
Translate this page into:
Segmental neuromyotonia
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Unilateral focal neuromyotonia has been rarely reported in fingers or extraocular muscles. We report a case of segmental neuromyotonia in a 20-year-old boy who presented to us with intermittent tightness in right upper limb. Electromyography revealed myokymic and neuromyotonic discharges in proximal as well as distal muscles of the right upper limb. Patient's symptoms responded well to phenytoin therapy. Such an atypical involvement of two contiguous areas of a single limb in neuromyotonia has not been reported previously. Awareness of such an atypical presentation of the disease can be important in timely diagnosis and treatment of a patient.
Keywords
Myokymia
myotonia
neuromyotonia

Introduction
Neuromyotonia is a rare disorder characterized by a fairly stereotyped clinical picture comprising of insidious onset muscle stiffness, continuous twitching of muscles, cramps, pseudomyotonia, pain, autonomic symptoms in the form of profuse sweating and behavioral abnormality. Mostly neuromyotonia is a generalized disorder with predominant involvement of distal extremities. However, there are reports of cases presenting with focal involvement. This focal involvement is either in the form of involvement of digits of extremities or extraocular muscles. Here we report an atypical case of a patient who had involvement of both distal and proximal regions of a single limb by neuromyotonia.
Case Report
A 20-year-old boy presented to us with intermittent tightness of the right upper limb for the last 2 years. The tightness involved both proximal and distal muscles of the right upper limb. He also complained of cramps and intermittent rippling sensations below the skin in the same limb. His complaints used to increase on voluntary activity of the limb. There was no history of difficulty in gripping objects; however, there was history of difficulty in releasing held objects. The tightness of muscles did not disappear during sleep. The patient also complained of dull aching pain in the same limb. There was no other sensory complaint. He also mentioned excessive sweating over the same limb.
On examination the patient had hypertrophy of the right arm and forearm. Myotonia was demonstrable in the right biceps and triceps on elbow flexion and extension respectively and in fingers flexors of the right upper limb. However, percussion myotonia was absent. Myokymia was also seen in the right trapezius, deltoid, biceps and triceps [Video 1]. Rest of the neurological examination was normal. Examination of other systems did not reveal any abnormality.
The nerve conduction study of the patient was normal. Electromyography revealed myokymic and neuromyotonic discharges in proximal (deltoid) and distal (first dorsal interosseous) muscles of the right upper limb, which confirmed the diagnosis of neuromyotonia [Figures 1 and 2]. Electromyography in the left deltoid, left first dorsal interosseous, bilateral vastus lateralis and bilateral tibialis anterior was normal. His routine blood investigations that included complete blood count, liver function tests, renal function tests, serum calcium, serum magnesium and random blood sugars were normal. Computed tomography of thorax was normal. Antibodies against voltage-gated potassium channels (VGKC) were not detected in serum.
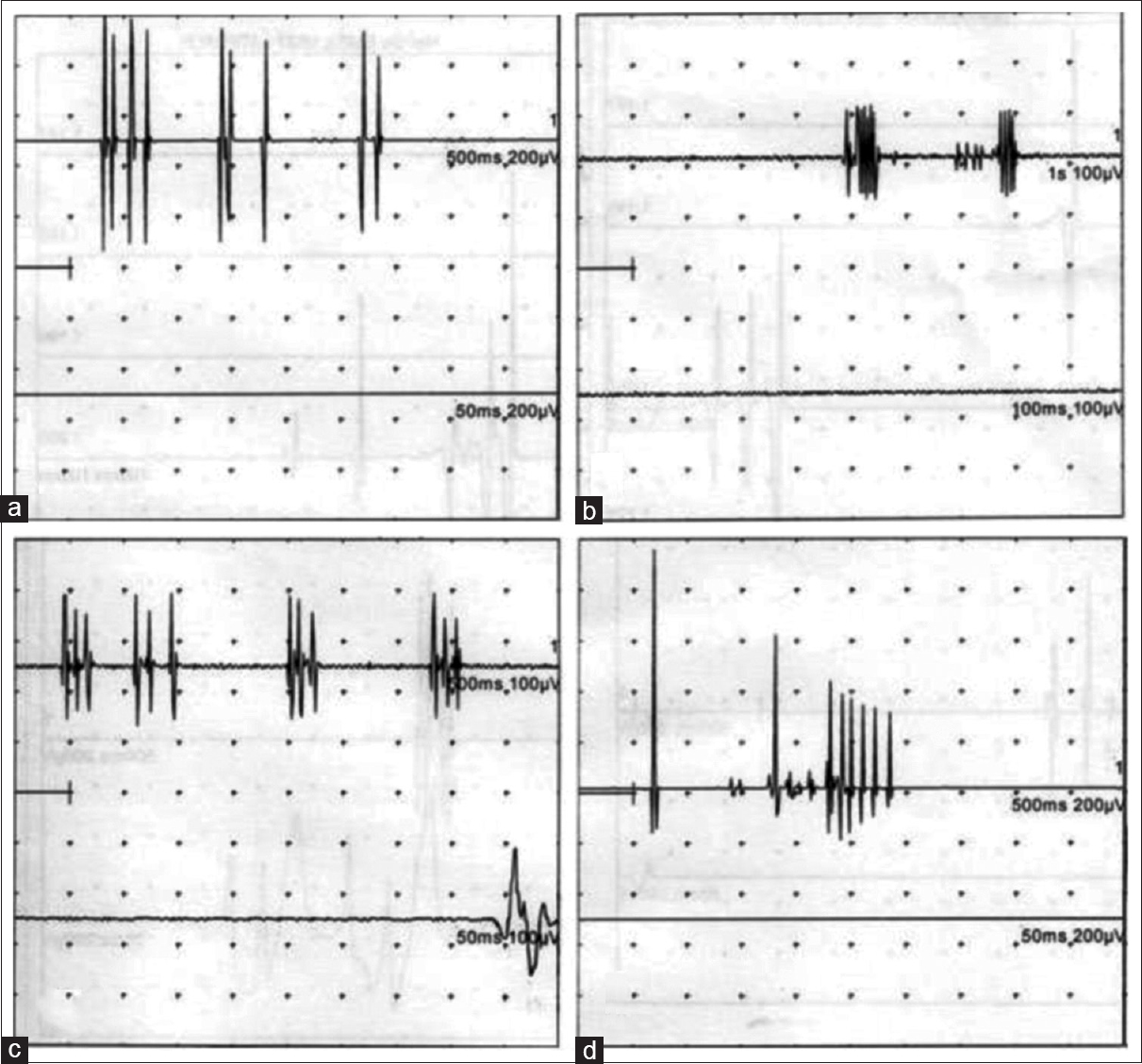
- Electromyography showing myokymic discharges (doublets, triplets and multiplets) in the right deltoid (a and b) and the right first dorsal interossea (c and d)
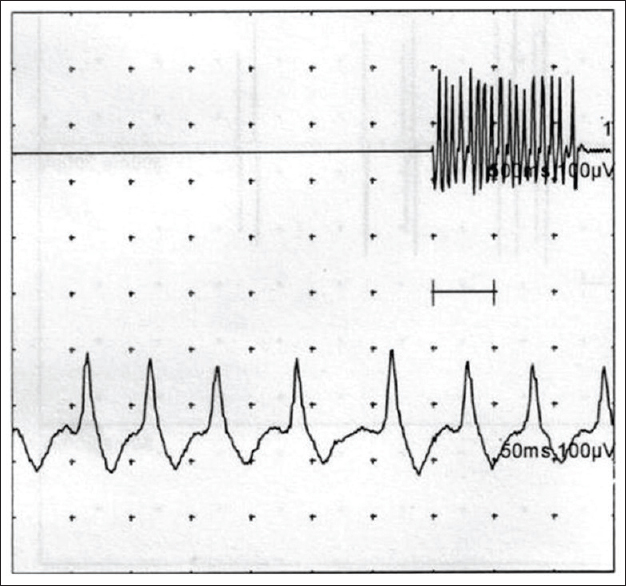
- Electromyography showing neuromyotonic discharge of frequency of around 160 Hz in the right deltoid
The patient was started on phenytoin at doses of 200 mg per day. The patient responded to the treatment and his symptoms resolved over the next few days.
Discussion
Neuromyotonia is a rare disorder characterized by a fairly stereotyped clinical picture comprising of insidious onset muscle stiffness, rippling or continuous twitching of muscles, cramps, pseudomyotonia, pain, autonomic symptoms in the form of profuse sweating and behavioral abnormality. Muscle stiffness is usually persistent, increases on voluntary activity and does not subside with sleep. The underlying pathogenesis is the abnormal peripheral nerve hyperexcitability that causes spontaneous abnormal muscle activity. It results in myokymic and neuromyotonic discharges on electromyography. On laboratory testing, VGKC antibodies can be found in around 40% cases.[1]
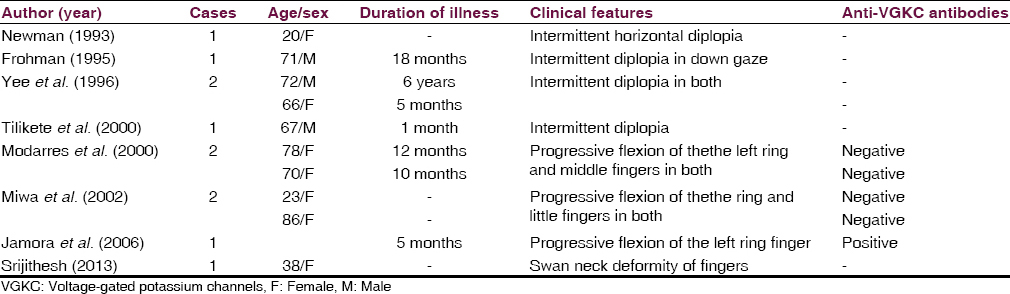
Mostly neuromyotonia is a generalized disorder with predominant involvement of distal extremities. However, there are reports of cases presenting with focal involvement. This focal involvement is either in the form of involvement of digits of extremities or extraocular muscles [Table 1].[23456789]
In our case there was involvement of both distal and proximal regions of a single limb. Such an involvement of two contiguous areas could be termed as “segmental neuromyotonia.” To the best of our knowledge, such presentation of neuromyotonia has not been reported so far. Electromyography revealed myokymic and neuromyotonic discharges in proximal as well as distal muscles of the right upper limb and did not show any abnormality in any sampled muscles of other limbs. Antibodies against VGKC were negative in our case.
Treatment of neuromyotonia consists mainly of membrane channel stabilizers like phenytoin sodium, carbamazepine, lamotrigine, topiramate, etc., Panagariya et al. have even shown the role of methylprednisolone and intravenous immunoglobulins in the treatment of neuromyotonia.[10]
Thus, we conclude that neuromyotonia can present as segmental involvement of a complete limb. Awareness of such an atypical presentation of the disease can be important in timely diagnosis and treatment of a patient.
Video on available at: www.ruralneuropractice.com
Source of Support: Nil.
Conflict of Interest: None declared.
References
- Acquired neuromyotonia following upper respiratory tract infection: A case report. Cases J. 2009;2:7952.
- [Google Scholar]
- Ocular neuromyotonia: Clinical features, physiological mechanisms, and response to therapy. Ann Neurol. 1995;37:620-6.
- [Google Scholar]
- Intermittent diplopia and strabismus caused by ocular neuromyotonia. Trans Am Ophthalmol Soc. 1996;94:207-26.
- [Google Scholar]
- Idiopathic ocular neuromyotonia: A neurovascular compression syndrome? J Neurol Neurosurg Psychiatry. 2000;69:642-4.
- [Google Scholar]
- Isolated finger flexion: A novel form of focal neuromyotonia. J Neurol Neurosurg Psychiatry. 2000;69:110-3.
- [Google Scholar]
- Isolated finger flexion caused by continuous muscle fiber activity. No To Shinkei. 2002;54:503-6.
- [Google Scholar]
- Finger flexion resembling focal dystonia in Isaacs’ syndrome. Parkinsonism Relat Disord. 2006;12:61-3.
- [Google Scholar]
- An unusual cause of swan neck deformity of the fingers. JAMA Neurol. 2013;70:263-5.
- [Google Scholar]
- Neuromyotonia: Clinical profile of twenty cases from northwest India. Neurol India. 2006;54:382-6.
- [Google Scholar]




