke are less commonly reported[4] from the Asian countries. Thus, we undertook this study to determine the clinical and etiological profile and associated risk factors of childhood stroke and their outcome in a Tertiary Care Center.
Materials and Methods
This prospective study on the clinic-etiological profile of childhood stroke was carried out in the Department of Pediatric Medicine in a tertiary care hospital of Kolkata during the period of April 2010 to March 2013. Informed consent was taken from the parents and ethical clearance was taken.
All the patients’ between the age group of 6 months and 12 years admitted with signs and symptoms suggestive of stroke (hemiparesis, fever, seizure, altered consciousness, etc.,) and later diagnosed as stroke by radio-imaging during the study period were included in our study. All the patients were closely followed up during the period of hospital stay, as well as up to 6 months after discharge. Children are presenting with paraplegia/paraparesis, spinal cord/brain trauma were excluded from this study.
After admission, a detailed history was taken on a predesigned and pretested proforma. The careful clinical examination was done and recorded accordingly, including routine measurement of blood pressure and detailed examination of the neurological system. Investigations were based on the findings on history and clinical examination and included complete blood count, prothrombin time, activated partial thromboplastin time, platelets count, electrocardiogram, echocardiography, lumbar puncture with cerebrospinal fluid analysis, blood protein C and protein S analysis, high performance liquid chromatography, computed tomography scan brain, magnetic resonance imaging brain, and magnetic resonance angiography.
The outcome of these children was noted, dividing into three groups – complete recovery, persistent neurodeficit and death. Discharged patients were followed up for at least another 6 months.
All data were collected, compiled and subjected to statistical analysis with the help of SPSS software (Version 17.0; IBM). Microsoft Word and Excel 2007 were used to generate the tables, graphs etc. Categorical variables were compared in two groups with the help of Chi-square test. All tests were two-tailed. A P < 0.05 was considered as statistically significant.
Results
During the study period, 34 patients were eventually diagnosed as having childhood stroke and were included in our study.
The study population was distributed equally among the two groups above and below 5 years. There were 12 male (70.6%) and 5 female (29.4%) children in the below 5 years group, whereas 9 male (52.9%) and 8 female (47.1%) children among those aged 5 years and above. Hence, childhood stroke affected significantly (P < 0.05) higher proportion of male children than their female counterparts in case of children <5 years. Though, there was no statistical difference in sex distribution in the age group of above 5 years. The mean age of stroke patients is 5.16 ± 3.5 years and the median age is 4.75 years.
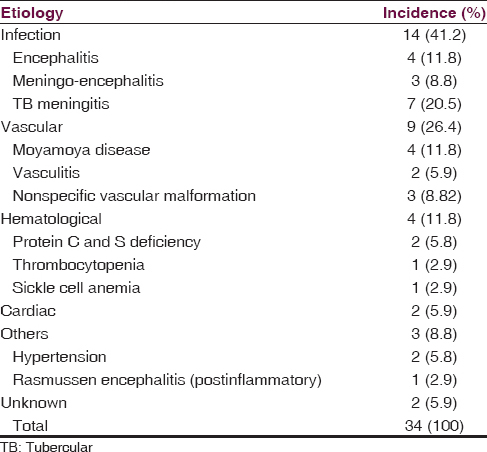
Regarding the etiologies [Table 1], intracranial infection was found to be the most common one (14 patients; 41.2%), followed by vascular (9 patients; 26.4%), hematological (4 patients; 11.8%), cardiac (2 patients; 5.9%), and others (hypertension, postinflammatory) (3 patients; 8.8%). In 2 (5.9%) patients, no etiology could be ascertained after available necessary investigations.
The most common clinical presentation of childhood stroke that we found in this study [Figure 1], was hemiparesis (24 cases [70.6%]), followed, respectively, by seizure (21 cases [61.8%]), altered consciousness (20 cases [58.8%]), both fever and cranial nerve palsy (15 cases [44.1%] each), vomiting (13 cases [38.2%]), and finally aphasia (5 cases [14.7%]).
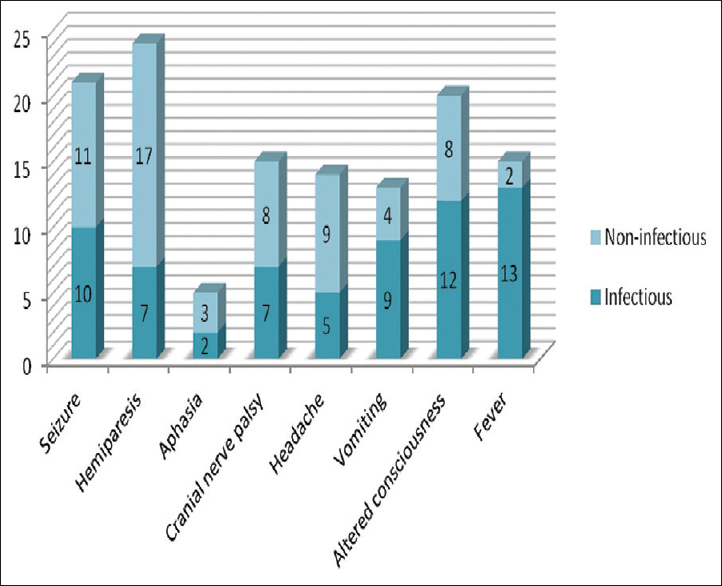
- Bar diagram showing frequency of different clinical features among the stroke patients (n = 34)
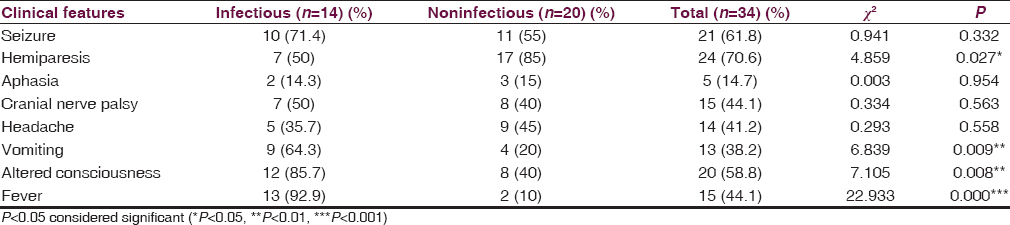
Among all the clinical features, hemiparesis was found to be significantly more common in patients with noninfectious etiology of stroke (P = 0.027). Whereas, vomiting, altered consciousness, and fever were found to be more commonly associated with infectious etiology, and the difference was statistically significant (P = 0.009, 0.008, and 0.000, respectively) [Table 2].
Among total 34 stroke patients in our study, 31 (91.2%) cases were diagnosed as ischemic stroke and 3 (8.82%) cases as a hemorrhagic stroke [Figures 2–4]. Unilateral infarctions were more common on the left side (57%) than on the right (43%).
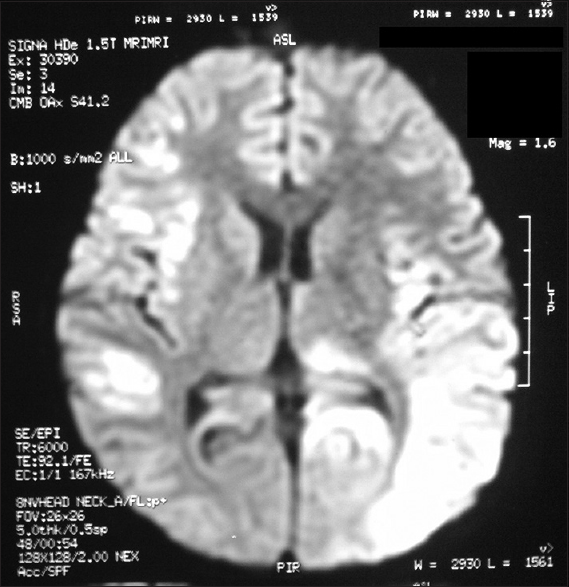
- Magnetic resonance imaging brain (T2-weighted image) of an 8-year-old male child with viral encephalitis, showing hyperintensity in bilateral cortical and subcortical white matter (left > right)
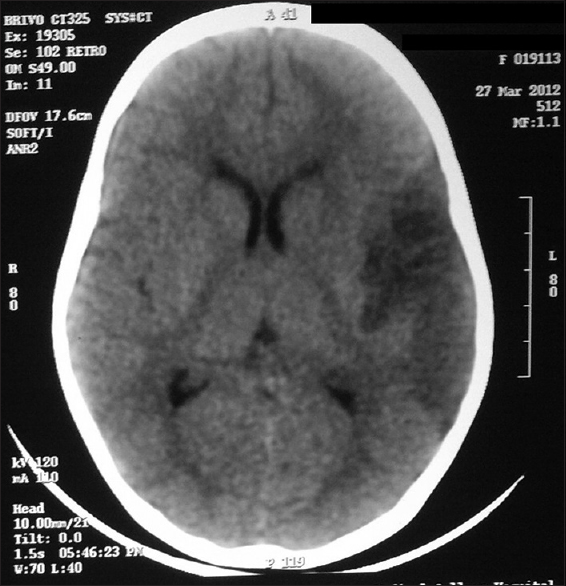
- Computed tomography scan brain of a 2½-year-old female child with Moyamoya disease showing infarction in left temporo-parietal region
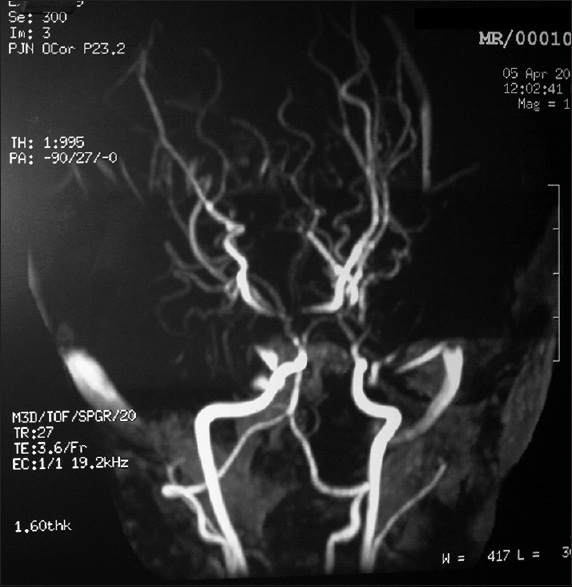
- Magnetic resonance angiography of a 2½-year-old female child with Moyamoya disease showing narrowing of supraclenoid right internal carotid artery with complete occlusion at right middle cerebral artery origin and also complete occlusion of left supraclenoid internal carotid artery and left middle cerebral artery with multiple collateral vessels around the circle of Willis supplying the occluded left middle cerebral artery territory
While analyzing the outcome, complete recovery was more frequent (95%) in patients with noninfectious etiology, whereas all of the expired patients had an infectious etiology. Hence, the outcome was significantly better in noninfectious etiology compared to infectious etiology with a P = 0.015. On the other hand, children with hemorrhagic stroke had a worse prognosis in relation to ischemic stroke patients.
Discussion
Pediatric stroke is now recognized as an important cause of morbidity and mortality. Stroke is defined as a sudden-onset, focal, neurologic deficit resulting from irreversible, focal, ischemic or hemorrhagic damage to the brain parenchyma secondary to a cerebro-vascular disorder.[5] The present study is a 3 years’ prospective study conducted in the department of Pediatric medicine in a tertiary care hospital of Kolkata, in contrast to some of the studies reported from the South-East Asian countries which were conducted as retrospective studies with more prolonged duration (10 years).[678] Though ischemic stroke is rare in children, these are more common than the hemorrhagic strokes.[3]
Totally, 34 patients of childhood stroke were admitted during the period of study. Male sex is more prevalent in our study and included 61.8% (21 boys) of total cases between 6 months and 12 years of age. However, this sex difference is more remarkable in the age group of below 5 years.
Adequate identification and determination of etiology is absolutely necessary as stroke can be prevented in some children and treated in others.[9] In the present study, intracranial infection was the most common etiology, causing stroke in 14 (41.2%) patients, and tubercular meningitis was the commonest one among them. Other etiologies found in order of frequencies are vascular (9 cases [26.4%]), hematological (4 cases [11.8%]), cardiac disorders and hypertension (2 cases [5.9%] each). In contrast to our study, studies by Lee et al.[6] showed vasculopathy (35.5%) as the commonest cause, and intracranial infection was placed 4th in frequency in their study. Another Asian study by Lee et al.[7] also showed vascular etiology (33%) as commonest and Intracranial infection was found to be next most common. A study by Siddiqui et al.[10] from Abbottabad reported Intracranial infection as the commonest etiology of stroke in their study, like ours.
Inflammatory mechanisms that accompany infections can stimulate coagulation by several pathways. These include expression of thromboplastin by monocytes and macrophages,[11] increased serum level of tumor necrosis factor which can affect pro-coagulant function of endothelium, inhibition of protein C and protein S anticoagulation systems[12] and increased levels of clotting factors like fibrinogen.[1314] Thus, there can be a significant chance of overlap between infective and vascular etiologies, as the mechanism of stroke in intracranial infection is often some form of vascular catastrophe.
In regard to clinical symptoms of stroke, we have found in our study that hemiparesis (70.6%) is the commonest presenting feature with next most common being seizure (61.8%), which was similar to the finding from study by Lee et al.[6] Vomiting, altered consciousness, and fever were found to be significantly associated with stroke patients with infectious etiologies, focal neurological deficit (hemiparesis) was mostly associated with noninfectious etiology, while other clinical presentations (e.g., Aphasia, Cranial nerve palsy, Headache) had no significant association with etiology. This type of data, relating the association of stroke symptoms with etiology is lacking in most of the Asian literature.
Hemorrhagic stroke accounts for approximately half of stroke in childhood. However, in our study, out of total 34 stroke patients, 31 (91.1%) patients were of ischemic stroke and 3 (8.82%) patients were diagnosed as a hemorrhagic stroke. This may be due to the referral of some hemorrhagic stroke patients to neurosurgery for necessary action, and thus, not being admitted to the pediatric department.
Regarding the outcome, in the study by Lee et al.,[7] neurological deficits were shown to be present in 45% of the children; the most frequent deficit was motor impairment (24%). But, in our study, complete recovery from neurodeficit was noted in most (76.5%) of the patients, whereas 8.82% patients had persistent neurodeficit and 14.7% patients died. Most of the patients, who were completely recovered from neurodeficit had noninfectious etiology of stroke and all the cases of mortality had infectious etiology. Hence, the outcome was significantly (P < 0.05) better in case of noninfectious etiology than infectious etiology. A Newer array of diagnostic facilities had helped us to diagnose the etiology as early as possible and proper management could be instituted accordingly to get a better prognosis.
Our study had a few limitations. First of all, as it is a tertiary care hospital or referral center, prevalence may be higher than the general population in this hospital-based study. Hence, the data cannot be projected to the general population, for which population-based studies are necessary. Second, a number of hemorrhagic stroke patients were less and it may be that they were referred to the neurosurgery department without admitting in our department.
To conclude, intracranial infection was the commonest cause of stroke in pediatric age group found in this study. Commonest clinical presentation was hemiparesis. Commonest type was an ischemic stroke. Most of the patients of stroke completely recovered from the acute neurological insult. With the help of newer diagnostic facilities, probability of finding an etiology of pediatric stroke is increased in cases of both noninfectious and infectious etiologies, which can greatly facilitate to adopt early and appropriate measures to decrease the chances of recurrences of stroke and also provide immediate cure for better neurological outcome.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
References
- Arterial ischemic strokes in infants and children: An overview of current approaches. Semin Thromb Hemost. 2003;29:567-73.
- [Google Scholar]
- Strokes in Thai children: Etiology and outcome. Southeast Asian J Trop Med Public Health. 1996;27:801-5.
- [Google Scholar]
- Risk factors and clinical outcomes of childhood ischemic stroke in a single Korean tertiary care center. J Child Neurol. 2012;27:485-91.
- [Google Scholar]
- Risk factors and outcomes of childhood ischemic stroke in Taiwan. Brain Dev. 2008;30:14-9.
- [Google Scholar]
- Diagnosis and treatment of ischemic pediatric stroke. Curr Neurol Neurosci Rep. 2002;2:18-24.
- [Google Scholar]
- Etiology of strokes and hemiplegia in children presenting at Ayub Teaching Hospital, Abbottabad. J Ayub Med Coll Abbottabad. 2006;18:60-3.
- [Google Scholar]
- The endotoxin-induced coagulant activity of human monocytes. Br J Haematol. 1975;30:311-6.
- [Google Scholar]
- Inflammation and coagulation: Linked processes potentially regulated through a common pathway mediated by protein C. Thromb Haemost. 1991;66:160-5.
- [Google Scholar]
- Seasonal variations of plasma fibrinogen and factor VII activity in the elderly: Winter infections and death from cardiovascular disease. Lancet. 1994;343:435-9.
- [Google Scholar]
- Immunohematologic characteristics of infection-associated cerebral infarction. Stroke. 1991;22:1004-9.
- [Google Scholar]




